In LFT what are the components present and what are their significant and their normal values. What indicates if they are abnormal and what are teh conditions
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative information to compose a complete answer. Let me put it all together.
Liver Function Tests (LFT) - Complete Overview
LFTs are a panel of blood tests used to assess the functional status of the liver, covering hepatocyte integrity, synthetic capacity, catabolic activity, and biliary excretion. The panel is often misnamed - not all components directly measure "function"; several are markers of injury.
Categories of LFT Components
LFT components fall into four functional groups:
| Category | Tests |
|---|---|
| Markers of hepatocyte injury | ALT, AST |
| Markers of cholestasis / bile duct injury | ALP, GGT |
| Markers of hepatic synthetic function | Albumin, Prothrombin Time (PT/INR) |
| Markers of catabolic / excretory function | Bilirubin (total, direct, indirect) |
| Additional (sometimes included) | Total protein, LDH, Ammonia |
1. Bilirubin
Normal values:
- Total bilirubin: 5-17 µmol/L (0.3-1.2 mg/dL)
- Direct (conjugated): < 0.3 mg/dL
- Indirect (unconjugated): < 0.8 mg/dL
Significance: Bilirubin is a breakdown product of haem proteins. In a functioning liver, unconjugated bilirubin is taken up by hepatocytes, conjugated with glucuronic acid, and secreted into bile.
Abnormal patterns and conditions:
| Pattern | Mechanism | Conditions |
|---|---|---|
| Raised total + raised indirect | Overwhelming supply OR impaired conjugation | Haemolytic anaemia, neonatal jaundice, Gilbert's syndrome, Crigler-Najjar syndrome |
| Raised total + raised direct | Obstruction to conjugated bilirubin excretion | Choledocholithiasis, pancreatic head carcinoma, cholangiocarcinoma, biliary atresia, primary biliary cholangitis |
| Both raised (mixed) | Combined hepatocellular damage | Acute viral hepatitis, alcoholic hepatitis, drug-induced liver injury, cirrhosis |
2. ALT (Alanine Aminotransferase)
Normal value: 5-40 IU/L
Significance: An intracellular enzyme found predominantly in hepatocytes. It is a more specific marker of hepatocyte injury than AST, since it is found mainly in the liver. Released into circulation when hepatocytes are damaged or necrotic.
Abnormal findings and conditions:
| Degree of elevation | Interpretation / Conditions |
|---|---|
| < 5x upper limit of normal (ULN) | Non-alcoholic fatty liver disease (NAFLD/NASH), alcoholic liver disease, chronic hepatitis |
| 5-10x ULN | Chronic active hepatitis, early acute hepatitis |
| > 10x ULN | Acute viral hepatitis, ischaemic hepatitis ("shock liver"), acetaminophen toxicity, acute Budd-Chiari |
| Near normal despite end-stage disease | Cirrhosis (hepatocytes largely destroyed - "burnt-out liver") |
3. AST (Aspartate Aminotransferase)
Normal value: 5-40 IU/L
Significance: Also released by injured hepatocytes, but less specific for the liver - also found in cardiac muscle, skeletal muscle, kidneys, and brain. Useful in combination with ALT.
Key ratios:
| Ratio | Interpretation |
|---|---|
| AST:ALT > 2:1 | Strongly suggests alcoholic hepatitis (alcohol stimulates AST production; pyridoxine deficiency disproportionately depresses ALT) |
| AST > ALT in chronic hepatitis | Suggests progression to cirrhosis |
| AST alone raised (normal ALT + normal GGT) | Consider myocardial infarction, skeletal muscle disease, rhabdomyolysis |
| AST and ALT both > 10,000 IU/L | Acute fulminant hepatic failure, ischaemic hepatitis |
4. ALP (Alkaline Phosphatase)
Normal value: 30-140 IU/L
Significance: Particularly elevated in cholestatic liver disease or biliary obstruction. ALP is also produced by bone, placenta, intestine, kidneys, and leukocytes - so elevation must be contextualised.
Abnormal findings and conditions:
| Degree of elevation | Interpretation / Conditions |
|---|---|
| Mild (up to 2x ULN) | Non-specific; seen in virtually all hepatobiliary disease; normal in pregnancy |
| > 4x ULN | Strongly suggests cholestasis - primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC), biliary obstruction (stones, stricture, tumour) |
| Raised ALP with normal GGT | Bone source - Paget's disease, prostate cancer, bone metastases, fractures, growing children |
| Raised ALP + raised GGT | Confirms hepatic / biliary origin |
5. GGT (Gamma-Glutamyl Transpeptidase)
Normal value: 10-48 IU/L (higher in males)
Significance: A sensitive but non-specific marker. Very useful as a confirmatory test alongside ALP to establish a hepatic origin. Its production is induced by alcohol and certain drugs.
Abnormal findings and conditions:
- Alcoholic liver disease - GGT is disproportionately elevated; raised GGT in the context of hepatitis strongly suggests alcohol as the cause
- Drug-induced enzyme induction - phenobarbitone, warfarin, anticonvulsants
- Can also rise in: acute/chronic pancreatitis, acute MI, COPD, rheumatoid arthritis, diabetes mellitus
- GGT is used to confirm that an elevated ALP is of hepatic rather than bony origin
6. Albumin
Normal value: 35-50 g/L (3.5-5 g/dL)
Significance: A protein synthesised exclusively by the liver. Reflects hepatic synthetic function. Has a half-life of approximately 3 weeks, making it most useful in chronic liver disease rather than acute disease.
Abnormal findings and conditions:
| Finding | Conditions |
|---|---|
| Hypoalbuminaemia (< 35 g/L) | Cirrhosis, chronic hepatitis, liver failure, alcoholic hepatitis |
| Low albumin with normal LFT enzymes | Malnutrition, nephrotic syndrome, protein-losing enteropathy (not always liver disease) |
| Progressive fall in albumin | Indicates deteriorating liver synthetic function in chronic liver disease |
7. Prothrombin Time (PT) / INR
Normal value: PT 12-16 seconds; INR 0.8-1.2
Significance: Reflects the liver's synthesis of vitamin K-dependent clotting factors (II, VII, IX, X). Factor VII has the shortest half-life (6 hours), so PT responds quickly to acute changes. This makes it more useful than albumin in acute liver disease.
Abnormal findings and conditions:
| Finding | Interpretation |
|---|---|
| Prolonged PT in acute hepatitis | Indicates widespread hepatocellular necrosis; suggests severe disease |
| PT corrects with IV Vitamin K (≥ 30% improvement in 24h) | Vitamin K deficiency (malabsorption), not true liver synthetic failure |
| PT does NOT correct with Vitamin K | True hepatic synthetic dysfunction |
| Markedly prolonged PT in cirrhosis | Progressive loss of synthetic capacity; poor prognosis |
| Prolonged PT + very high AST/ALT | Fulminant hepatic failure - medical emergency |
8. Total Protein
Normal value: 60-85 g/L (6-8.5 g/dL)
Consists of albumin + globulins. In chronic liver disease, albumin falls but globulins (immunoglobulins) often rise (the liver is immunocompromised and produces excess ineffective immunoglobulins) - so total protein may remain deceptively normal even when liver function is severely impaired.
9. LDH (Lactate Dehydrogenase)
A non-specific marker. Moderate elevations are seen in hepatocellular disorders and cirrhosis; purely cholestatic conditions cause minimal elevation. The isoenzyme LDH-5 is liver-specific but not widely used. Haemolysis raises both LDH and unconjugated bilirubin.
10. Ammonia
Normally metabolised by the liver (urea cycle). In hepatic failure, ammonia accumulates and causes hepatic encephalopathy. Very high levels in fulminant liver failure indicate poor prognosis.
Interpreting Patterns of Abnormality
The key to LFT interpretation is recognising the predominant pattern of abnormality:
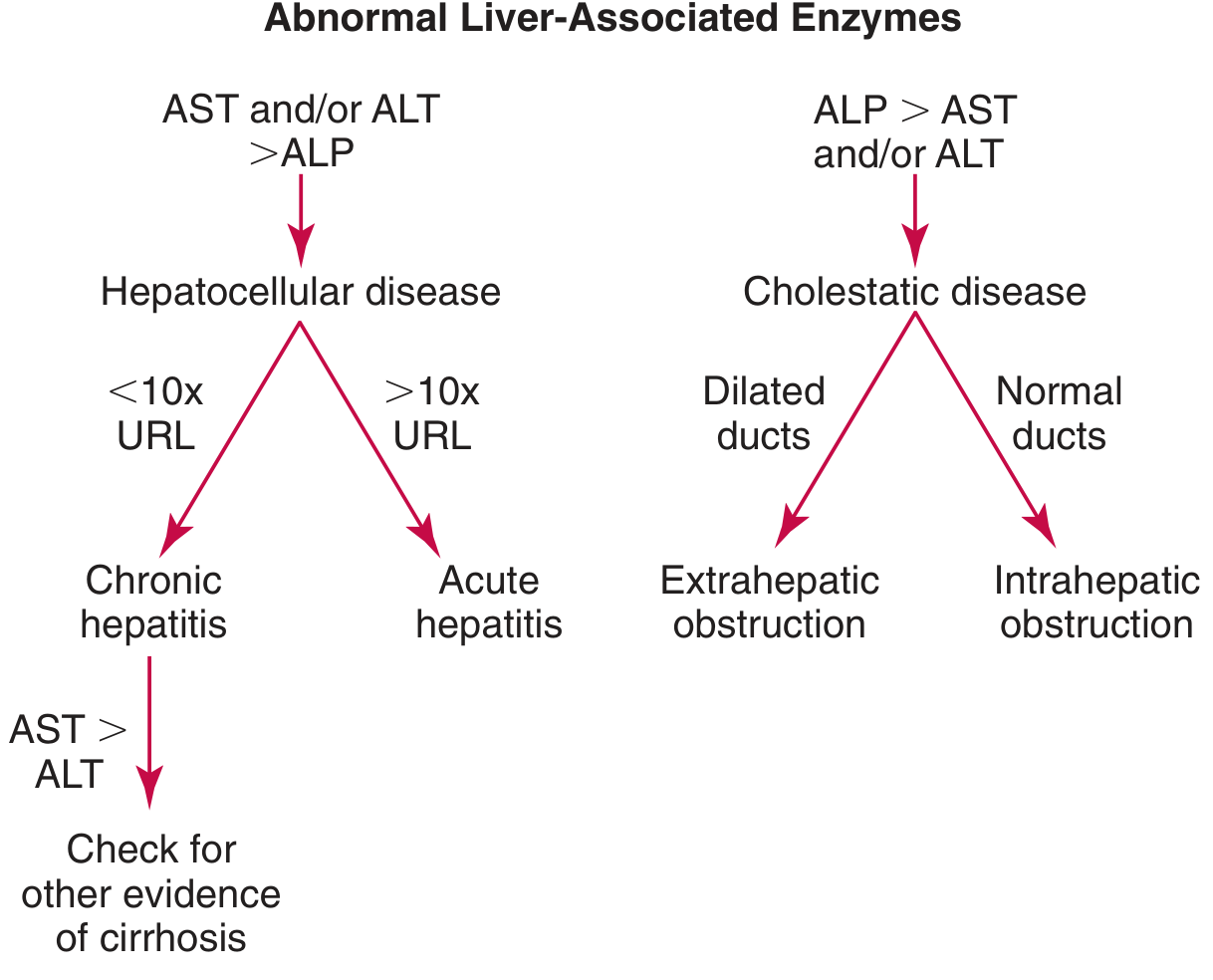
| Pattern | Predominant enzyme | Likely category | Examples |
|---|---|---|---|
| Hepatocellular | AST/ALT > ALP | Parenchymal injury | Viral hepatitis, alcoholic hepatitis, NAFLD, ischaemic hepatitis, drug toxicity, autoimmune hepatitis |
| - ALT/AST > 10x ULN | - | Acute hepatitis | Acute viral hepatitis, acetaminophen overdose, ischaemic hepatitis |
| - ALT/AST < 10x ULN | - | Chronic hepatitis | Chronic viral hepatitis, NAFLD, ALD |
| - AST:ALT > 2 | - | Alcoholic | Alcoholic hepatitis |
| - AST > ALT in chronic disease | - | Cirrhosis | Advanced fibrosis/cirrhosis |
| Cholestatic | ALP > AST/ALT | Bile duct injury | Biliary obstruction, PBC, PSC, cholangitis |
| - Dilated ducts on imaging | - | Extrahepatic obstruction | Gallstones, pancreatic carcinoma, cholangiocarcinoma |
| - Normal ducts on imaging | - | Intrahepatic cholestasis | PBC, PSC, drug-induced cholestasis, intrahepatic cholestasis of pregnancy |
| Synthetic failure | Low albumin + prolonged PT | Liver synthetic failure | Cirrhosis, acute liver failure, chronic hepatitis |
| Mixed | All components elevated | Combined pattern | Decompensated cirrhosis, severe acute hepatitis |
Quick Reference: Normal Values Summary
| Test | Normal Range | Reflects |
|---|---|---|
| Total Bilirubin | 0.3-1.2 mg/dL (5-17 µmol/L) | Excretory/catabolic function |
| Direct Bilirubin | < 0.3 mg/dL | Conjugation + excretion |
| Indirect Bilirubin | < 0.8 mg/dL | Haem breakdown + uptake |
| ALT | 5-40 IU/L | Hepatocyte injury (liver-specific) |
| AST | 5-40 IU/L | Hepatocyte injury (non-specific) |
| ALP | 30-140 IU/L | Biliary / cholestasis |
| GGT | 10-48 IU/L | Biliary + alcohol marker |
| Albumin | 35-50 g/L | Synthetic function (chronic) |
| Total Protein | 60-85 g/L | General protein status |
| PT | 12-16 seconds | Synthetic function (acute) |
| INR | 0.8-1.2 | Clotting factor synthesis |
Sources: Bailey and Love's Short Practice of Surgery (28th Ed.), Tintinalli's Emergency Medicine, Tietz Textbook of Laboratory Medicine (7th Ed.), Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.