Male type alopecia
Reading File
Finding Sources
Searching PubMed
"androgenetic alopecia" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of male-pattern alopecia (androgenetic alopecia, AGA) based on authoritative dermatology textbooks.
Male-Pattern Alopecia (Androgenetic Alopecia)
Definition
Androgenetic alopecia is the most common type of hair loss - a nonscarring, progressive miniaturization of the hair follicle with shortening of the anagen phase in genetically predisposed individuals, occurring in a characteristic pattern distribution. - Fitzpatrick's Dermatology, p. 1525
Epidemiology
- Approximately 50-60% of men are affected by age 50, rising to ~80% by age 70.
- Prevalence and severity are lower in Asians and Native Americans compared to Europeans (only ~10-20% of Chinese men are affected by age 40-49).
- Onset can occur at any time after puberty. - Fitzpatrick's Dermatology, p. 1525
Pathophysiology
The process involves a triad of genetic predisposition, androgens, and time:
- Androgenic drive: The 5α-reductase enzyme (especially type 2 isoenzyme) converts testosterone to dihydrotestosterone (DHT) in the scalp. DHT binds androgen receptors on dermal papilla cells, triggering follicular miniaturization.
- Androgen receptor gene: Early-onset AGA (before age 30) is closely linked to the androgen receptor gene. Eunuchs castrated before puberty do not develop baldness; androgen therapy can induce it.
- Molecular mediators: Androgen-inducible TGF-β1 from dermal papilla cells suppresses hair growth. In congenital 5α-reductase type 2 deficiency, pattern baldness does not occur.
- Hair cycle changes: Progressive shortening of the anagen (growth) phase and lengthening of the kenogen (lag) phase result in progressively finer, shorter hairs until terminal hairs are replaced by vellus hairs.
- Polygenic inheritance: Suggested by high population prevalence, gaussian distribution, and increased risk with more affected relatives. - Andrews' Diseases of the Skin, p. 871-872
Hamilton-Norwood Classification
This is the standard staging system for male-pattern hair loss:
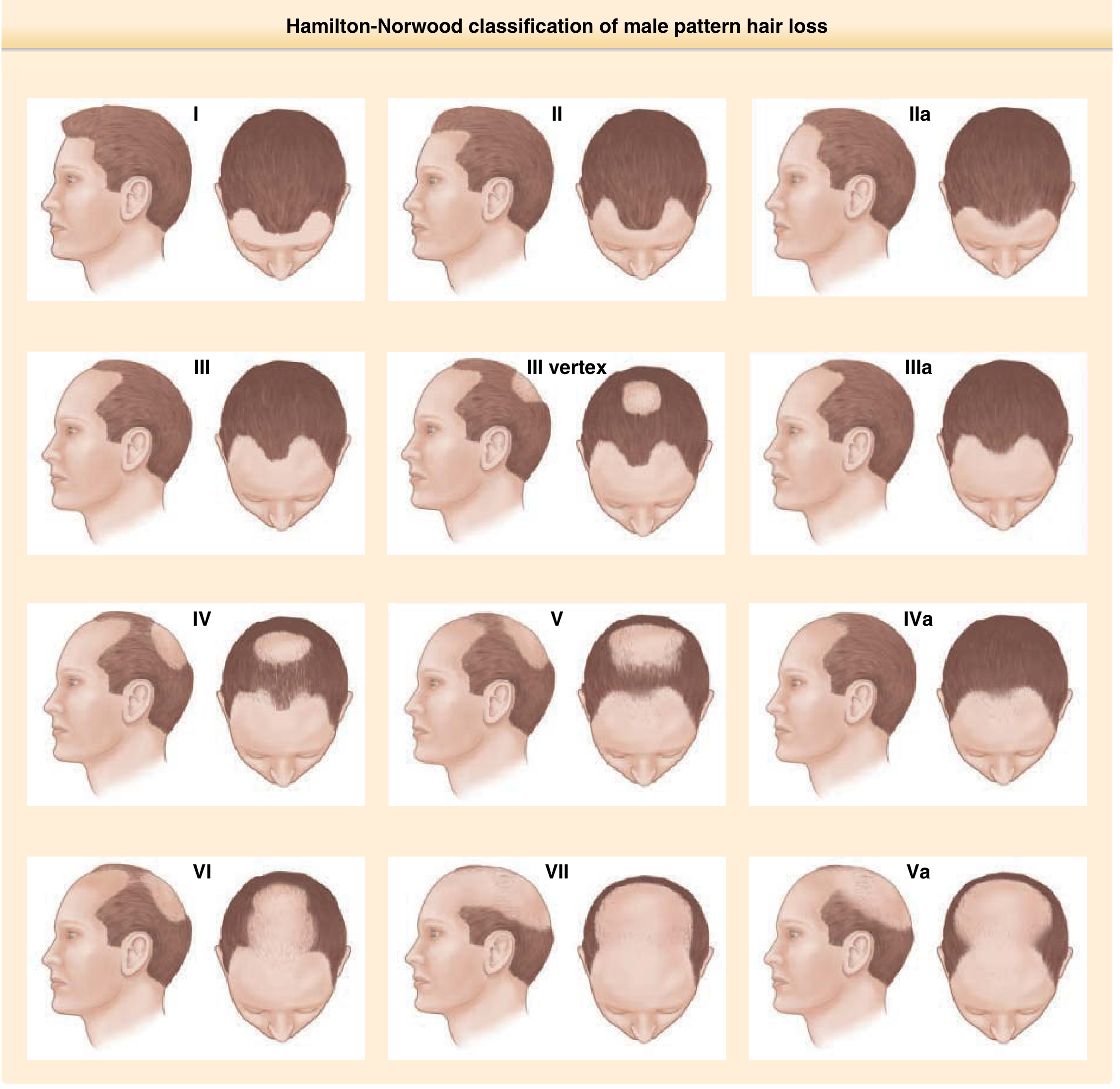
- Stage I: Minimal recession at the anterior hairline (normal)
- Stage II: Slight triangular recession at the frontotemporal corners (Geheimratswinkeln/"professor angles")
- Stage IIa: Anterior hairline recession deeper toward the vertex
- Stage III / III Vertex: More pronounced frontotemporal recession; vertex thinning begins
- Stage IV: Vertex bald spot enlarges; the frontal band separates from the vertex
- Stage V-VII: Progressive confluence of the frontal and vertex areas; only a rim of hair remains on the occipital and parietal sides
The occipital and parietal areas are permanently spared even in the most advanced stages. - Fitzpatrick's Dermatology, p. 1526
Clinical Features
- Begins in the teens, 20s, or 30s
- Anterior hairline recedes bilaterally at the frontotemporal corners
- The forehead progressively heightens; vertex hair thins
- Hair shafts show variable diameter (anisotrichosis) - a hallmark finding
- Rate of progression varies: some men lose hair rapidly then stabilize; others progress slowly over decades
- "Whisker" or kinky scalp hair may be an early sign - Andrews' Diseases of the Skin, p. 871
Histopathology
- Decreased anagen follicles, increased telogen follicles
- Follicular miniaturization and shaft diameter variability (most evident on transverse sections)
- Fibrous/fibro-mucinous tract remnants below miniaturized follicles
- Many mast cells in fibrous tracts; minimal lymphoid inflammation (if significant inflammation is present, consider a concurrent diagnosis)
- Sebaceous glands may appear relatively enlarged
- Sparse lymphoid infiltrate at the follicular infundibulum may represent seborrheic folliculitis - Andrews' Diseases of the Skin, p. 872
Diagnosis
Diagnosis is primarily clinical (history + examination). Additional workup may be needed to exclude differentials:
| Tool | Role |
|---|---|
| Dermoscopy/trichoscopy | Hair diameter variation, loss of trio groups, increased vellus hairs; excludes scarring alopecia |
| Hair pull test | >10% pulled = positive (active shedding); positive frontally, negative occipitally in AGA |
| Global photography | Standardized long-term monitoring |
| Biopsy | Rarely needed; indicated only if cicatricial alopecia or diffuse alopecia areata suspected |
| Labs | Ferritin, TSH (for diffuse effluvium); hormonal workup in women with hyperandrogenism signs |
- Fitzpatrick's Dermatology, p. 1528-1529
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Alopecia areata (diffuse) | Non-patterned; exclamation mark hairs; positive pull test globally |
| Lichen planopilaris | Perifollicular erythema/scale; scarring; histology shows lymphocytic destruction |
| Frontal fibrosing alopecia | Frontotemporal band-like scarring; loss of eyebrows; perifollicular inflammation |
| Traction alopecia | History of chronic tight hairstyles; reversible if caught early |
| Telogen effluvium | Diffuse shedding; often triggered by systemic stress; not patterned |
Management
1. Topical Minoxidil (First-line)
- Mechanism: Promotes dermal papilla cell survival, prolongs anagen, enlarges shaft diameter (likely via potassium channel opening)
- Dosing: 5% solution or foam - 1 mL (or half a cap of foam) twice daily
- Response assessment: At 6 months; continued indefinitely to maintain effect
- Best results: Early cases (<10 years duration), bald area <10 cm diameter, pretreatment density >20 hairs/cm²
- Side effects: Hypertrichosis (local spread), initial telogen shedding in first 8 weeks, contact dermatitis (from propylene glycol in 5% solution)
- Available OTC - Andrews' Diseases of the Skin, p. 871-872
2. Oral Finasteride (First-line in men)
- Mechanism: Selective 5α-reductase type 2 inhibitor; reduces scalp DHT levels
- Dosing: 1 mg/day orally
- Efficacy: Stops hair loss in up to 90% of men for at least 5 years; ~65% show measurable regrowth
- Time course: Visible results only after 6+ months; if no effect at 12 months, discontinue
- Side effects: Sexual dysfunction (reduced libido, erectile dysfunction) in a small minority; reduces PSA (must be considered when screening for prostate cancer)
- Finasteride + minoxidil combination is more effective than either alone - Andrews' Diseases of the Skin, p. 872
3. Dutasteride
- Blocks both type 1 and type 2 5α-reductase (broader DHT suppression than finasteride)
- More potent DHT reduction; used off-label for AGA in many countries - Andrews' Diseases of the Skin, p. 872
4. Low-Level Laser/LED Therapy
- A 2025 systematic review and meta-analysis (PMID 39404126) supports efficacy in alopecia; can be used as adjunctive therapy.
5. Microneedling
- A 2025 meta-analysis (PMID 40056230) shows combined microneedling therapy is superior to topical minoxidil alone, likely by enhancing drug penetration and stimulating growth factors.
6. Hair Transplantation
- Follicular unit grafting from the occipital donor area to the frontal scalp
- Best for stable, nonprogressive AGA with adequate donor supply
- Can recreate natural hairlines with excellent cosmetic results
- Not appropriate during active progression - Andrews' Diseases of the Skin, p. 872
7. Investigational / Emerging
- Platelet-rich plasma (PRP)
- Topical antiandrogens (fluridil)
- Topical adenosine
- JAK inhibitors (under investigation)
Key Points Summary
| Feature | Detail |
|---|---|
| Cause | DHT + genetic susceptibility (AR gene, polygenic) |
| Classification | Hamilton-Norwood (stages I-VII) |
| Histology | Follicular miniaturization, anagen shortening, fibrous tracts |
| First-line treatment | Minoxidil (topical) + Finasteride (oral) |
| Response time | 6-12 months minimum |
| Reversibility | Limited in advanced disease; early treatment is key |
Recent evidence note: A 2024 systematic review on micronutrients and AGA (PMID 39440586) highlights nutritional deficiencies (e.g., zinc, iron, vitamin D) as potential contributors - correcting deficiencies may support treatment outcomes, though they are not primary causes.
This is a shared conversation. Sign in to Orris to start your own chat.