Explain complete Anatomy of GI tract for mbbs 1st year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
GI tract gastrointestinal anatomy overview diagram
Reading File
Searching Images
stomach anatomy parts regions relations
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
large intestine colon rectum anal canal anatomy diagram
I now have comprehensive content from Gray's Anatomy for Students. Let me compile the full, structured answer for an MBBS 1st year student.
Complete Anatomy of the Gastrointestinal (GI) Tract — MBBS 1st Year
Source: Gray's Anatomy for Students; Color Atlas of Human Anatomy Vol. 2 (Internal Organs)
Overview
The gastrointestinal (GI) tract is a continuous muscular tube extending from the oral cavity to the anus (~9 m in total). It is responsible for ingestion, mechanical digestion, chemical digestion, absorption of nutrients, and elimination of waste.
Divisions of the GI tract:
| Region | Parts |
|---|---|
| Mouth & Pharynx | Oral cavity, pharynx |
| Foregut | Esophagus, stomach, duodenum (upper half), liver, gallbladder, pancreas |
| Midgut | Duodenum (lower half), jejunum, ileum, cecum, appendix, ascending colon, proximal 2/3 transverse colon |
| Hindgut | Distal 1/3 transverse colon, descending colon, sigmoid colon, rectum, upper anal canal |
1. Esophagus
Overview
A muscular tube ~25 cm long passing between the pharynx and stomach.
- Begins: Lower border of cricoid cartilage — vertebral level C6
- Ends: Cardiac opening of stomach — vertebral level T11
- Passes through: neck → posterior mediastinum → esophageal hiatus in diaphragm (T10)
Course & Relations
- Lies anterior to vertebral column, posterior to trachea (in neck/superior mediastinum)
- In the superior mediastinum: crossed by the arch of the aorta (left) and azygos vein (right)
- In the posterior mediastinum: lies posterior to the left atrium (clinically important — esophageal compression can affect cardiac imaging)
- As it reaches the diaphragm, it deflects anteriorly and to the left
Constrictions (4 sites — clinically important for lodged objects and corrosive injuries)
- Pharyngoesophageal junction (cricopharyngeus) — level C6
- Crossed by the arch of the aorta — T4/5
- Compressed by the left main bronchus — T4/5
- Passage through the esophageal hiatus — T10
Blood Supply
- Cervical: Inferior thyroid arteries
- Thoracic: Esophageal branches of thoracic aorta + bronchial arteries
- Abdominal: Left gastric artery (branch of celiac trunk)
Venous Drainage
- → Azygos/hemiazygos veins (systemic) + left gastric vein (portal)
- Portosystemic anastomosis at the lower esophagus → site of esophageal varices in portal hypertension
Innervation
- Parasympathetic: Vagus nerve (CN X) — forms the esophageal plexus which reconstitutes as anterior (left) and posterior (right) vagal trunks below the diaphragm
- Sympathetic: T5–T10 via greater splanchnic nerve
2. Peritoneum & Mesenteries
Before the abdominal organs — an understanding of the peritoneum is essential.
- Parietal peritoneum: lines the abdominal wall; innervated by spinal nerves T7–L1 (sensitive to well-localized pain)
- Visceral peritoneum: covers the organs; innervated by autonomic nerves (pain is poorly localized, referred)
- Peritoneal cavity: potential space between parietal and visceral layers; closed in men, semi-open in women (via uterine tubes)
Classification of Organs
| Type | Meaning | Examples |
|---|---|---|
| Intraperitoneal | Covered almost entirely by peritoneum; suspended by mesentery | Stomach, jejunum, ileum, transverse colon, sigmoid colon |
| Retroperitoneal (primary) | Never had a mesentery | Kidneys, aorta, IVC |
| Retroperitoneal (secondary) | Initially intraperitoneal, later fused to posterior wall | Duodenum (2nd–4th), ascending & descending colon, pancreas |
Key Peritoneal Folds
- Greater omentum: hangs from greater curvature of stomach; acts as "policeman of abdomen" (limits infection spread)
- Lesser omentum: connects lesser curvature of stomach + duodenum to liver (hepatogastric + hepatoduodenal ligaments)
- Mesentery proper: fan-shaped fold suspending jejunum and ileum; root runs from duodenojejunal flexure (L2 left) to ileocecal junction (right iliac fossa)
- Transverse mesocolon: suspends transverse colon
- Sigmoid mesocolon: suspends sigmoid colon
- Epiploic foramen (Foramen of Winslow): communication between greater and lesser peritoneal sacs
3. Stomach
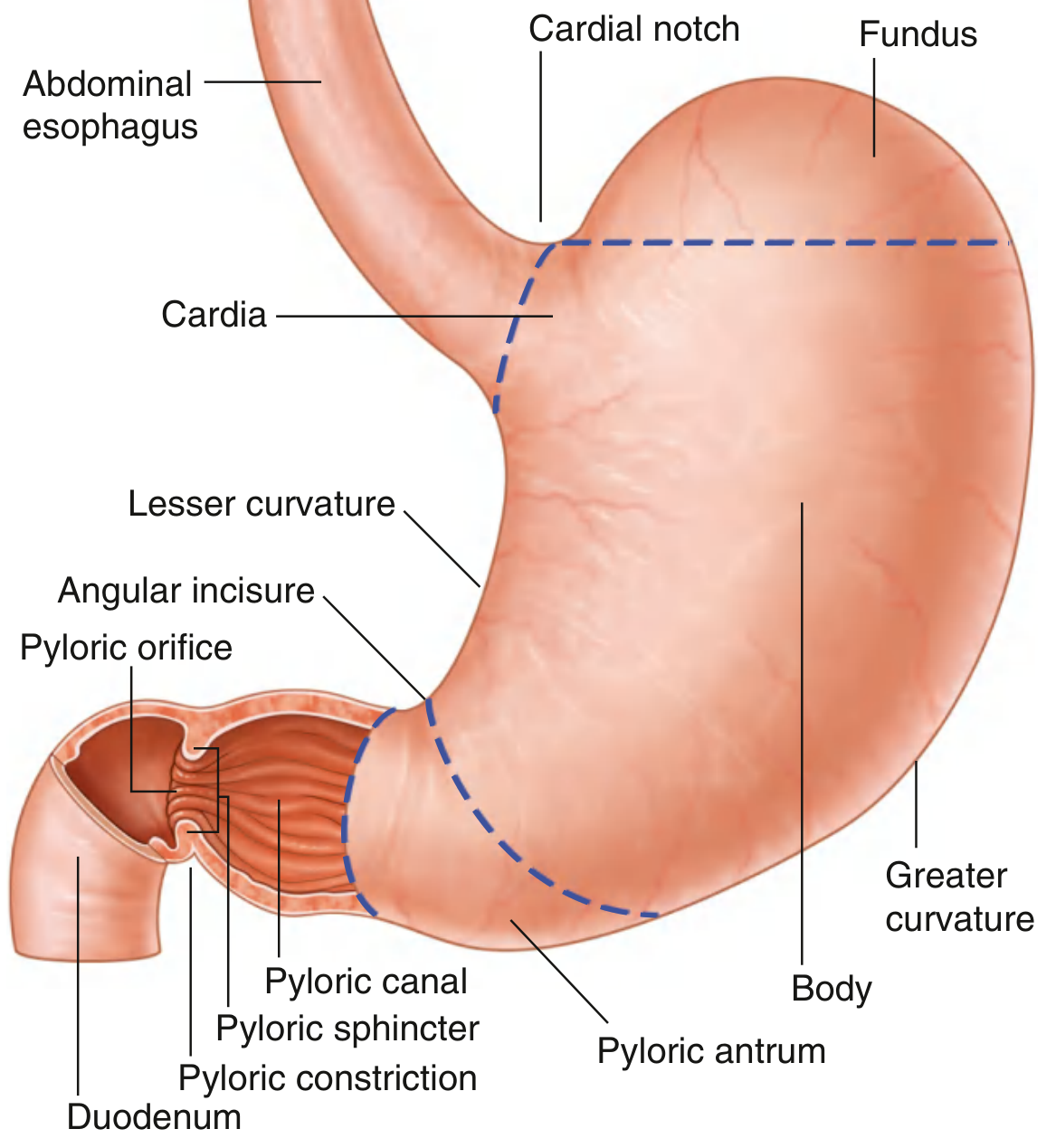
Overview
The most dilated part of the GI tract. J-shaped, located in the epigastric, umbilical, and left hypochondrium regions.
Parts (4)
| Part | Details |
|---|---|
| Cardia | Surrounds the esophagogastric (cardiac) orifice |
| Fundus | Dome above the level of the cardiac orifice; contains swallowed air (gastric bubble on X-ray) |
| Body | Largest part |
| Pyloric part | Consists of pyloric antrum + pyloric canal; ends at pylorus |
Pylorus: Marked by the pyloric constriction; contains the pyloric sphincter (thickened circular muscle). The pyloric orifice lies just right of midline at vertebral level L1 (transpyloric plane).
Curvatures
- Greater curvature (left/inferior): attachment of gastrosplenic ligament and greater omentum
- Lesser curvature (right/superior): attachment of lesser omentum
- Cardiac notch (angle of His): angle between esophagus and fundus
- Angular incisure (incisura angularis): bend on lesser curvature marking pyloric antrum
Blood Supply — all from celiac trunk
| Artery | Source | Region |
|---|---|---|
| Left gastric | Celiac trunk directly | Lesser curvature (left) |
| Right gastric | Hepatic artery proper | Lesser curvature (right) |
| Left gastro-omental (gastroepiploic) | Splenic artery | Greater curvature (left) |
| Right gastro-omental (gastroepiploic) | Gastroduodenal artery | Greater curvature (right) |
| Short gastric arteries (5–7) | Splenic artery | Fundus |
Venous Drainage → Hepatic Portal System
- Right and left gastric veins → portal vein
- Short gastric + left gastro-omental veins → splenic vein
- Right gastro-omental vein → superior mesenteric vein
Lymphatics
Broadly drain to celiac lymph nodes; subgroups follow arterial supply.
Innervation
- Parasympathetic (secretomotor + motor): Anterior vagal trunk (left vagus) + posterior vagal trunk (right vagus)
- Sympathetic (inhibitory + vasomotor): T6–T9 via greater splanchnic nerve → celiac plexus
- Pain from stomach is referred to the epigastrium
4. Small Intestine (~6–7 m)
4A. Duodenum
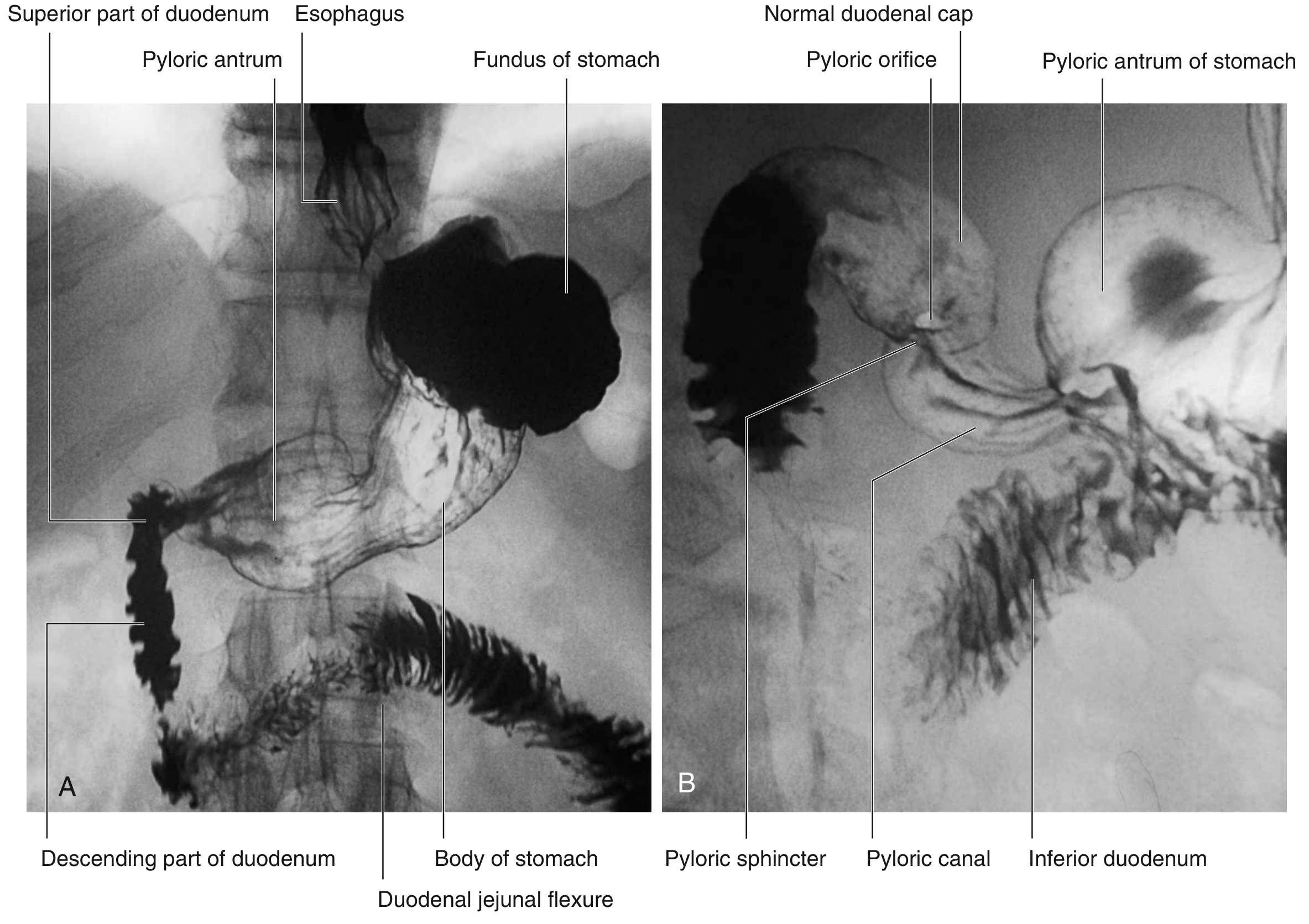
C-shaped, 20–25 cm, widest lumen of small intestine. Mostly retroperitoneal (except the first 2 cm). Wraps around the head of the pancreas.
4 Parts:
| Part | Vertebral Level | Key Relations |
|---|---|---|
| Superior (1st) | L1 | Begins at pylorus; duodenal cap (ampulla) — most ulcers here; anterior to portal vein, bile duct, gastroduodenal artery |
| Descending (2nd) | L1–L3 | Contains major duodenal papilla (opening of bile + pancreatic ducts) & minor duodenal papilla (accessory pancreatic duct); anterior: transverse colon; posterior: right kidney |
| Horizontal/Inferior (3rd) | L3 | Crosses IVC, aorta, vertebral column; crossed anteriorly by superior mesenteric artery and vein |
| Ascending (4th) | L2–L3 | Ascends to duodenojejunal (DJ) flexure; anchored by Ligament of Treitz (suspensory muscle of duodenum) |
DJ flexure = transition from foregut/midgut; lies to the left of L2, at same level as pylorus.
Blood supply:
- Above major papilla (foregut): Superior pancreaticoduodenal artery (from gastroduodenal artery — celiac trunk)
- Below major papilla (midgut): Inferior pancreaticoduodenal artery (from superior mesenteric artery)
4B. Jejunum
- Makes up proximal 2/5 of the jejuno-ileal loop (~2.5 m)
- Located mostly in the left upper quadrant
- Features: Wider diameter, thicker walls, more prominent plicae circulares (valvulae conniventes), longer vasa recta, fewer arterial arcades, deeper red color
- Blood supply: Jejunal branches of the superior mesenteric artery (SMA)
4C. Ileum
- Makes up distal 3/5 (~3.5 m)
- Located mostly in the right lower quadrant
- Features: Narrower, thinner walls, fewer and less prominent plicae circulares, shorter vasa recta, more arterial arcades, more mesenteric fat, Peyer's patches (lymphoid follicles — especially prominent in distal ileum)
- Ends at ileocecal junction in right iliac fossa
- Blood supply: Ileal branches of SMA
Jejunum vs. Ileum (exam comparison):
| Feature | Jejunum | Ileum |
|---|---|---|
| Position | LUQ | RLQ |
| Calibre | Wider | Narrower |
| Wall | Thicker | Thinner |
| Plicae circulares | Prominent | Few/absent distally |
| Vasa recta | Long | Short |
| Arterial arcades | Fewer (1–2) | More (4–5) |
| Peyer's patches | Rare | Numerous |
| Mesenteric fat | Less | More |
5. Large Intestine (~1.5 m)
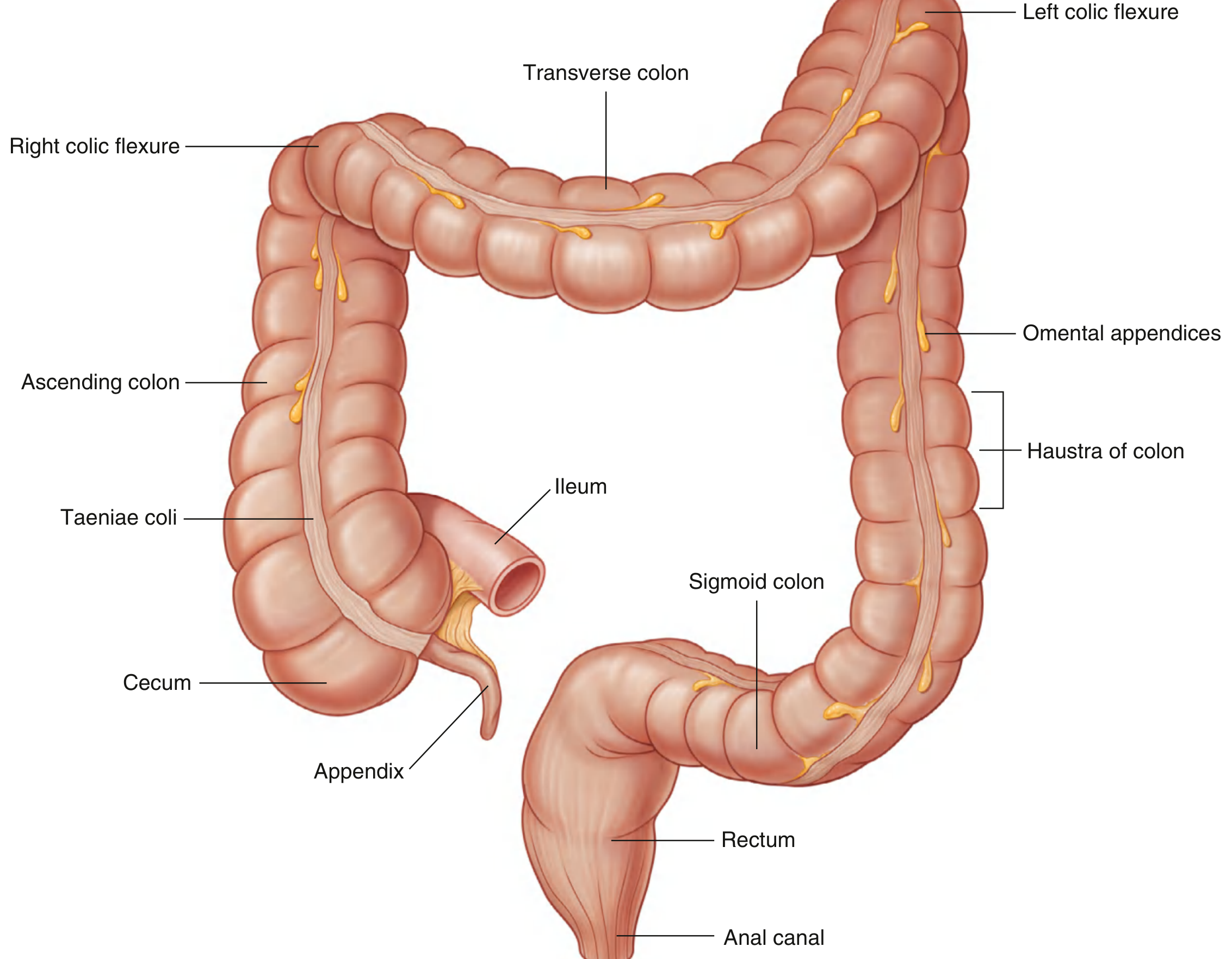
Extends from distal ileum to anus. Functions: water absorption, electrolyte absorption, vitamin K production (by bacteria), storage and elimination of feces.
Distinguishing features of the large intestine:
- Taeniae coli: 3 longitudinal bands of muscle (converge at appendix and merge into continuous layer at rectum)
- Haustra: sacculations between taeniae
- Omental (epiploic) appendices: fatty peritoneal tags attached to colon
5A. Cecum
- First part of large intestine, in right iliac fossa
- Intraperitoneal but usually has no mesentery
- Receives the ileum via the ileocecal valve (ileocecal fold)
- The three taeniae coli converge here → point to the appendix base
5B. Vermiform Appendix
- Blind-ended tube, 2–20 cm long (average 9 cm)
- Base: at the confluence of the three taeniae coli, at the posteromedial wall of cecum, McBurney's point (junction of lateral 1/3 and medial 2/3 of line from ASIS to umbilicus) — site of tenderness in appendicitis
- Position varies: retrocecal (most common ~65%), pelvic, pre-ileal, post-ileal
- Blood supply: Appendicular artery (branch of ileocolic artery from SMA), runs in mesoappendix
- Clinical: Appendicitis pain referred to umbilicus initially (T10 dermatome), then localizes to RIF
5C. Colon
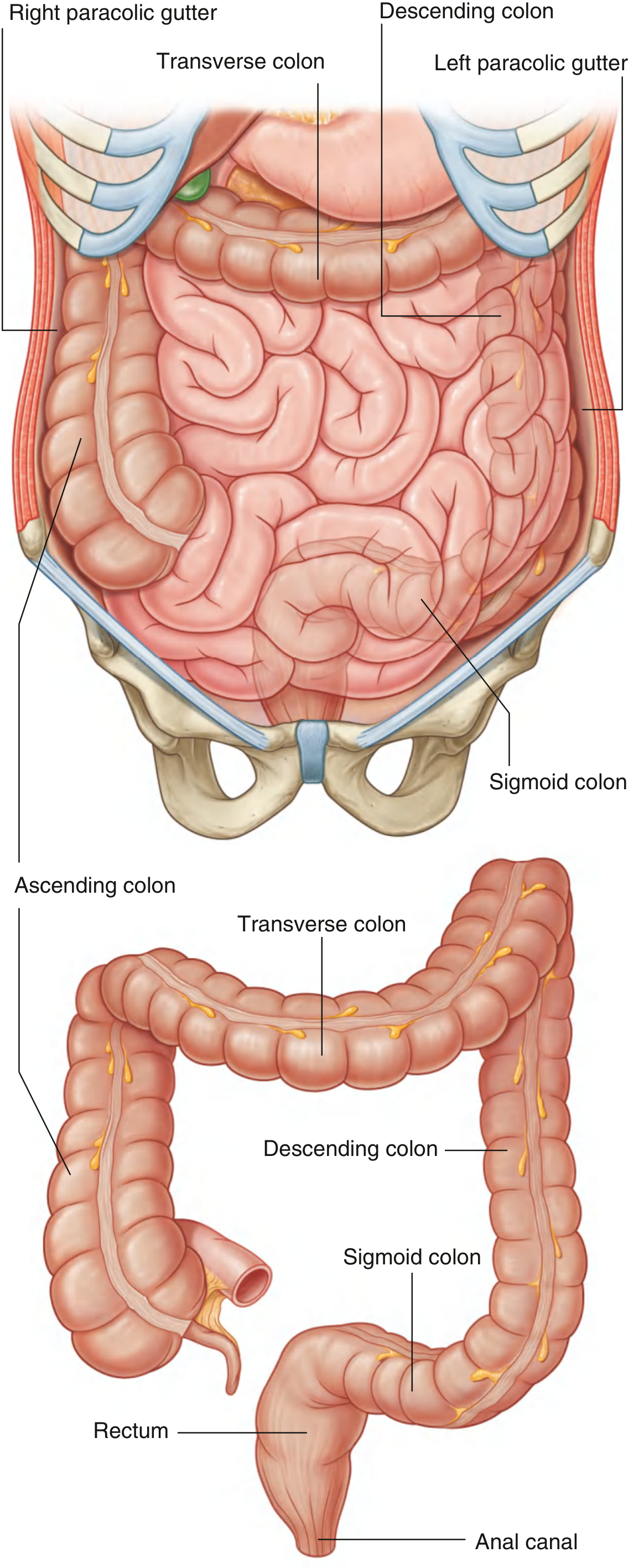
| Part | Peritoneal Status | Location | Blood Supply |
|---|---|---|---|
| Ascending colon | Secondarily retroperitoneal | Right flank (right iliac fossa → right hypochondrium) | Ileocolic + right colic arteries (SMA) |
| Right colic (hepatic) flexure | — | Below right lobe of liver | — |
| Transverse colon | Intraperitoneal (transverse mesocolon) | Crosses abdomen at umbilical level | Right + middle colic (SMA); left colic (IMA) |
| Left colic (splenic) flexure | — | Below spleen; higher + more posterior than hepatic flexure; anchored by phrenicocolic ligament | — |
| Descending colon | Secondarily retroperitoneal | Left flank | Left colic artery (IMA) |
| Sigmoid colon | Intraperitoneal (sigmoid mesocolon) | Left iliac fossa → pelvic inlet → S2 | Sigmoid arteries (IMA) |
Paracolic gutters: grooves between lateral margins of ascending/descending colon and the posterolateral abdominal wall — clinically important routes for spread of infection/ascites.
Marginal artery of Drummond: anastomosis between branches of SMA and IMA running along the colon — clinically important in colonic surgery.
5D. Rectum
- Begins at S2–S3 (rectosigmoid junction), 12–15 cm long
- Has 3 lateral flexures externally and 3 transverse (Houston's) folds internally
- No taeniae coli (smooth external longitudinal muscle layer)
- Peritoneal coverage: upper 1/3 covered anteriorly and laterally; middle 1/3 only anteriorly; lower 1/3 extraperitoneal
- Relations: Posterior = sacrum/coccyx; Anterior in men = bladder, seminal vesicles, prostate; Anterior in women = uterus, vagina
5E. Anal Canal (~4 cm)
- Begins at the anorectal junction (anorectal ring, pelvic diaphragm level), ends at the anus
- Pectinate (dentate) line (at level of anal valves): most important anatomical landmark
| Feature | Above dentate line | Below dentate line |
|---|---|---|
| Embryological origin | Endoderm (hindgut) | Ectoderm (proctodeum) |
| Epithelium | Columnar | Stratified squamous |
| Arterial supply | Superior rectal (IMA) | Inferior rectal (pudendal) |
| Venous drainage | Superior rectal → IMV → portal | Inferior rectal → internal pudendal → internal iliac → IVC |
| Lymph drainage | Internal iliac nodes | Superficial inguinal nodes |
| Sensation | Visceral (autonomic) — painless | Somatic (pudendal nerve) — painful |
- Internal anal sphincter: smooth muscle (involuntary), thickening of circular layer of muscularis
- External anal sphincter: skeletal muscle (voluntary), supplied by pudendal nerve (S2, S3, S4) + perineal branch of S4
6. Blood Supply Summary
Three Unpaired Branches of the Abdominal Aorta
| Artery | Vertebral Level | Territory |
|---|---|---|
| Celiac trunk | T12/L1 (upper border of L1) | Foregut: abdominal esophagus, stomach, duodenum (1st & 2nd parts), liver, gallbladder, spleen, pancreas |
| Superior mesenteric artery (SMA) | L1 (lower border) | Midgut: duodenum (3rd & 4th parts), jejunum, ileum, cecum, appendix, ascending colon, proximal 2/3 transverse colon |
| Inferior mesenteric artery (IMA) | L3 | Hindgut: distal 1/3 transverse colon, descending colon, sigmoid colon, rectum, upper anal canal |
Venous Drainage — Hepatic Portal System
All venous blood from the GI tract drains through the liver via the hepatic portal vein before reaching the systemic circulation.
Portal vein formation: Superior mesenteric vein + splenic vein (at L2 behind the neck of pancreas)
- Inferior mesenteric vein → splenic vein
- Formed behind the neck of the pancreas at vertebral level L2
Portosystemic (Portocaval) Anastomoses — exam favorite!
| Site | Portal tributary | Systemic tributary | Clinical result |
|---|---|---|---|
| Lower esophagus | Left gastric vein | Azygos veins | Esophageal varices |
| Anorectal junction | Superior rectal vein | Inferior/middle rectal veins | Anorectal varices |
| Paraumbilical | Paraumbilical veins (via round ligament) | Epigastric veins | Caput medusae |
| Bare area of liver | Portal tributaries | Diaphragmatic/phrenic veins | Enlarged collaterals |
| Retroperitoneal gut | Colic/intestinal veins | Lumbar/renal veins | Dilated retroperitoneal vessels |
7. Lymphatic Drainage
| Region | Primary Nodes | Converge To |
|---|---|---|
| Stomach | Gastric, gastro-omental nodes | Celiac nodes |
| Small intestine | Mesenteric nodes (along SMA) | Preaortic nodes → cisterna chyli |
| Large intestine | Paracolic → epicolic → intermediate colic nodes | Celiac/superior/inferior mesenteric nodes → preaortic |
| Rectum (upper) | Inferior mesenteric nodes | Preaortic |
| Anal canal (below dentate) | Superficial inguinal nodes | External iliac |
8. Innervation
| Type | Source | Effect |
|---|---|---|
| Sympathetic | T5–L2 (prevertebral ganglia: celiac, SMA, IMA ganglia) | Inhibits peristalsis; vasoconstriction; contracts sphincters; transmits pain |
| Parasympathetic | Vagus (CN X): foregut + midgut; Pelvic splanchnic nerves (S2–S4): hindgut | Stimulates peristalsis, secretion; relaxes sphincters |
| Enteric NS | Myenteric (Auerbach's) + submucosal (Meissner's) plexuses | Intrinsic regulation; "gut brain" |
Referred pain patterns:
- Foregut (stomach, duodenum) → epigastrium
- Midgut (small intestine, appendix) → periumbilical/umbilical region
- Hindgut (large intestine) → hypogastrium
9. Histology of the GI Wall (General Layers)
From lumen outward:
- Mucosa — epithelium + lamina propria + muscularis mucosae
- Submucosa — dense CT, Meissner's (submucosal) plexus, blood vessels
- Muscularis externa — inner circular + outer longitudinal smooth muscle; Auerbach's (myenteric) plexus between them
- Adventitia / Serosa — CT covering; serosa where covered by peritoneum
10. Developmental Anatomy (Gut Rotation)
- The gut tube develops from endoderm (epithelium) + splanchnic mesoderm (muscle, CT, peritoneum)
- Foregut: supplied by celiac artery; derivatives: esophagus–liver–pancreas
- Midgut: herniates into umbilical cord at week 6, rotates 270° counterclockwise around SMA axis, returns to abdomen at week 10
- Hindgut: descends into pelvis; cloaca is divided into urogenital sinus (anterior) and anorectal canal (posterior) by the urorectal septum
- Clinical: Malrotation and midgut volvulus can cause acute bowel ischemia — surgical emergency
Quick Revision Summary Table
| Organ | Length | Peritoneal status | Blood supply | Vertebral level |
|---|---|---|---|---|
| Esophagus (abdominal) | ~1–2 cm | Intraperitoneal | Left gastric | T11 |
| Stomach | Variable | Intraperitoneal | Celiac branches | T10–L1 |
| Duodenum | 20–25 cm | Secondarily retroperitoneal (except 1st 2 cm) | Celiac + SMA | L1–L3 |
| Jejunum | ~2.5 m | Intraperitoneal | SMA | — |
| Ileum | ~3.5 m | Intraperitoneal | SMA | — |
| Cecum | 6–8 cm | Intraperitoneal | SMA (ileocolic) | Right iliac fossa |
| Appendix | 2–20 cm | Intraperitoneal (mesoappendix) | SMA (appendicular) | — |
| Ascending colon | ~15 cm | Secondarily retroperitoneal | SMA | — |
| Transverse colon | ~50 cm | Intraperitoneal | SMA + IMA | — |
| Descending colon | ~25 cm | Secondarily retroperitoneal | IMA | — |
| Sigmoid colon | ~40 cm | Intraperitoneal | IMA | — |
| Rectum | 12–15 cm | Extraperitoneal (lower 2/3) | IMA + internal iliac | S2–S3 |
| Anal canal | ~4 cm | Extraperitoneal | IMA (above) / Pudendal (below) | — |
Gray's Anatomy for Students (9780323934237); Color Atlas of Human Anatomy Vol. 2 Internal Organs (9783132424487)
This is a shared conversation. Sign in to Orris to start your own chat.