In detail on thyroid from anatomy to assessment management surgery part
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
The Thyroid Gland - A Complete Clinical Reference
Sources: Gray's Anatomy for Students, Sabiston Textbook of Surgery (11th/14th ed.), Guyton & Hall Medical Physiology, Robbins & Cotran Pathologic Basis of Disease, Schwartz's Principles of Surgery
PART 1 - EMBRYOLOGY
The thyroid is the first endocrine gland to develop, arising from two distinct embryological precursor tissues called anlages.
Median Thyroid Anlage
- Begins as a thickening of the endodermal epithelium of the foregut, on the floor of the pharynx at approximately the level of what will become the base of the tongue
- This thickening evaginates and descends caudally, following the developing heart and great vessels
- The foramen cecum at the base of the tongue marks the origin site
- The path of descent is tracked by the thyroglossal duct, which normally involutes by the 7th-10th week of gestation
Lateral Thyroid Anlage
- Arises from the 4th pharyngeal pouch (ultimobranchial body)
- Provides the parafollicular C cells that secrete calcitonin
- Fuses with the median anlage to complete the gland
Clinical Significance of Embryological Remnants
| Remnant | Location | Clinical Issue |
|---|---|---|
| Lingual thyroid | Base of tongue | May be the only functional thyroid tissue |
| Thyroglossal duct cyst | Midline, moves with tongue protrusion | Most common neck mass in children |
| Pyramidal lobe | Extends superiorly from isthmus | Present in ~50% of people; must be removed in thyroidectomy |
| Thyroglossal fistula | Midline sinus | Persistent or post-infection rupture of cyst |
| Ectopic thyroid | Anywhere along descent path | May cause subclinical/clinical hypothyroidism |
Sabiston Textbook of Surgery, p. 1522 - "In utero, thyroid development begins with the median thyroid anlage, which is a thickening of the endodermal epithelium of the foregut in the floor of the pharynx... As it descends caudally, along with the developing heart and great vessels, a thin cord of tissue - the thyroglossal duct - connects the descending anlage to its site of origin."
PART 2 - GROSS ANATOMY
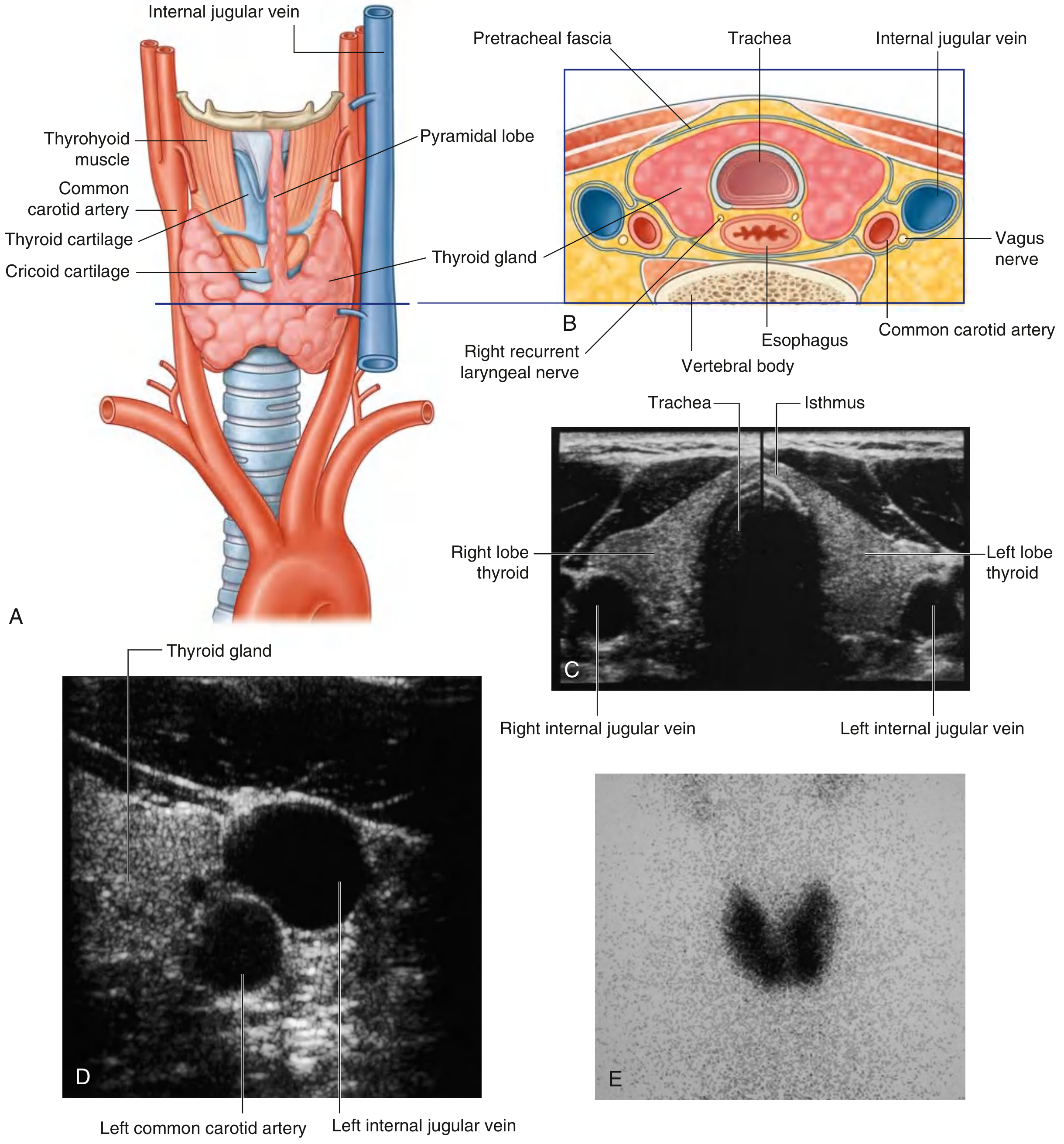
Position and Shape
- Lies anterior to the neck, inferior and lateral to the thyroid cartilage
- Consists of two lateral lobes (right and left) connected by an isthmus
- The lateral lobes cover the anterolateral surfaces of the trachea, cricoid cartilage, and lower thyroid cartilage
- Lies deep to the sternohyoid, sternothyroid, and omohyoid muscles (strap muscles) within the visceral compartment, enclosed by pretracheal fascia
- Weight: ~20-30 g in a normal adult
- Isthmus crosses the anterior surface of the 2nd and 3rd tracheal rings
- Pyramidal lobe (when present) extends superiorly from the isthmus, often toward the left
Relations
- Anterior: Strap muscles (sternohyoid over sternothyroid), investing layer of deep cervical fascia
- Posterior: Trachea and esophagus (esophagus deviates slightly left), recurrent laryngeal nerves, parathyroid glands
- Lateral: Carotid sheath (common carotid artery, internal jugular vein, vagus nerve)
- Posterior capsule: The parathyroid glands (typically 4) are embedded in or attached to the posterior thyroid capsule
PART 3 - ARTERIAL SUPPLY
Superior Thyroid Artery
- Origin: First branch of the external carotid artery
- Descends along the lateral margin of the thyrohyoid muscle to reach the superior pole of the lateral lobe
- Divides into:
- Anterior glandular branch - runs along the superior border; anastomoses with its twin across the isthmus
- Posterior glandular branch - runs to the posterior gland; may anastomose with the inferior thyroid artery
- Travels alongside the external branch of the superior laryngeal nerve (EBSLN), which is at risk during superior pole ligation in thyroidectomy
Inferior Thyroid Artery
- Origin: Thyrocervical trunk → subclavian artery
- Ascends along the medial edge of the anterior scalene muscle, passes posterior to the carotid sheath
- Divides into multiple branches before entering the inferior pole and posterior surface of the gland
- Has an important and variable relationship with the recurrent laryngeal nerve (RLN) - the nerve may pass anterior, posterior, or between branches of the inferior thyroid artery
- Supplies the parathyroid glands (this supply is at risk during thyroidectomy)
Thyroidea Ima Artery (Arteria Thyroidea Ima)
- Present in ~3-10% of individuals
- Arises from the brachiocephalic trunk or directly from the aortic arch
- Ascends on the anterior trachea to reach the isthmus
- Surgically significant during low neck incisions and tracheostomy
Venous Drainage
Three pairs of veins form a periglandular plexus:
- Superior thyroid vein - drains into the internal jugular vein (alongside superior thyroid artery)
- Middle thyroid vein - short, direct, drains into the internal jugular vein (no accompanying artery - dividing it early during thyroidectomy helps mobilize the lobe)
- Inferior thyroid vein - multiple, descend to drain into the brachiocephalic vein(s)
PART 4 - NERVE SUPPLY & SURGICAL DANGER ZONES
Recurrent Laryngeal Nerve (RLN)
- Branch of the vagus nerve
- Right RLN: Loops around the subclavian artery and ascends in the tracheoesophageal groove
- Left RLN: Loops around the arch of the aorta and ascends in the tracheoesophageal groove
- Enters the larynx posterior to the cricothyroid joint to supply all intrinsic muscles of the larynx except cricothyroid
- Relationship to inferior thyroid artery: Highly variable - may pass anterior, posterior, or between its branches
- Damage: Unilateral - hoarseness; bilateral - respiratory distress (emergency)
- Non-recurrent RLN: Rare variant (~0.5-1% right side), associated with aberrant right subclavian artery - passes directly from the vagus to the larynx horizontally; highly at risk during surgery
External Branch of Superior Laryngeal Nerve (EBSLN)
- Branch of the superior laryngeal nerve (branch of vagus)
- Descends with the superior thyroid artery on its medial side
- Supplies the cricothyroid muscle (pitch control)
- At risk during superior pole ligation; Cernea classification categorizes the relationship
- Damage: Loss of high-pitched phonation, vocal fatigue
Sympathetic Innervation
- Vasomotor supply via cervical sympathetic chains
PART 5 - LYMPHATIC DRAINAGE
- Drain along the superior thyroid veins to pre- and para-tracheal nodes, and then to the deep cervical chain
- Prelaryngeal (Delphian) node - anterior to cricothyroid membrane; if enlarged, may indicate thyroid carcinoma
- Lymphatics also drain to the superior mediastinal nodes
PART 6 - HISTOLOGY
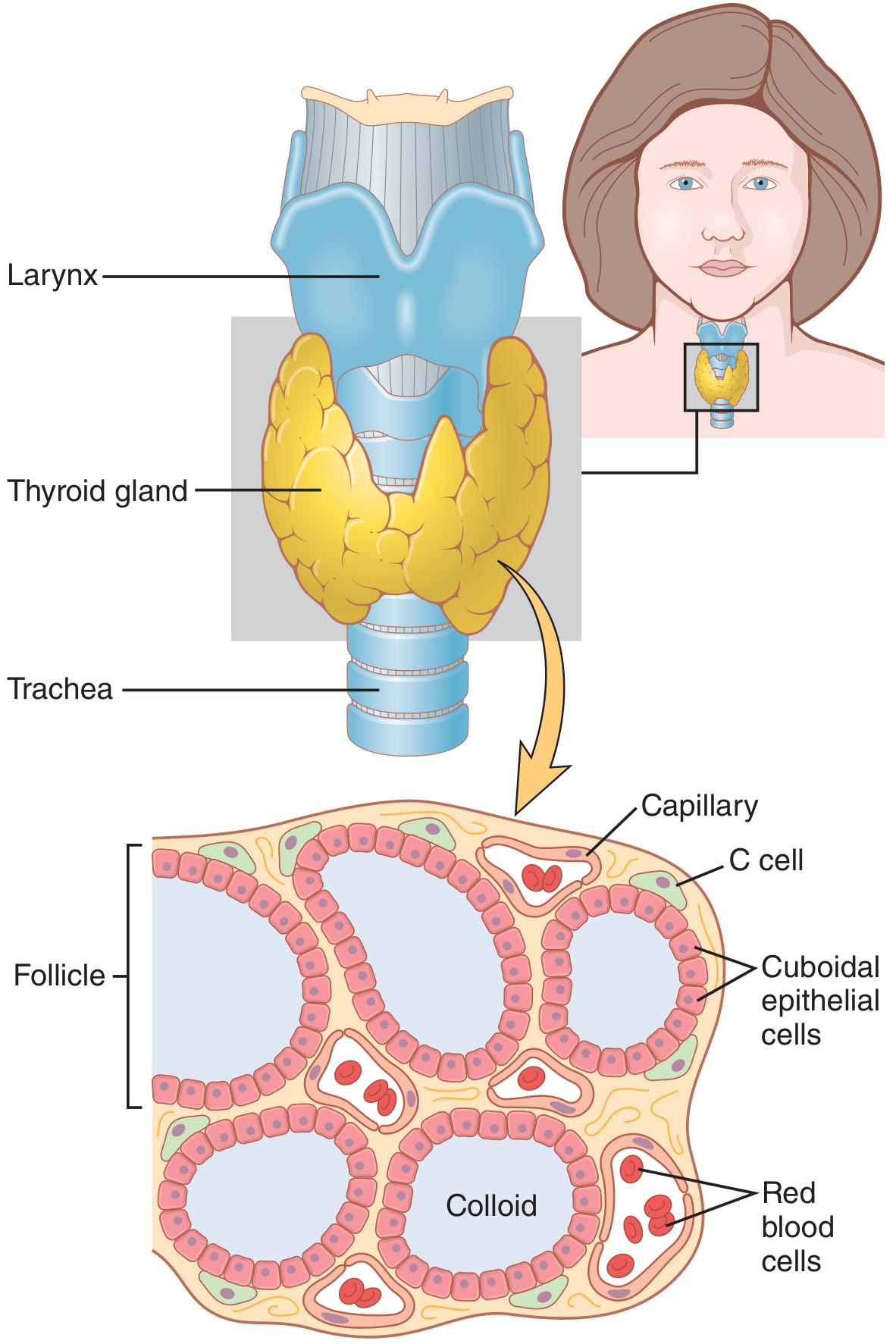
The thyroid gland is divided by thin fibrous septa into lobules, each composed of 20-40 colloid-filled follicles.
Follicular (Principal) Cells
- Cuboidal to low columnar epithelium lining the follicles
- Height varies with activity - tall columnar when active (high TSH), flat squamous when inactive
- Synthesize thyroglobulin and the thyroid hormones T4 and T3
- Have a sodium-iodide symporter (NIS) on the basolateral membrane for iodide trapping
- Apical surface faces the colloid; secretory vesicles fuse here to release thyroglobulin
Colloid
- Gel-like substance filling follicular lumen
- Consists primarily of thyroglobulin (iodinated glycoprotein - the storage form of thyroid hormone)
- Stains pink on H&E
Parafollicular C Cells
- Located between follicular cells or in interfollicular connective tissue
- Derived from the lateral anlage (ultimobranchial body / neural crest)
- Secrete calcitonin (reduces serum calcium)
- Stain lightly with H&E; immunohistochemistry with anti-calcitonin confirms them
- Are the cells of origin of medullary thyroid carcinoma
Guyton & Hall, p. 930 - "The thyroid gland is composed of large numbers of closed follicles (100-300 micrometers in diameter) that are filled with a secretory substance called colloid and lined with cuboidal epithelial cells that secrete into the interior of the follicles."
PART 7 - PHYSIOLOGY & HORMONE SYNTHESIS
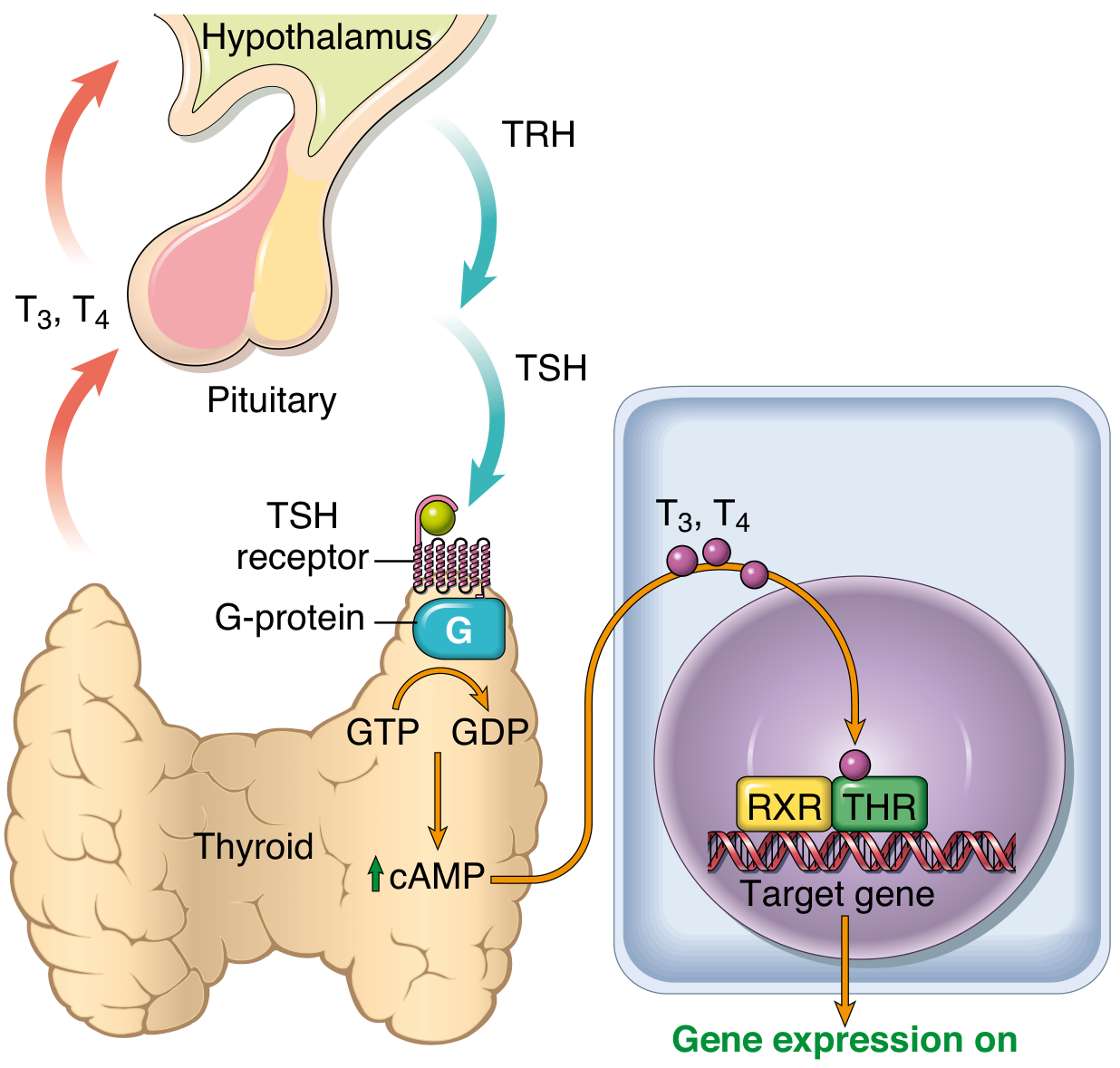
Hypothalamic-Pituitary-Thyroid (HPT) Axis
- Hypothalamus secretes TRH (thyrotropin-releasing hormone)
- Anterior pituitary thyrotrophs release TSH (thyroid-stimulating hormone / thyrotropin)
- TSH binds its receptor on follicular cells → activates Gs protein → increases cAMP → stimulates thyroid growth and hormone synthesis
- Negative feedback: T3/T4 inhibit both TRH (hypothalamus) and TSH (pituitary) secretion
Steps of Thyroid Hormone Synthesis
| Step | Process | Key Molecule |
|---|---|---|
| 1 | Iodide trapping | NIS (Na⁺/I⁻ symporter) concentrates I⁻ ~30x (up to 250x when maximally active) |
| 2 | Oxidation of iodide | Thyroid peroxidase (TPO) oxidizes I⁻ to reactive iodine |
| 3 | Organification | Reactive iodine added to tyrosine residues on thyroglobulin → MIT (monoiodotyrosine) and DIT (diiodotyrosine) |
| 4 | Coupling | TPO couples MIT + DIT → T3 (3,5,3'-triiodothyronine); DIT + DIT → T4 (thyroxine) |
| 5 | Storage | Iodinated thyroglobulin stored as colloid (~100 days' supply) |
| 6 | Secretion | TSH stimulates endocytosis of colloid; lysosomal proteases cleave thyroglobulin; T3/T4 released into blood |
| 7 | Peripheral conversion | ~80% of circulating T3 comes from deiodination of T4 in peripheral tissues (liver, kidney, muscle) |
Thyroid Hormones in Blood
- T4: Half-life ~6 days; mostly protein-bound (TBG > transthyretin > albumin)
- T3: Half-life ~1 day; biologically more active; binds nuclear receptors with 10x greater affinity than T4
- T3 is the active nuclear hormone - T4 acts as a prohormone
Physiological Effects of Thyroid Hormones
- Metabolic: Increase BMR; stimulate carbohydrate, fat, and protein metabolism; increase O2 consumption in all tissues except brain, testes, spleen
- Cardiovascular: Increase heart rate and cardiac output; enhance adrenergic receptor sensitivity
- Growth & Development: Essential for bone growth (GH synergy) and brain development in fetus and neonates (hypothyroidism → cretinism)
- Thermoregulation: Increase thermogenesis (calorigenic effect)
- Hematopoietic: Stimulate erythropoiesis
- Lipid metabolism: Reduce LDL and total cholesterol (hence hypothyroidism causes hypercholesterolemia)
Iodine Requirements
- ~50 mg/year (1 mg/week) of iodine needed for normal hormone production
- Iodine deficiency → goiter (TSH-driven hyperplasia) and hypothyroidism
- Table salt iodization (1:100,000) is the primary prevention strategy
PART 8 - CLINICAL ASSESSMENT
History
Symptoms of Hypothyroidism:
- Fatigue, weight gain, cold intolerance, constipation
- Bradycardia, dry skin, hair loss, menorrhagia
- Cognitive slowing, depression, myxedema (severe)
- In neonates: jaundice, poor feeding, macroglossia, constipation
Symptoms of Hyperthyroidism:
- Weight loss despite increased appetite, heat intolerance, sweating
- Palpitations, tremor, anxiety, irritability, insomnia
- Diarrhea, oligomenorrhea
- Exophthalmos (Graves disease specifically)
General Thyroid History:
- Duration and progression of symptoms
- Family history of thyroid disease or autoimmune conditions
- Prior neck radiation (risk factor for thyroid cancer)
- Medications (amiodarone, lithium, iodine-containing contrast)
- Pregnancy/postpartum status
- Compressive symptoms: dysphagia, stridor, hoarseness, neck pressure
Physical Examination
Inspection:
- Midline neck swelling; moves with swallowing (thyroid) vs. sticking out tongue (thyroglossal cyst)
- Symmetry of enlargement
Palpation (from behind):
- Size, shape, consistency (soft/firm/hard/nodular)
- Tenderness (subacute thyroiditis)
- Lymphadenopathy
- Pyramidal lobe
Auscultation:
- Bruit over the gland = hypervascular (Graves disease classically)
Systemic Signs:
| System | Hypothyroidism | Hyperthyroidism |
|---|---|---|
| Pulse | Bradycardia | Tachycardia, AF |
| Skin | Dry, coarse, myxedematous | Warm, moist, fine |
| Hair | Coarse, thinning, loss of lateral 1/3 eyebrow | Fine, diffuse loss |
| Reflexes | Delayed relaxation | Hyperreflexia |
| Eyes | Periorbital puffiness | Exophthalmos (Graves) |
| BP | Diastolic hypertension | Wide pulse pressure |
PART 9 - INVESTIGATIONS
Biochemical Tests
| Test | Reference Range | Interpretation |
|---|---|---|
| TSH | 0.4-4.0 mU/L | Best initial test; most sensitive; low in hyperthyroidism, high in hypothyroidism |
| Free T4 | 9-23 pmol/L | Confirms thyroid function; ordered after abnormal TSH |
| Free T3 | 3.5-7.8 pmol/L | Useful in T3 thyrotoxicosis, monitoring |
| Anti-TPO antibodies | <35 IU/mL | Elevated in Hashimoto's and Graves disease |
| Anti-thyroglobulin antibodies | Elevated in Hashimoto's | |
| TSH receptor antibodies (TRAb) | Graves disease confirmation | |
| Thyroglobulin (Tg) | Tumor marker for differentiated thyroid cancer (post-thyroidectomy) | |
| Calcitonin | Tumor marker for medullary thyroid carcinoma | |
| CEA | Elevated in medullary thyroid carcinoma |
Thyroid Function Pattern Interpretation
| TSH | Free T4 | Diagnosis |
|---|---|---|
| Low | High | Primary hyperthyroidism / thyrotoxicosis |
| High | Low | Primary hypothyroidism |
| Low | Low/Normal | Secondary (pituitary) hypothyroidism |
| Normal | Normal | Euthyroid |
| Low | Normal | Subclinical hyperthyroidism |
| High | Normal | Subclinical hypothyroidism |
Imaging
Ultrasound (US) - First-line imaging:
- Defines size, lobes, nodule characteristics
- Suspicious features (TIRADS): solid, hypoechoic, irregular margins, microcalcifications, taller-than-wide shape, extrathyroidal extension
- Guides FNA biopsy
- Evaluates lymph nodes
Nuclear Scintigraphy (Tc-99m or I-123):
- Assesses functional status of nodules
- "Hot" (autonomous) nodule = increased uptake; rarely malignant
- "Cold" (non-functioning) nodule = decreased uptake; higher risk of malignancy (~10-15%)
- Diffuse uptake = Graves disease; heterogeneous = toxic multinodular goiter
- Pre-RAI treatment planning
CT/MRI:
- Substernal goiter - extent of mediastinal involvement
- Thyroid cancer staging - invasion of surrounding structures
- Recurrent disease mapping
- Note: Iodinated CT contrast delays RAI by weeks - use MRI when possible
PET-CT:
- Radioiodine-negative DTC (differentiated thyroid cancer)
- Aggressive histologies / recurrent disease
Fine-Needle Aspiration (FNA) Cytology
- Gold standard for evaluating thyroid nodules
- Bethesda System for Reporting Thyroid Cytopathology:
| Bethesda Category | Description | Malignancy Risk | Action |
|---|---|---|---|
| I | Non-diagnostic/unsatisfactory | N/A | Repeat FNA |
| II | Benign | <3% | Clinical follow-up |
| III | Atypia of undetermined significance (AUS/FLUS) | 10-30% | Repeat FNA or molecular testing |
| IV | Follicular neoplasm/suspicious for FN | 25-40% | Surgical lobectomy |
| V | Suspicious for malignancy | 50-75% | Near-total/total thyroidectomy |
| VI | Malignant | 97-99% | Definitive surgery |
Molecular Testing:
- Used on indeterminate FNA (Bethesda III/IV)
- Tests: ThyroSeq, Afirma Gene Expression Classifier
- Panels test for BRAF, RAS, RET/PTC, PAX8/PPAR-gamma mutations to guide surgical vs. surveillance decisions
PART 10 - THYROID DISORDERS & MANAGEMENT
A. Hypothyroidism
1. Hashimoto's Thyroiditis (Chronic Lymphocytic Thyroiditis)
- Most common cause of hypothyroidism in iodine-sufficient regions
- Autoimmune: CD8+ cytotoxic T cells and anti-TPO/anti-Tg antibodies destroy follicular cells
- Pathology: Dense lymphocytic infiltrate with germinal centers; Hurthle cell (oxyphilic) metaplasia of follicular cells; fibrosis
- Clinical: Painless symmetric goiter + gradual hypothyroidism; "Hashitoxicosis" may precede (release of preformed hormone)
- Increased risk of: other autoimmune diseases, thyroid lymphoma, possibly papillary thyroid carcinoma
- Management: Levothyroxine (T4) replacement; titrate to normalize TSH; lifelong therapy
2. Subacute (Granulomatous/de Quervain's) Thyroiditis
- Viral (post-viral) etiology; associated with coxsackie, mumps
- Painful thyroid, tender to palpation, low-grade fever, elevated ESR
- Triphasic: hyperthyroid → euthyroid → hypothyroid → recovery
- Pathology: Granulomatous inflammation with giant cells
- Management: NSAIDs for pain; beta-blockers for transient thyrotoxicosis; steroids if severe; levothyroxine if prolonged hypothyroid phase
3. Riedel Thyroiditis
- Rare, fibro-inflammatory; "woody hard" thyroid; may compress trachea/esophagus
- IgG4-related disease
- Management: Surgery if causing compression; steroids; tamoxifen
4. Iatrogenic Hypothyroidism
- Post-thyroidectomy, post-radioiodine ablation, drugs (amiodarone, lithium, anti-thyroid drugs)
- Management: Levothyroxine replacement
Levothyroxine Dosing:
- Starting dose: 1.6 mcg/kg/day (lower in elderly and cardiac patients)
- Monitor TSH at 6-8 weeks after dose changes
- Target TSH: 0.5-2.5 mU/L (post-cancer: TSH suppression to <0.1 mU/L)
B. Hyperthyroidism
1. Graves Disease
- Most common cause of hyperthyroidism (~80%)
- Autoimmune: TSH receptor-stimulating antibodies (TRAb/TSI) bind and stimulate TSH receptors
- Clinical triad: Diffuse goiter + ophthalmopathy (Graves orbitopathy) + pretibial myxedema
- Ophthalmopathy: Exophthalmos, lid retraction, periorbital edema, opthalmoplegia; due to TSH receptor antibodies cross-reacting with orbital fibroblasts
- Management Options:
- Anti-thyroid drugs (ATDs): Methimazole (1st line) or propylthiouracil (PTU, used in 1st trimester pregnancy, thyroid storm); inhibit TPO; monitor for agranulocytosis
- Radioactive iodine (RAI) I-131: Ablates thyroid; results in hypothyroidism requiring lifelong T4; contraindicated in pregnancy and severe ophthalmopathy
- Surgery (total thyroidectomy): When ATDs/RAI fail, patient preference, large goiter, coexisting malignancy, pregnancy contraindications to RAI
2. Toxic Multinodular Goiter (Plummer's Disease)
- Multiple autonomously functioning nodules; more common in elderly and iodine-deficient areas
- TSH suppressed; T3/T4 elevated; scintigraphy: heterogeneous or patchy uptake
- Management: RAI or surgery (subtotal/total thyroidectomy) preferred in large goiters or compressive symptoms
3. Toxic Adenoma (Solitary Autonomous Nodule)
- Single hot nodule on scintigraphy (suppresses surrounding normal tissue)
- Often due to activating TSH receptor mutation (TSHR)
- Management: RAI or surgical excision (lobectomy)
4. Thyroid Storm (Thyrotoxic Crisis)
- Life-threatening emergency; precipitated by surgery, infection, trauma in uncontrolled hyperthyroid
- Burch-Wartofsky score for diagnosis
- Management: PTU (blocks synthesis + peripheral conversion of T4→T3), SSKI (iodine), propranolol, hydrocortisone, supportive care
5. Amiodarone-Induced Thyrotoxicosis
- Type 1 (excess iodine in pre-existing goiter): ATDs
- Type 2 (destructive thyroiditis): Steroids
C. Goiter
Endemic/Diffuse Goiter:
- Iodine deficiency → decreased T3/T4 → increased TSH → diffuse thyroid hyperplasia
- Management: Iodine supplementation, levothyroxine to suppress TSH
Nontoxic Multinodular Goiter:
- Long-standing iodine deficiency → cyclical hyperplasia → nodule formation
- Substernal extension may cause compressive symptoms (stridor, dysphagia, SVC obstruction)
- Workup: USS, TFTs, CT for substernal extension
- Management: Observation if small/asymptomatic; surgery if compressive, suspicious for malignancy, or patient preference
D. Thyroid Cancer
Four main types:
| Type | Origin | Frequency | Features |
|---|---|---|---|
| Papillary (PTC) | Follicular cell | ~80% | Best prognosis; "Orphan Annie eye" nuclei; psammoma bodies; RET/PTC, BRAF mutations |
| Follicular (FTC) | Follicular cell | ~10% | Vascular and capsular invasion; RAS, PAX8/PPAR-gamma mutations; hematogenous spread (bone, lung) |
| Medullary (MTC) | C cells | ~5% | Sporadic or familial (MEN 2A/2B); RET mutation; calcitonin as tumor marker; amyloid deposits |
| Anaplastic (ATC) | Follicular cell | ~1-2% | Rapidly fatal; most aggressive; TP53 mutations; often from dedifferentiated DTC |
Differentiated Thyroid Cancer (DTC) - Management:
- Papillary microcarcinoma (<1 cm): Active surveillance or lobectomy
- Low-risk PTC/FTC: Thyroid lobectomy
- High-risk DTC (>4 cm, extrathyroidal extension, nodal disease): Total thyroidectomy + central neck dissection
- Radioactive iodine (RAI) ablation: Post-thyroidectomy for high-risk disease to ablate remnant and treat metastases
- TSH suppression: Levothyroxine therapy to keep TSH <0.1 mU/L reduces recurrence risk
- Follow-up: Thyroglobulin levels + neck US at intervals; rising Tg signals recurrence
Medullary Thyroid Cancer:
- Total thyroidectomy + central neck dissection is the only curative treatment
- Genetic testing for RET mutation in all patients + family screening
- Prophylactic thyroidectomy in RET mutation carriers (timing based on specific mutation - ATA risk classification A-D)
- Systemic therapy: Vandetanib or cabozantinib for advanced/metastatic disease
PART 11 - THYROID SURGERY
Indications for Thyroidectomy
- Hyperthyroidism (failed/contraindicated medical therapy)
- Goiters with compressive symptoms
- Thyroid nodules (indeterminate or malignant)
- Thyroid cancer
Types of Resection
| Procedure | Description | Indication |
|---|---|---|
| Total thyroidectomy | All visible thyroid removed; <1g remnant | Cancer, Graves, large goiter |
| Near-total thyroidectomy | <1 g remnant left at ligament of Berry | Graves disease (protects RLN) |
| Subtotal thyroidectomy | 3-5 g remnant left | Less common today |
| Hemithyroidectomy (Lobectomy) | One lobe + isthmus ± pyramidal lobe | Low-risk DTC, solitary nodule |
| Isthmusectomy | Isthmus only | Rarely (papillary microcarcinoma of isthmus) |
Sabiston Textbook of Surgery, p. 1522 - "In modern practice, the vast majority of thyroid resections fall under two categories: total thyroidectomy, in which all or nearly all of the visible thyroid gland is excised, and thyroid lobectomy, in which all of the visible thyroid on one side is excised along with the isthmus."
Preoperative Preparation
- Biochemical: TFTs, calcium (parathyroid baseline), CBC
- Imaging: Neck ultrasound; CT/MRI for substernal goiter
- FNA: If not already performed for nodular disease
- Voice assessment: Laryngoscopy to document pre-existing RLN function
- Euthyroid state: For hyperthyroid patients, achieve euthyroid with ATDs before surgery
- Graves disease pre-op: Potassium iodide (Lugol's iodine) 10-14 days before surgery to reduce gland vascularity
Surgical Technique - Total Thyroidectomy
1. Positioning & Incision:
- Supine with neck extended (shoulder roll)
- Kocher incision: transverse collar incision, 1-2 cm above sternal notch, in a skin crease
2. Flap development:
- Superior flap to thyroid cartilage; inferior flap to sternal notch
- Platysma divided; subplatysmal flaps raised
3. Midline division:
- Median raphé of strap muscles divided longitudinally
- Sternohyoid and sternothyroid separated from thyroid
4. Lateral mobilization:
- Middle thyroid vein divided early - critical step to mobilize the lobe
- Medial rotation of the lobe exposes the posterior surface
5. Superior pole dissection:
- Superior pole vessels ligated individually (not en masse) close to the gland to protect the EBSLN
- "Skeletonizing" the superior pole to avoid EBSLN injury
6. Recurrent laryngeal nerve (RLN) identification:
- Mandatory before ligation of inferior thyroid artery branches
- Located in the tracheoesophageal groove
- Landmarks: Inferior thyroid artery, Berry's ligament (suspensory ligament of thyroid - dense fibrous band attaching thyroid to trachea; the nerve runs immediately posterior), Zuckerkandl's tubercle (posterior thyroid protrusion - RLN runs medial to it)
- Nerve followed to entry point at cricothyroid joint
- Intraoperative nerve monitoring (IONM) increasingly used
7. Parathyroid identification and preservation:
- Superior parathyroids: Usually at the level of inferior thyroid artery, posterior to the RLN, near the posterior thyroid capsule
- Inferior parathyroids: More variable position; commonly anterior to the RLN at the inferior thyroid pole
- Preserve with intact blood supply (inferior thyroid artery branches)
- Autotransplantation: If blood supply is compromised, parathyroid is minced and implanted into the sternocleidomastoid muscle
8. Berry's ligament division:
- Final attachment of thyroid to trachea
- RLN is at greatest risk here - must be under direct vision
9. Hemostasis and closure:
- Meticulous hemostasis
- Drain placement (surgeon preference)
- Layer closure: strap muscles, platysma, subcuticular skin
Adjunctive Technologies
- Intraoperative nerve monitoring (IONM): EMG endotracheal tube monitors RLN function; helps identify nerve, confirms neural integrity; does not eliminate RLN injury but reduces risk
- Harmonic scalpel / LigaSure: Energy devices for hemostasis reduce operative time
- Fluorescence: Near-infrared autofluorescence (NIRAF) to identify parathyroid glands intraoperatively; reduces inadvertent parathyroidectomy
Complications
| Complication | Incidence | Presentation | Management |
|---|---|---|---|
| RLN injury (unilateral) | 0.5-2% permanent | Hoarseness, aspiration | Voice therapy; medialization injection/thyroplasty if permanent |
| RLN injury (bilateral) | <0.5% | Stridor, respiratory distress | Emergency airway management; tracheostomy |
| Hypoparathyroidism (transient) | Up to 30% | Perioral tingling, Chvostek's/Trousseau's sign, tetany | IV/oral calcium ± calcitriol |
| Hypoparathyroidism (permanent) | 1-3% | Chronic hypocalcemia | Long-term calcium + calcitriol |
| Neck hematoma | 0.3-1% | Expanding neck swelling, stridor | Return to OR immediately; bedside hematoma evacuation if airway compromised |
| Wound infection | <1% | Antibiotics | |
| Thyroid storm | Rare | Uncontrolled hyperthyroid | PTU, beta-blockers, iodide, steroids |
| Seroma | Variable | Fluid collection | Aspiration |
| EBSLN injury | 1-10% | Vocal fatigue, loss of high notes | Usually improves; voice therapy |
Postoperative Care
- Calcium monitoring: Serum calcium and PTH at 6 hours post-op; PTH <10 pg/mL predicts hypoparathyroidism
- Voice check: Before discharge
- Levothyroxine: Started next morning post-op (TSH-suppressive dosing for cancer, replacement for goiter/Graves)
- Drain: Removed when output <30 mL/24 hours
Minimally Invasive and Alternative Approaches
- Endoscopic thyroidectomy: Minimally invasive video-assisted thyroidectomy (MIVAT) for small thyroid and nodules <3 cm
- Robotic thyroidectomy: Remote-access approaches (transaxillary, transoral, retroauricular/facelift) to avoid neck scar; cosmetically superior but longer operative time and learning curve
- Transoral endoscopic thyroidectomy (TOETVA): No external incision; scar-free; gaining adoption in Asia and globally
- Thermal ablation (non-surgical): Radiofrequency ablation (RFA) or laser ablation for benign nodules/low-risk papillary microcarcinoma in selected patients
Summary Reference Card
| Domain | Key Points |
|---|---|
| Embryology | Median anlage (pharynx) + lateral anlage (4th pouch/C cells); thyroglossal duct; foramen cecum |
| Anatomy | 2 lobes + isthmus; strap muscles anterior; RLN in TE groove; 4 parathyroids on posterior capsule |
| Blood supply | Superior (ECA) and inferior (thyrocervical trunk); venous drainage via IJV and brachiocephalic |
| Key nerves | RLN (all intrinsic laryngeal except cricothyroid); EBSLN (cricothyroid); both at risk in thyroidectomy |
| Histology | Follicular cells (T3/T4); C cells (calcitonin); colloid (thyroglobulin storage) |
| Synthesis | Iodide trapping (NIS) → oxidation (TPO) → organification → coupling → secretion → T4 deiodinates to active T3 |
| Investigation | TSH best initial test; USS + FNA for nodules; Bethesda classification; scintigraphy for functional assessment |
| Hypothyroid Rx | Levothyroxine 1.6 mcg/kg/day; titrate TSH to 0.5-2.5 mU/L |
| Hyperthyroid Rx | ATDs (methimazole/PTU) → RAI or surgery |
| Cancer | PTC most common; total thyroidectomy ± RAI; calcitonin/RET for MTC; Tg for surveillance |
| Surgery | RLN identification mandatory; preserve parathyroids; IONM reduces nerve risk; hematoma = emergency |
Sources: Gray's Anatomy for Students (9th ed.), Sabiston Textbook of Surgery (The Biological Basis of Modern Surgical Practice), Guyton & Hall Textbook of Medical Physiology (14th ed.), Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), Schwartz's Principles of Surgery (11th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.