Hemoptysis
Reading File
Finding Sources
Searching PubMed
hemoptysis causes management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from 5 authoritative textbooks. Let me compose the full clinical answer.
Hemoptysis
Definition: Hemoptysis is the expectoration of blood originating from the tracheobronchial tree or pulmonary parenchyma. The volume ranges from blood-streaked sputum to massive life-threatening hemorrhage. - Murray & Nadel's Textbook of Respiratory Medicine
Distinguishing Hemoptysis from Mimics
Before evaluating hemoptysis, confirm the source:
| Feature | Hemoptysis | Hematemesis | Epistaxis |
|---|---|---|---|
| Color | Bright red | Dark, coffee-ground | From nose |
| pH | Alkaline | Acidic | N/A |
| Consistency | Frothy, mixed with sputum | Contains food particles | Posterior drip |
| Macrophages | Hemosiderin-laden macrophages present | Absent | Absent |
| Associated symptoms | Cough, dyspnea | Nausea, melena, abdominal pain | Anterior/posterior nasal examination |
Blood from the airway is usually bright red, frothy, and alkaline; blood from the GI tract is dark, acidic, and may contain food particles. - Fishman's Pulmonary Diseases and Disorders
Pathophysiology: Vascular Origin
Most massive hemoptysis arises from the bronchial circulation (high-pressure systemic vessels at ~100 mmHg), not the pulmonary circulation (low-pressure, ~15 mmHg). Bronchial arteries in conditions like bronchiectasis become distorted, hypertrophied, and friable. Cardiopulmonary conditions (PE, pulmonary hypertension) reduce pulmonary artery flow and cause compensatory bronchial artery hypertrophy at anastomotic sites, further increasing bleeding risk. Dieulafoy's disease of the bronchus - a submucosal fistula between bronchial and pulmonary arteries - is a rare but recognized cause. - Fishman's; Tintinalli's Emergency Medicine
Etiology
Airway Causes
- Acute/chronic bronchitis - most common cause overall in developed countries (blood-streaked sputum)
- Bronchiectasis - major source of massive hemoptysis; distorted, hypertrophied bronchial vessels
- Bronchogenic carcinoma - accounts for a large proportion of cases; up to 20% of lung cancer patients have hemoptysis at some point
- Endobronchial metastases - from carcinoid tumors, breast, colon, renal, melanoma
- Carcinoid tumor - biopsy can cause impressive hemorrhage
- Foreign body
Parenchymal/Infectious Causes
- Tuberculosis - leading cause worldwide; destruction of lung parenchyma ruptures blood vessels; cavitary TB can erode into pulmonary artery forming a Rasmussen aneurysm with potentially fatal hemorrhage
- Pneumonia - bacterial, viral
- Lung abscess
- Aspergillosis/fungal infections - especially in immunocompromised patients; cavitary lesions after granulocytopenia resolves
- Bronchiectasis (post-TB, cystic fibrosis)
- Parasitic: Paragonimus (lung fluke from infected crustaceans), Echinococcus (hydatid cysts)
Vascular Causes
- Pulmonary embolism with infarction (usually not massive)
- Mitral stenosis - pulmonary venous hypertension
- Arteriovenous malformations (Osler-Weber-Rendu / HHT - friable telangiectasias)
- Pulmonary artery pseudoaneurysm (Rasmussen aneurysm in TB cavities)
Inflammatory/Autoimmune
- Granulomatosis with polyangiitis (formerly Wegener's) - associated with saddle nose deformity, hematuria
- Goodpasture syndrome - anti-GBM antibody disease; ask about hematuria/renal insufficiency
- Diffuse alveolar hemorrhage - from vasculitis, bone marrow transplantation chemotherapy
Other Causes
- Iatrogenic - Swan-Ganz catheter injury, bronchoscopic biopsy, lung biopsy
- Trauma - deceleration injuries, penetrating thoracic trauma
- Tracheoinnominate fistula - erosion of tracheostomy into the innominate artery (catastrophic)
- Aortobronchial fistula - aortic aneurysm erosion into airway
- Catamenial - cyclical hemoptysis with menstruation (pulmonary endometriosis)
- Drug/toxic - cocaine/heroin inhalation, nitrogen dioxide exposure (diffuse alveolar hemorrhage); bevacizumab/ramucirumab (VEGF inhibitors) increase risk especially in squamous cell NSCLC with cavitary lesions
- Cryptogenic - ~30% historically; CT has reduced this proportion
Age/smoking rule of thumb: Hemoptysis before middle age: think infections. After age 40-45 or with smoking history: bronchogenic carcinoma leads the differential. - Fishman's Pulmonary Diseases and Disorders
Classification by Severity
There is no single consensus definition. The most commonly cited threshold for massive (life-threatening) hemoptysis is >200-600 mL in 24 hours. However, volume alone is insufficient - the key clinical definition is any hemoptysis that threatens life, regardless of volume, especially in patients with underlying lung disease, low reserve, or rapid bleeding rate. - Harrison's Principles of Internal Medicine 22E (2025)
| Grade | Characteristics | Management approach |
|---|---|---|
| Mild (non-massive) | Blood-streaked sputum, small volumes, stable | Outpatient workup, treat underlying cause |
| Massive/Life-threatening | Any hemoptysis causing respiratory/hemodynamic instability | Immediate airway control, multidisciplinary emergent management |
Clinical Evaluation
History
- Smoking history, duration, pack-years
- Travel or emigration from TB-endemic regions (Africa, Southeast Asia, Eastern Europe, Middle East, inner-city areas)
- History of structural lung disease (bronchiectasis, COPD, cystic fibrosis)
- Fever, weight loss, night sweats (TB, malignancy)
- Hematuria or renal disease (Goodpasture's, GPA)
- Anticoagulant use, recent procedures
- Cyclical timing with menstruation (catamenial/endometriosis)
- Drug use (cocaine, heroin inhalation)
Physical Examination
- Examine sputum directly (blood-streaked vs. frank blood/clots)
- Oral cavity and nasopharynx (exclude epistaxis, gingival bleeding)
- Lung auscultation: rales, bronchial breath sounds, amphoric sounds over cavities
- Clubbing (chronic suppurative disease, malignancy)
- Saddle nose deformity (GPA)
- Telangiectasias on lips/tongue (HHT/Osler-Weber-Rendu)
- Signs of DVT/PE
Investigations
Initial Workup
- Chest X-ray - insensitive for lateralizing/identifying source, especially in mild hemoptysis; useful as a starting point
- CBC (anemia from chronic blood loss, thrombocytopenia)
- Coagulation studies (PT, INR, aPTT)
- Renal function + urinalysis (GPA, Goodpasture's)
- Sputum AFB (TB smear/culture)
CT Chest
CT is the imaging investigation of choice. It identifies the cause and localizes the source of bleeding in 70-88% of cases, far outperforming plain radiographs. Specific findings:
- CT chest with IV contrast / CT angiography - visualizes bronchial/nonbronchial systemic arteries and the pulmonary circulation
- Identifies bronchial artery hypertrophy (diameter ≥2-3 mm), tortuous vessels, aneurysm formation, pleural thickening adjacent to parenchymal disease
- Preferred over plain CT in massive hemoptysis for procedural planning
- Indications for CT: suspected malignancy, bronchiectasis/cavitary disease, candidates for embolization
Multidetector CT (MDCT) using 16-detector rows or greater in a single breath hold is preferred for massive hemoptysis evaluation. It can detect Rasmussen aneurysms, Dieulafoy disease, and anomalous vessels. - Murray & Nadel's; Tintinalli's
Bronchoscopy
- Role is controversial in non-massive hemoptysis - does not increase diagnostic yield beyond CT
- In massive hemoptysis: early bronchoscopy (during active bleeding or within 48 hours) can localize the bleeding source and guide embolization
- Current recommendation: MDCT before bronchoscopy in most cases of massive hemoptysis
- Allows direct therapeutic interventions: clot clearance, Nd:YAG laser, argon plasma coagulation (APC), electrocautery, topical hemostatic tamponade
Management
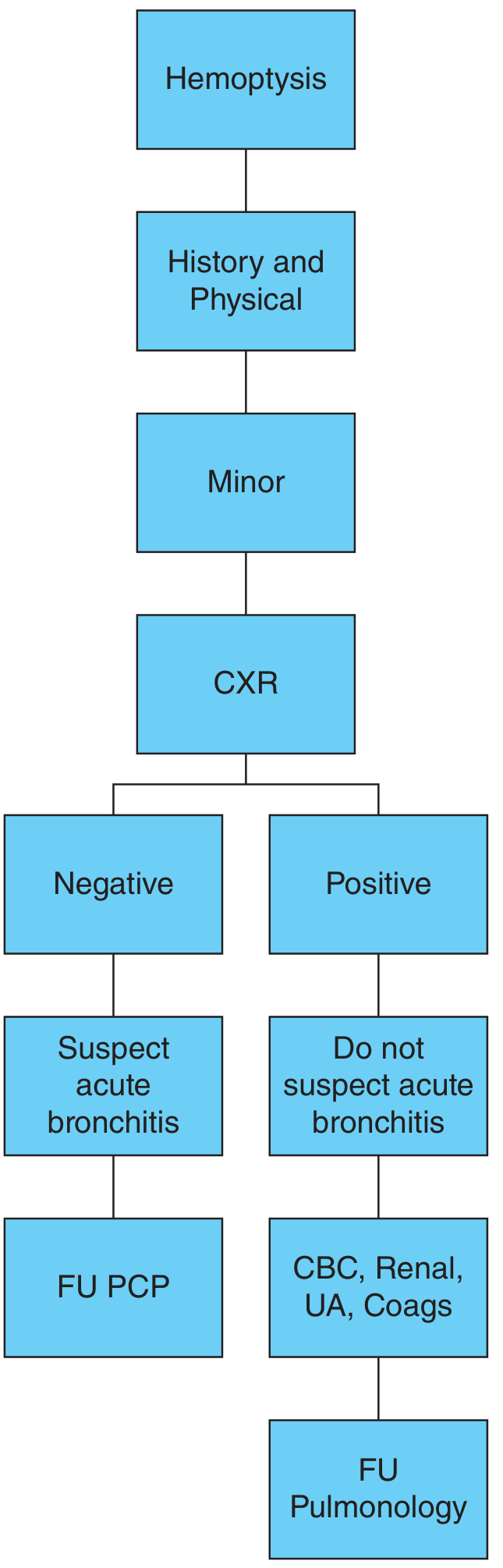
Mild Hemoptysis
- Identify and treat the underlying cause
- Acute bronchitis: antibiotics if bacterial
- Arrange follow-up with pulmonologist if structural disease or malignancy suspected
- Most cases are self-limited with conservative management
Massive Hemoptysis - Emergency Management
Priorities: Airway → Oxygenation → Hemodynamic stabilization
Step 1: Airway Control
- Position the patient - lateral decubitus with bleeding side DOWN to prevent aspiration into the unaffected lung
- If intubation required: use large-bore ETT (to allow bronchoscopy)
- If the bleeding side is known and uncontrollable: selective right (or left) main bronchus intubation of the unaffected lung to protect it
- Fogarty catheter (14F/100 cm) can be used to tamponade the affected bronchus
- Tracheoinnominate fistula (from tracheostomy erosion): immediate digital pressure on the anterior trachea through the tracheostomy site against the posterior sternum - emergency surgical consultation
Step 2: Investigations
- MDCT chest angiography (after stabilization) to localize and plan intervention
- Multidisciplinary consultation: pulmonology + interventional radiology + cardiothoracic surgery + ICU
Step 3: Definitive Bleeding Control
| Modality | Details |
|---|---|
| Bronchial artery embolization (BAE) | First-line definitive treatment for massive and recurrent hemoptysis. Controls bleeding in 75-90% of cases. Allows safer definitive surgery if needed. |
| Rebleeding after BAE | Occurs in 20-50% without definitive surgery; usually responds to second embolization |
| BAE complications | Postembolization syndrome (pleuritic pain, fever, dysphagia, leukocytosis - resolves in 5-7 days); rare: transverse myelitis (spinal cord ischemia), pulmonary infarction, bronchial/esophageal necrosis, MI |
| Endoscopic (bronchoscopic) therapy | Nd:YAG laser, APC, electrocautery for directly visualized lesions; topical hemostatic agents |
| Surgery | Reserved for: failed embolization, iatrogenic pulmonary artery injury, thoracic trauma, tracheoinnominate fistula. Better outcomes in non-urgent setting. |
- Harrison's 22E (2025): BAE is considered the first-line definitive procedure; controls brisk bleeding in 75-90%, allowing safer definitive surgery if appropriate.
- Tintinalli's: BAE followed by bronchoscopy if necessary is the initial and most effective treatment of massive and recurrent hemoptysis.
Special Situations
- Aspergillosis-related cavitary lesions in hematologic malignancy: Cavitation after granulocytopenia resolves can cause massive hemoptysis; correct thrombocytopenia/coagulopathy; surgical evaluation recommended
- Bevacizumab/ramucirumab (VEGF inhibitors): Contraindicated in NSCLC patients with squamous histology, cavitary lesions, or prior hemoptysis ≥2.5 mL in the past 3 months due to high risk of pulmonary hemorrhage
- Pulmonary embolism with infarction: Hemoptysis generally does not pose increased major bleeding risk, but underlying conditions like bronchiectasis or lung cancer may significantly increase risk; vena cava filter may be warranted if anticoagulation risk is high
Disposition
- Mild, self-limited hemoptysis with normal CXR and no risk factors: outpatient PCP or pulmonologist follow-up
- Any severe hemoptysis, hemodynamic/respiratory instability, or high-risk etiology: ICU admission or transfer to tertiary care center
Key Clinical Pearls
- ~30% of hemoptysis cases were historically cryptogenic; MDCT has substantially reduced this.
- Bronchial (not pulmonary) artery is the source of most life-threatening hemoptysis due to high systemic perfusion pressure.
- TB is the leading cause worldwide; bronchogenic carcinoma leads after age 40-45 with smoking history.
- Rasmussen aneurysm = pulmonary artery pseudoaneurysm from erosion of TB cavity wall - potentially fatal.
- Tracheoinnominate fistula from tracheostomy = catastrophic; first-line control is digital pressure.
- BAE controls 75-90% of massive hemoptysis but carries 20-50% rebleeding risk without definitive surgical correction of the underlying cause.
- A recent 2025 systematic review on nebulized tranexamic acid for hemoptysis (PMID 39841268) supports its emerging role in hemoptysis management.
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Fishman's Pulmonary Diseases and Disorders | Murray & Nadel's Textbook of Respiratory Medicine | Tintinalli's Emergency Medicine | Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.