Diplopia evaluation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full, structured response.
Diplopia: Clinical Evaluation
1. First Step - Monocular vs. Binocular
The most important initial question: does the diplopia resolve when either eye is covered?
- Monocular diplopia - persists with one eye closed. Almost always an ocular (non-neurological) cause: corneal abnormality, uncorrected refractive error, cataract, lens dislocation, foveal traction, or rarely malingering/psychiatric disease. Test with a pinhole: diplopia from refractive error resolves; diplopia from retinal or lenticular pathology does not.
- Binocular diplopia - resolves when either eye is covered. This means ocular misalignment is present and requires systematic neurological evaluation.
- Harrison's Principles of Internal Medicine 22E, p. 278; Neuroanatomy Through Clinical Cases 3e, p. 599
2. Key Historical Features in Binocular Diplopia
Ask about:
- Direction of diplopia: purely horizontal, purely vertical, or torsional
- Gaze position that worsens it: e.g., worse looking left, worse reading/looking down
- Mode of onset: acute vs. gradual
- Intermittency and diurnal variation: worse at end of day = myasthenia gravis
- Head tilt: compensatory head posture suggests CN IV palsy
- Associated symptoms: ptosis, pain, proptosis, headache, jaw claudication, fever, weakness, ataxia
- Medical history: diabetes, hypertension, thyroid disease, cancer, MS
- Harrison's 22E, p. 278; Rosen's Emergency Medicine, p. 206
3. Structural Causes (Orbital/Restrictive Diplopia)
These are recognized by local orbital signs and a pattern that does NOT follow classic CN palsy stereotypes:
| Cause | Key Features |
|---|---|
| Thyroid eye disease (Graves) | Inferior + medial recti fibrosis; restriction of elevation and abduction; proptosis, eyelid retraction, injection |
| Orbital myositis / pseudotumor | Painful proptosis, periorbital swelling, restricted motility; mimics CN palsy but pattern atypical |
| Orbital fracture (blowout) | Trauma history; muscle entrapment (inferior rectus); worsens on upgaze |
| Orbital tumor / abscess | Gradual onset; mass effect; proptosis; may have fever if infectious |
| Giant cell arteritis | Age >50; headache, scalp tenderness, jaw claudication; ESR/CRP elevated |
Dedicated orbital imaging (MRI with fat saturation + gadolinium) is useful when the cause is not evident clinically.
- Harrison's 22E, p. 278; Rosen's Emergency Medicine, p. 206
4. Neuromuscular Cause: Myasthenia Gravis
A major cause of painless, variable, binocular diplopia - can mimic any CN palsy.
- Diplopia fluctuates, worsens with fatigue/at end of day, improves with rest
- Not confined to a single CN distribution
- Pupils always normal
- May have fatigable ptosis (unilateral or bilateral)
- ~50% of patients present with purely ocular symptoms
- Bedside ice test: apply ice to closed eyelid for 5 minutes; improvement of ptosis ~5 mm = positive (cold mitigates acetylcholinesterase inhibition)
- Labs: anti-AChR antibodies (may be negative in purely ocular form); anti-MuSK antibodies
- Beware: Botulism from food or wound poisoning can mimic ocular myasthenia
- Harrison's 22E, p. 278; Rosen's Emergency Medicine, p. 206
5. CN Palsy Patterns
Once restrictive orbitopathy and myasthenia are excluded, a cranial nerve lesion is the most likely cause.
Extraocular muscle actions by gaze position
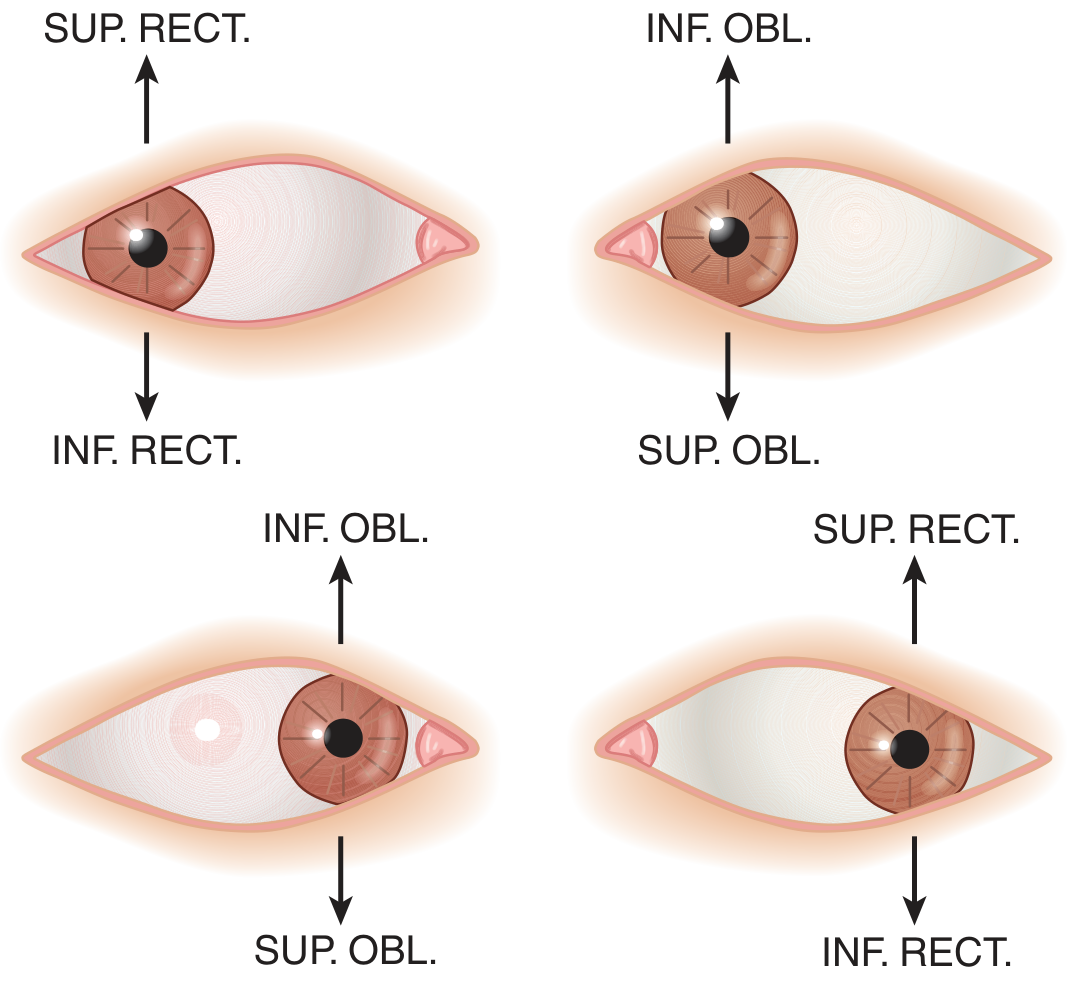
Figure: Muscles chiefly responsible for vertical movements in different gaze positions - Adams & Victor's Principles of Neurology, 12e
CN III (Oculomotor) Palsy
- Muscles affected: medial rectus, superior rectus, inferior rectus, inferior oblique, levator palpebrae, iris sphincter
- Eye position: down and out (unopposed lateral rectus + superior oblique)
- Signs: ptosis, dilated pupil (parasympathetic fibers run on the outside of the nerve = vulnerable to compression)
- Diplopia: in all directions except lateral gaze to the affected side
- Pupil-involving CN III: urgent neuroimaging + CT/MR angiogram to exclude posterior communicating artery aneurysm
- Pupil-sparing CN III: typically microvascular ischemia (diabetes, hypertension); spontaneous recovery in months
- Aberrant regeneration (lid elevates on downgaze/adduction): indicates compressive or traumatic etiology - NOT seen with microvascular CN III
Brainstem/midbrain syndromes with CN III:
- Nothnagel's: CN III + cerebellar ataxia (superior cerebellar peduncle)
- Benedikt's: CN III + contralateral tremor/chorea/athetosis (red nucleus)
- Weber's: CN III + contralateral hemiparesis (cerebral peduncle)
- Harrison's 22E, pp. 278-279
CN IV (Trochlear) Palsy
- Muscle affected: superior oblique (depresses and intorts the globe)
- Result: hypertropia + excyclotorsion of the affected eye
- Complaint: vertical diplopia, especially on reading or looking down
- Bielschowsky head tilt test (cardinal feature): diplopia worsens on tilting head toward the side of palsy, improves on tilting away
- Common causes: closed head trauma (nerve crosses at dorsal midbrain, vulnerable to tentorial impact), microvascular ischemia, congenital (review old photos for habitual head tilt)
- No aneurysmal cause expected (unlike CN III)
- Management: base-down prism; if persistent, inferior oblique weakening surgery
- Harrison's 22E, p. 279
CN VI (Abducens) Palsy
- Muscle affected: lateral rectus
- Result: failure of abduction; eye esotropic at rest
- Complaint: horizontal diplopia, worst on gaze to the side of the lesion
- Important distinction: CN VI nucleus lesion vs. fascicle lesion
- Nuclear lesion = complete ipsilateral gaze palsy (both ipsilateral LR and contralateral MR fail via MLF)
- Fascicle lesion = isolated lateral rectus weakness only
Brainstem syndromes with CN VI:
- Foville's (dorsal pons): lateral gaze palsy + ipsilateral facial palsy + contralateral hemiparesis
- Millard-Gubler (ventral pons): lateral rectus weakness only + ipsilateral facial palsy + contralateral hemiparesis
- Gradenigo's syndrome (petrous apex): mastoiditis + deafness + pain + CN VI palsy
CN VI has the longest intracranial course and is a false localizing sign in raised ICP (stretches over petrous apex).
- Harrison's 22E, p. 279
6. Internuclear Ophthalmoplegia (INO)
A supranuclear cause of diplopia from a medial longitudinal fasciculus (MLF) lesion:
- Finding: failure of adduction of one eye on horizontal gaze (with preserved adduction on convergence) + nystagmus in the abducting eye
- Cause: most commonly MS (bilateral INO = virtually pathognomonic for MS), also brainstem infarct
- In patients with MS, diplopia may be the presenting (isolated) syndrome

Figure: Left internuclear ophthalmoplegia - Harrison's Principles of Internal Medicine 22E
7. Other Important Neurological Causes
| Condition | Clue |
|---|---|
| Wernicke encephalopathy | Alcohol/malnutrition/bariatric surgery; triad of ophthalmoplegia (usually CN VI), ataxia, altered mentation |
| Miller-Fisher syndrome | Classic triad: ophthalmoplegia + ataxia + areflexia (no limb weakness) |
| Basilar meningitis | Diplopia + headache, photophobia, meningism, fever |
| Raised ICP | False-localizing CN VI palsy |
| Brainstem lacunar stroke | Crossed findings: CN palsy ipsilateral, motor/sensory deficits contralateral |
| Cavernous sinus syndrome | CN III, IV, V1/V2, VI all affected; Horner syndrome possible; causes: carotid aneurysm, cavernous sinus thrombosis, pituitary adenoma, meningioma, Tolosa-Hunt, herpes zoster |
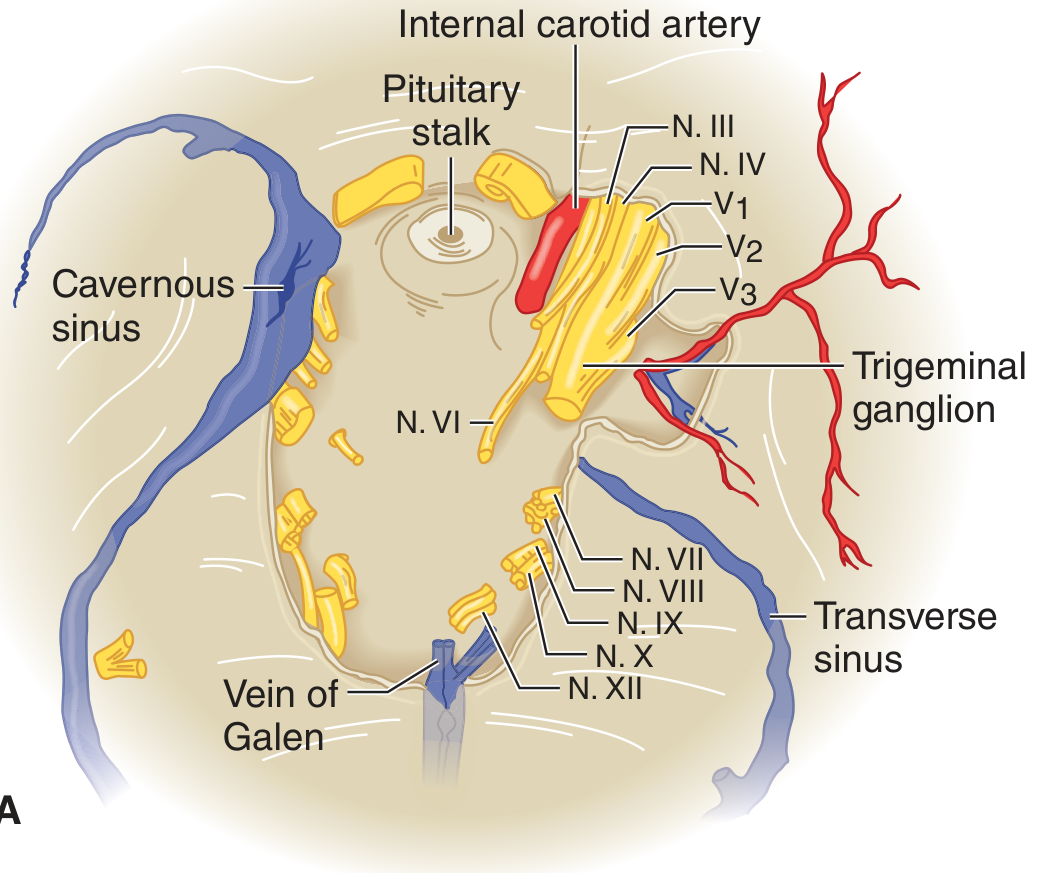
Figure: Cavernous sinus and cranial nerve relationships - Adams & Victor's Principles of Neurology, 12e
8. Bedside Examination Tools
Cover Test
- More sensitive than motility testing for subtle misalignment
- Perform in primary gaze, then with head turned/tilted in each direction fixating a distant target
- Detects comitant deviations (equal in all gaze positions = strabismus) vs. incomitant (CN palsy, restrictive)
Red Glass Test
- Place red glass over one eye (typically right); patient follows a white light in 9 gaze positions
- Reports positions of red (right eye) and white (left eye) images
- Image further from midline in the direction of attempted gaze = from the abnormal eye
Corneal Light Reflex (Hirschberg Test)
- Shine flashlight from directly in front; symmetric corneal reflections = normal
- Displaced reflection = eye misalignment
Ice Test (for Myasthenia)
- Ice pack on closed eyelid for 5 minutes
- Improvement in ptosis (~5 mm) = positive for myasthenia
- Neuroanatomy Through Clinical Cases 3e, pp. 599-600; Rosen's Emergency Medicine, p. 206
9. Ancillary Testing
| Indication | Test |
|---|---|
| Suspected myasthenia | Anti-AChR, anti-MuSK antibodies; ice test; repetitive nerve stimulation |
| Suspected thyroid eye disease | TSH, free T4, thyroid antibodies |
| Suspected GCA (age >50, headache, jaw claudication) | ESR, CRP; temporal artery biopsy if ESR >50 or CRP >20 |
| Suspected MS | Brain/spinal cord MRI with gadolinium |
| CN III with pupil involvement | CT/MR angiogram (exclude PComA aneurysm) |
| Orbital/restrictive cause | MRI orbit with fat saturation + gadolinium |
| Suspected stroke/brainstem lesion | MRI brain with DWI |
| Metabolic causes | CBC, BMP, glucose, HbA1c, B1 (thiamine if Wernicke suspected) |
- Harrison's 22E, p. 278; Rosen's Emergency Medicine, pp. 206-208
10. Diagnostic Algorithm Summary
Diplopia
|
├─ Monocular (persists with one eye closed)
│ → Ocular cause (cornea, lens, retina)
│ → Pinhole test (resolves = refractive; persists = structural)
│
└─ Binocular (resolves covering either eye)
|
├─ Signs of orbital disease (proptosis, pain, restricted motility atypical pattern)
│ → Restrictive: Thyroid, pseudotumor, fracture, tumor, GCA
│ → MRI orbit
│
├─ Variable, fatigue-related, pupils normal
│ → Myasthenia gravis
│ → Ice test, AChR antibodies, EMG
│
└─ Follows CN distribution
|
├─ CN III: Down-out eye + ptosis ± dilated pupil
│ Pupil involved → aneurysm workup (CTA/MRA)
│ Pupil spared + microvascular risk → ischemic CN III
│
├─ CN IV: Vertical diplopia, worse reading, head tilt
│ Bielschowsky test; closed head trauma common
│
├─ CN VI: Horizontal diplopia, esotropia, worse ipsilateral gaze
│ Gaze palsy → nuclear; isolated LR → fascicle
│
└─ Supranuclear / other
INO (MLF) → MS or stroke
Gaze palsy → frontal/pontine
Cavernous sinus → multiple CN (III+IV+V1+VI)
Sources: Harrison's Principles of Internal Medicine 22E; Rosen's Emergency Medicine; Adams & Victor's Principles of Neurology 12e; Neuroanatomy Through Clinical Cases 3e
This is a shared conversation. Sign in to Orris to start your own chat.