Intoduction etiology pathophysiology clinical meatures investigation and management of pcos
Reading File
Finding Sources
Finding Sources
Searching PubMed
"polycystic ovary syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive response. Let me compile this into a well-structured, detailed answer.
Polycystic Ovary Syndrome (PCOS)
1. Introduction
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder of women in reproductive age, affecting approximately 6 to 12% of this population worldwide without obvious geographic or ethnic differences. It is the leading cause of hyperandrogenism (HA), hirsutism, and anovulatory infertility in developed countries. The syndrome was first described in 1935 by Stein and Leventhal, who noted the association of amenorrhea with bilateral polycystic ovaries and obesity. More than 50% of affected women develop type 2 diabetes by age 40 years, underscoring its major metabolic impact.
- Goldman-Cecil Medicine, p. 2560; Berek & Novak's Gynecology, p. 1919
2. Etiology
PCOS is a complex multigenic disorder arising from interactions between multiple genetic and environmental factors.
Genetic Factors
- Likely polygenic/multifactorial inheritance; familial clustering is well established
- Genome-wide association studies (GWAS) have identified susceptibility loci including YAP1 (11q22.1), THADA (2p21), FSHB (11p14.1), ERBB4 (2q34), KRR1 (12q21.2), and RAD50 (5q31.1); the first four have been confirmed in both European and Han Chinese cohorts
- Candidate genes cluster into four categories:
- Insulin resistance (IR)-related genes (IRS-1, IRS-2, insulin receptor at 19p13.3)
- Genes involved in androgen biosynthesis and action (CYP17, CYP19, CYP11A)
- Genes encoding inflammatory cytokines
- Other candidate genes (SHBG, TCF7L2, FBN3/D19S884)
- Theca cells in PCOS show elevated mRNA for CYP11A, 3BHSD2, and CYP17 with corresponding overproduction of testosterone and androstenedione
Environmental Factors
-
Obesity is both a trigger and an amplifier - increasing body fat worsens hyperinsulinemia, which drives androgen excess
-
Sedentary lifestyle and caloric excess promote insulin resistance
-
PCOS may emerge or worsen in adulthood coincident with the onset of obesity
-
Berek & Novak's Gynecology, pp. 1926-1927
3. Pathophysiology
The hyperandrogenism and anovulation of PCOS involve abnormalities in four endocrinologically active compartments:
A. Ovarian Compartment (Primary)
- The ovary is the most consistent contributor of excess androgens in PCOS
- CYP17 dysregulation (the androgen-forming enzyme in both ovaries and adrenals) is a key pathogenetic mechanism
- Ovarian stroma, theca, and granulosa cells are all stimulated by elevated LH
- Total and free testosterone levels correlate directly with LH levels
- Ovaries are more sensitive to gonadotropic stimulation, possibly due to CYP17 dysregulation
- GnRH agonist treatment effectively suppresses serum testosterone and androstenedione, confirming ovarian origin
B. Hypothalamic-Pituitary Compartment
- Increased frequency (but not amplitude) of GnRH pulses from the hypothalamus
- This drives increased LH secretion relative to FSH, explaining the characteristically elevated LH:FSH ratio
- FSH is not proportionally elevated because the increased pulse frequency plus synergistic negative feedback from chronically elevated estrogen and follicular inhibin suppress FSH selectively
- ~25% of PCOS patients have mildly elevated prolactin from abnormal estrogen feedback to the pituitary
C. Insulin Resistance and Hyperinsulinemia
- Insulin resistance is a central feature, present across all racial/ethnic groups - implying a common underlying defect
- Compensatory hyperinsulinemia directly stimulates ovarian theca cell androgen production (via LH-receptor pathways)
- Insulin also suppresses hepatic sex hormone-binding globulin (SHBG) production, increasing free (bioactive) androgens
- ~1/3 of obese PCOS patients have impaired glucose tolerance (IGT); 7.5-10% have overt type 2 diabetes
- Even non-obese PCOS women have elevated rates: ~10% IGT, ~1.5% T2DM vs. 7.8% and 1% in general population respectively
D. Adrenal Compartment
- Adrenal androgens (DHEAS, DHEA) are mildly elevated in ~50% of PCOS patients
- Adrenal CYP17 dysregulation may contribute
E. Peripheral (Adipose Tissue)
- Adipose tissue converts androgens to estrogens (aromatization), creating a cycle of chronically elevated estrogen
- This sustained estrogen, without cyclic progesterone, prevents the LH surge needed for ovulation
- Increased adiposity also independently worsens insulin resistance
Ovarian Pathology
-
Macroscopically: Ovaries are 2-5x normal size, with a white thickened cortex and multiple small cysts (<1 cm)
-
Microscopically: Fibrotic, hypocellular superficial cortex; increased follicles with luteinized theca interna; stromal luteinized cells; atretic follicles
-
Berek & Novak's Gynecology, pp. 1986-1988, 1983
4. Clinical Features
Menstrual Irregularities (75-85%)
- Oligomenorrhea (cycles >35 days) is most common
- Amenorrhea (primary or secondary)
- Dysfunctional uterine bleeding (irregular, often heavy)
- Classically begins at or near menarche; may worsen with time
Hyperandrogenism
- Hirsutism (~70% in US patients): excess terminal hair in androgen-sensitive areas (upper lip, chin, chest, abdomen, inner thighs) - scored by the modified Ferriman-Gallwey scale
- Acne: often severe or treatment-resistant
- Androgenic alopecia: male-pattern hair thinning at the crown/frontal scalp
Obesity
- Present in >50% of PCOS patients
- Characteristically central/android distribution (increased waist-to-hip ratio)
- Worsens hyperinsulinemia and hyperandrogenism
Infertility
- Most common cause of anovulatory infertility
- Results from chronic anovulation
Metabolic Features
- Dyslipidemia (up to 70% prevalence): elevated triglycerides, LDL, total cholesterol; decreased HDL
- Impaired fibrinolysis: elevated plasminogen activator inhibitor (PAI-1)
- Hypertension: risk increases with age, reaching ~40% by perimenopause
- Acanthosis nigricans: velvety, hyperpigmented skin folds in the neck, axillae - marker of severe insulin resistance (HAIR-AN syndrome variant)
Psychological
- Depression in 35-40% (vs. ~10.7% in controls, even after adjusting for BMI)
- Anxiety disorders and eating disorders are also more common
Long-term Risks
-
Endometrial carcinoma: unopposed estrogen from chronic anovulation
-
~7-fold increased risk for myocardial infarction
-
Increased atherosclerosis and cardiovascular disease
-
In pregnancy: increased risk of early miscarriage, gestational diabetes, gestational hypertension, preeclampsia, and preterm birth
-
Berek & Novak's Gynecology, pp. 1951-1953; Goldman-Cecil Medicine, p. 1851
5. Diagnostic Criteria and Investigations
Diagnostic Criteria (Rotterdam 2003 - most widely used)
Two of the following three are required, after excluding other etiologies:
- Oligoovulation or anovulation
- Clinical and/or biochemical hyperandrogenism
- Polycystic ovarian morphology on ultrasound
This yields four PCOS phenotypes:
- HA + ovarian dysfunction + PCO morphology (classic, most severe)
- HA + ovarian dysfunction
- HA + PCO morphology
- Ovarian dysfunction + PCO morphology
Diagnoses to rule out (as shown in the algorithm below):
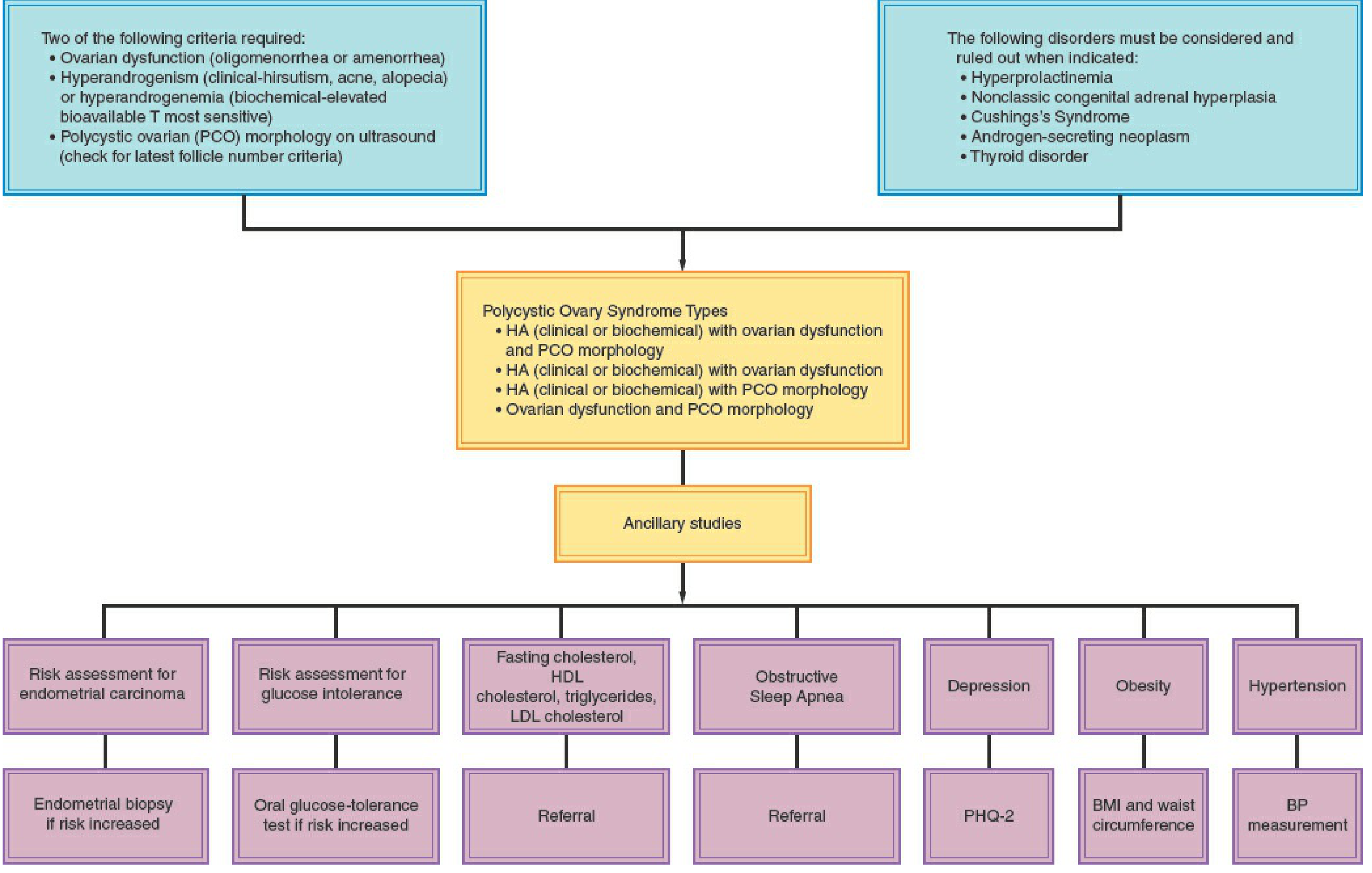
Diagnostic algorithm for PCOS showing criteria, phenotypes, and required ancillary studies. Source: Berek & Novak's Gynecology
Disorders to exclude: hyperprolactinemia, nonclassic congenital adrenal hyperplasia (NCAH), Cushing's syndrome, androgen-secreting neoplasm (adrenal or ovarian), thyroid disease, hypo-/hypergonadotropic disorders.
Investigations
Hormonal Profile:
| Test | Finding in PCOS |
|---|---|
| LH | Elevated (in ~2/3 of cases) |
| FSH | Normal or low |
| LH:FSH ratio | Often >2:1 or 3:1 |
| Total testosterone | Mildly-moderately elevated |
| Free testosterone | Elevated (most sensitive) |
| DHEAS | Elevated in ~50% |
| Androstenedione | Elevated |
| SHBG | Decreased |
| Prolactin | Mildly elevated in ~25% |
| 17-OHP (follicular phase) | To exclude NCAH (if elevated, do ACTH stimulation) |
| TSH | To exclude thyroid disease |
| Fasting cortisol / 24-hr urinary free cortisol | To exclude Cushing's |
Metabolic Screening:
- Fasting glucose and 2-hour 75-g OGTT: screening for IGT and T2DM
- Normal 2-hr glucose: <140 mg/dL
- IGT: 140-199 mg/dL
- T2DM: ≥200 mg/dL
- Fasting lipid profile: total cholesterol, HDL, LDL, triglycerides
- HbA1c: useful for chronic hyperglycemia detection
- Waist circumference and BMI at every visit
Ultrasound (Transvaginal preferred):
- PCO morphology criteria: ≥20 follicles in either ovary measuring 2-9 mm in diameter, and/or ovarian volume >10 mL
- A single ovary meeting criteria is sufficient
- Note: PCO appearance alone (without clinical/endocrine features) is found in ~23% of reproductive-age women and is not diagnostic of PCOS
Note on AMH: Anti-Mullerian hormone (AMH) reliably predicts the small antral follicle count independent of PCOS status and may be a useful adjunct marker.
- Berek & Novak's Gynecology, pp. 1934, 1966; Goldman-Cecil Medicine, p. 1857-1858
6. Management
Management must be individualized based on the patient's primary concerns: menstrual regulation, hirsutism/acne, metabolic health, or fertility.
A. Lifestyle Modification (First-Line for All)
- Weight loss of 5-10% in overweight/obese women:
- Reduces insulin levels by ~40% per 10 kg lost
- Reduces testosterone by ~35% per 10 kg lost
- Restores ovulation in >75% of women
- Improves dyslipidemia, blood pressure, and quality of life
- Exercise reduces insulin resistance independently of weight loss
- Dietary management: caloric restriction, low glycemic index diet
B. Hormonal Contraceptives (Not Desiring Pregnancy)
Combined oral contraceptive pills (COCPs) are first-line therapy for menstrual regulation and hyperandrogenism:
- Progestin component suppresses LH → reduces ovarian androgen production
- Estrogen component increases hepatic SHBG → reduces free androgens
- Directly suppresses adrenal androgen production
- Provides endometrial protection against hyperplasia and carcinoma
- Reduces hair growth in ~2/3 of hirsute patients
- Use the lowest effective estrogen dose (cyclic or continuous)
- If inadequate response after 6 months, add antiandrogens
Progestins alone (e.g., medroxyprogesterone acetate 5-10 mg orally for 10-14 days/month): protect endometrium when COCPs are contraindicated; do NOT suppress ovulation when used intermittently (contraception still required).
C. Antiandrogens (Adjunctive for Hirsutism)
Spironolactone (most commonly used):
- Mechanisms: competitive inhibition of DHT at the intracellular receptor; suppresses testosterone biosynthesis; inhibits skin 5α-reductase
- Dose: 50-100 mg twice daily (200 mg/day for maximal effect)
- 70-80% show at least modest improvement in hirsutism at ≥100 mg/day for 6 months
- Side effects: menstrual irregularity (>50% at 200 mg/day), mastodynia, hyperkalemia - monitor potassium and creatinine
- Must use contraception (theoretical risk of feminizing a male fetus)
- Combine with OCP for synergistic effect
Cyproterone acetate: synthetic progestin with potent antiandrogenic properties; competitive inhibition of testosterone/DHT at the androgen receptor; available in combination with ethinyl estradiol (Diane-35)
Flutamide: non-steroidal antiandrogen; used in some settings
5α-reductase inhibitors (Finasteride): inhibit conversion of testosterone to the more potent DHT in skin
D. Insulin Sensitizers
Metformin (1500-2000 mg/day in divided doses):
- Suppresses hepatic gluconeogenesis
- Improves insulin sensitivity
- Reduces insulin and androgen levels
- Can restore ovulation in 60-70% of affected women
- Indicated for: overweight/obese PCOS for cardiometabolic risk prevention; adjunct to diet/exercise; women with IGT or T2DM
- Not recommended as monotherapy for: endometrial protection, hirsutism treatment, ovulation induction, prevention of gestational diabetes
E. Ovulation Induction (Desiring Pregnancy)
First-line: Letrozole (aromatase inhibitor)
- 5 mg on days 3-7 of the cycle
- Superior to clomiphene in live birth rates for PCOS
- Preferred over metformin alone
Second-line: Clomiphene citrate (selective estrogen receptor modulator)
- 50 mg on days 3-7
- ~75-80% of women conceive with letrozole or clomiphene
Adjunct: Metformin - useful as an add-on with diet and exercise in obese PCOS women; can improve ovulation rates with clomiphene
Injectable Gonadotropins: used by specialists; risk of ovarian hyperstimulation syndrome (OHSS) is higher in PCOS, so careful monitoring is mandatory for monofollicular development
Surgical: Laparoscopic Ovarian Drilling (LOD)
- Multiple punctures of the ovary with diathermy or laser
- Achieves unifollicular ovulation or improves response to medical induction
- Reserved for women resistant to medical therapy
- Risk: ovarian adhesions → infertility
F. Endometrial Protection
All anovulatory PCOS women need endometrial protection:
- COCPs (preferred)
- Cyclic progestins
- Levonorgestrel-releasing IUD
G. Metabolic Syndrome Management
Screen for and manage all components:
-
Waist circumference >88 cm (F)
-
Triglycerides >150 mg/dL
-
HDL <50 mg/dL
-
Blood pressure >130/85 mmHg
-
Fasting glucose 110-126 mg/dL or 2-hr OGTT 140-199 mg/dL
-
Blood pressure measurement at every visit (target <120/80)
-
Lipid profile at baseline; repeat every 2 years or sooner with weight gain
-
Screening for obstructive sleep apnea if appropriate
-
Vitamin D assessment and supplementation when deficient
H. Psychological Support
- Screen for depression (PHQ-2 as initial screen), anxiety, and eating disorders at diagnosis and regularly
- Lifestyle modification programs improve depression and quality of life
Summary Table
| Feature | Detail |
|---|---|
| Prevalence | 6-12% of reproductive-age women |
| Diagnosis | Rotterdam 2003 (2 of 3 criteria) |
| First-line (no pregnancy desired) | COCP + lifestyle modification |
| First-line (ovulation induction) | Letrozole > clomiphene |
| Insulin sensitizer | Metformin 1500-2000 mg/day |
| Antiandrogen for hirsutism | Spironolactone 50-200 mg/day |
| Key metabolic risk | T2DM (>50% by age 40), CVD, endometrial cancer |
| Surgical option | Laparoscopic ovarian drilling (refractory cases) |
Recent Evidence Update (2024-2025)
Recent meta-analyses highlight evolving management approaches:
- GLP-1 receptor agonists (e.g., semaglutide, liraglutide) show efficacy for weight loss and hormonal regulation in obese PCOS women - a meta-analysis of RCTs (PMID 39178623, 2024) supports their use as an emerging option
- Lifestyle interventions remain cornerstone therapy - a 2025 systematic review (PMID 39861440) confirms comprehensive lifestyle management significantly improves reproductive and metabolic outcomes
- Pregnancy outcomes in PCOS remain worse than controls even with treatment - a 2024 meta-analysis (PMID 38965226) found increased risks of gestational diabetes, preeclampsia, and preterm birth, reinforcing the need for preconception counseling
Sources: Goldman-Cecil Medicine International Edition (9780323930345), Berek & Novak's Gynecology (9781496380357), Harrison's Principles of Internal Medicine 22E (9781265977061), and current PubMed evidence (2024-2025).
This is a shared conversation. Sign in to Orris to start your own chat.