What is arterial pulse
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the arterial pulse, drawn from Ganong's Review of Medical Physiology and Fuster & Hurst's The Heart.
Arterial Pulse
Definition & Origin
The arterial pulse is a pressure wave generated when blood is ejected from the left ventricle into the aorta during systole. This ejection does two things simultaneously:
- Moves blood forward through the vasculature
- Creates a traveling pressure wave that expands arterial walls as it propagates distally
The expansion of the arterial wall as the wave passes is what you feel as the "pulse." — Ganong's Review of Medical Physiology
Pulse Wave Velocity
The speed at which the wave travels is independent of, and much faster than, actual blood flow velocity:
| Vessel | Pulse Wave Velocity |
|---|---|
| Aorta | ~4 m/s |
| Large arteries | ~8 m/s |
| Small arteries | ~16 m/s |
As a result, the radial pulse is felt at the wrist about 0.1 seconds after peak systolic ejection. With aging, arteries stiffen and the wave travels even faster.
Pulse Strength
- Determined primarily by pulse pressure (systolic − diastolic), not mean pressure
- Proportional to stroke volume
- Weak/thready pulse: shock, low stroke volume
- Strong/bounding pulse: high stroke volume (exercise, histamine, aortic regurgitation)
- In aortic regurgitation, the pulse is so forceful it may cause visible head nodding — the classic Corrigan (water-hammer) pulse
The Dicrotic Notch
A small oscillation on the descending limb of the pressure wave caused by vibrations when the aortic valve snaps shut. It is visible on pressure recordings but not palpable at the wrist.
Examination Technique
The pulse is best assessed at the carotid or brachial arteries. Key features to assess:
- Amplitude (indirect measure of cardiac output / stroke volume)
- Contour (rate of rise, peak timing, shape)
- Simultaneous radial + femoral palpation to detect coarctation of the aorta
— Fuster and Hurst's The Heart, 15th Edition
Abnormal Pulse Patterns
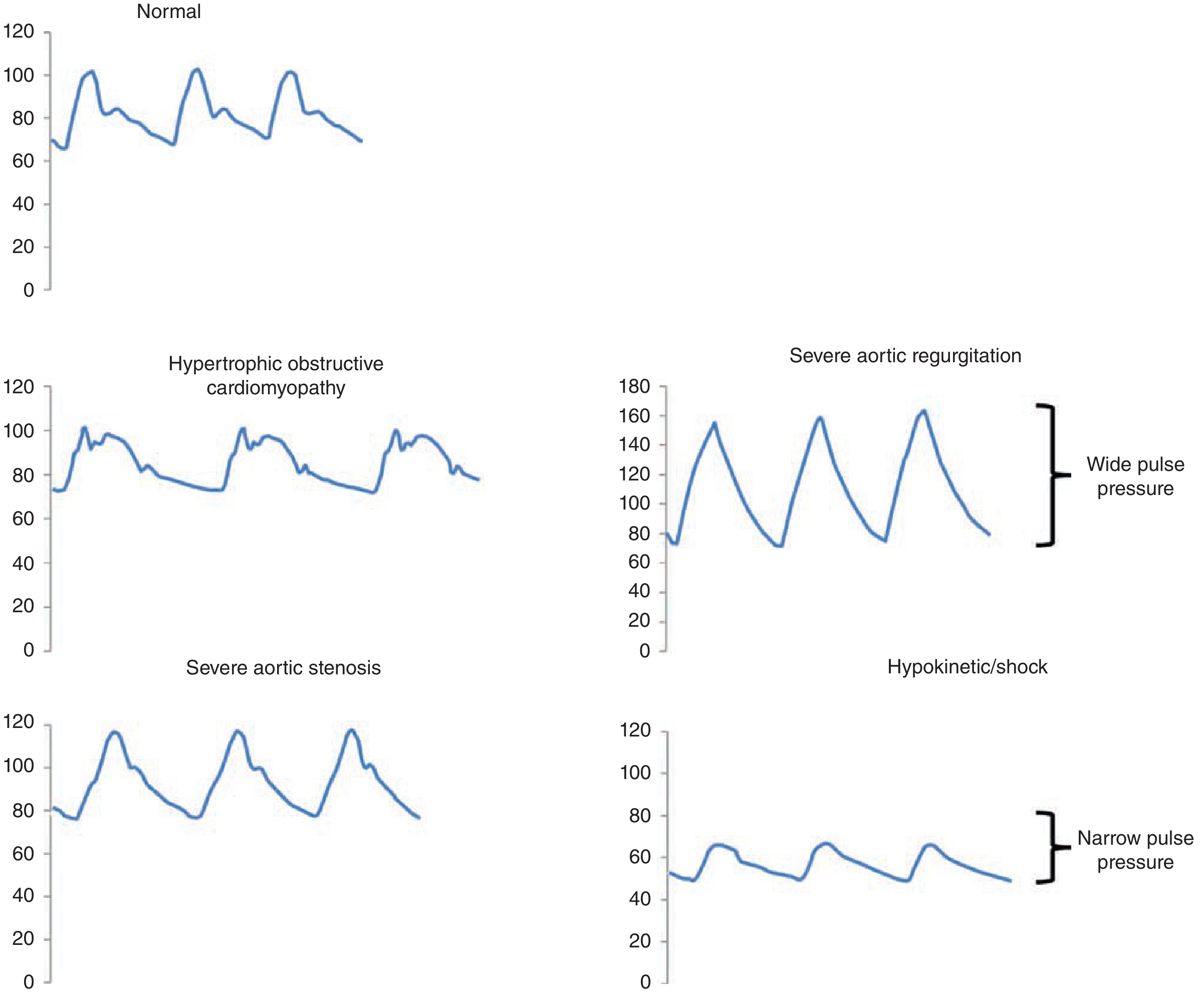
Figure: Normal arterial pulse waveform and abnormal patterns in disease states — Fuster and Hurst's The Heart, 15th Ed.
| Pulse Type | Pattern | Cause |
|---|---|---|
| Parvus et tardus | Reduced amplitude + slurred, delayed upstroke | Severe aortic stenosis |
| Spike-and-dome (bifid) | Brisk early rise, mid-systolic dip, secondary peak | Hypertrophic obstructive cardiomyopathy (HOCM) |
| Water-hammer (Corrigan) | Bounding, high amplitude, rapid collapse | Severe aortic regurgitation |
| Bisferiens | Two palpable systolic peaks | Mixed aortic valve disease (AR predominant) |
| Anacrotic | Positive notch on ascending limb | Aortic stenosis |
| Dicrotic | Exaggerated notch on descending limb | Shock / severe peripheral vasoconstriction |
| Pulsus alternans | Beat-to-beat variation in amplitude (non-respirophasic) | Severe LV systolic dysfunction (ominous sign) |
| Thready/hypokinetic | Narrow pulse pressure, weak | Shock states |
Key Clinical Points
- Pulsus alternans is non-respirophasic (distinguishes it from pulsus paradoxus, which varies with breathing)
- Amplitude of the pulse is an indirect measure of cardiac output — proportional to stroke volume
- Parvus and tardus should be graded separately (1+ to 4+); one may predominate
- In HOCM, obstruction develops mid-systole, so the initial upstroke is brisk (early forceful contraction before obstruction)
— Fuster and Hurst's The Heart, 15th Edition; Ganong's Review of Medical Physiology, 26th Edition
This is a shared conversation. Sign in to Orris to start your own chat.