According to hba1c level treatment of dm
Reading File
Finding Sources
Searching PubMed
"HbA1c" AND "diabetes mellitus" AND "glycemic targets"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Now I have comprehensive material. Here is the complete answer:
DM Treatment Based on HbA1c Level
What is HbA1c and Why It Guides Treatment
HbA1c (glycated hemoglobin) reflects average plasma glucose over the preceding 8-12 weeks, since red blood cells live up to 120 days. It is the cornerstone for both diagnosing diabetes and monitoring how well treatment is working.
Diagnostic thresholds (ADA criteria):
| HbA1c | Interpretation |
|---|---|
| < 5.7% | Normal |
| 5.7 - 6.4% | Prediabetes |
| ≥ 6.5% | Diabetes mellitus (confirm with repeat test) |
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
HbA1c Treatment Targets
| Patient Group | HbA1c Target |
|---|---|
| Most adults with T2DM | < 7.0% (53 mmol/mol) |
| Young, healthy, no hypoglycemia risk | < 6.5% |
| Elderly, comorbidities, limited life expectancy | < 8.0% (less stringent) |
| Pregnant women with DM | < 6.0 - 6.5% |
The ADA states that the goal of treatment is to keep HbA1c as close to normal as safely possible, because there is no specific value below which complications are completely eliminated.
- Tietz Textbook of Laboratory Medicine, 7th Ed.
Treatment Algorithm Based on HbA1c
Step 1 - All patients at diagnosis
Lifestyle modification + Metformin (first-line unless contraindicated)
- Metformin: initial 500 mg twice daily, range 500-2500 mg/day
- Lowers HbA1c by ~1.5%
Step 2 - If HbA1c remains above target, add a second agent (choice depends on comorbidities):
Flowchart from Goldman-Cecil Medicine:
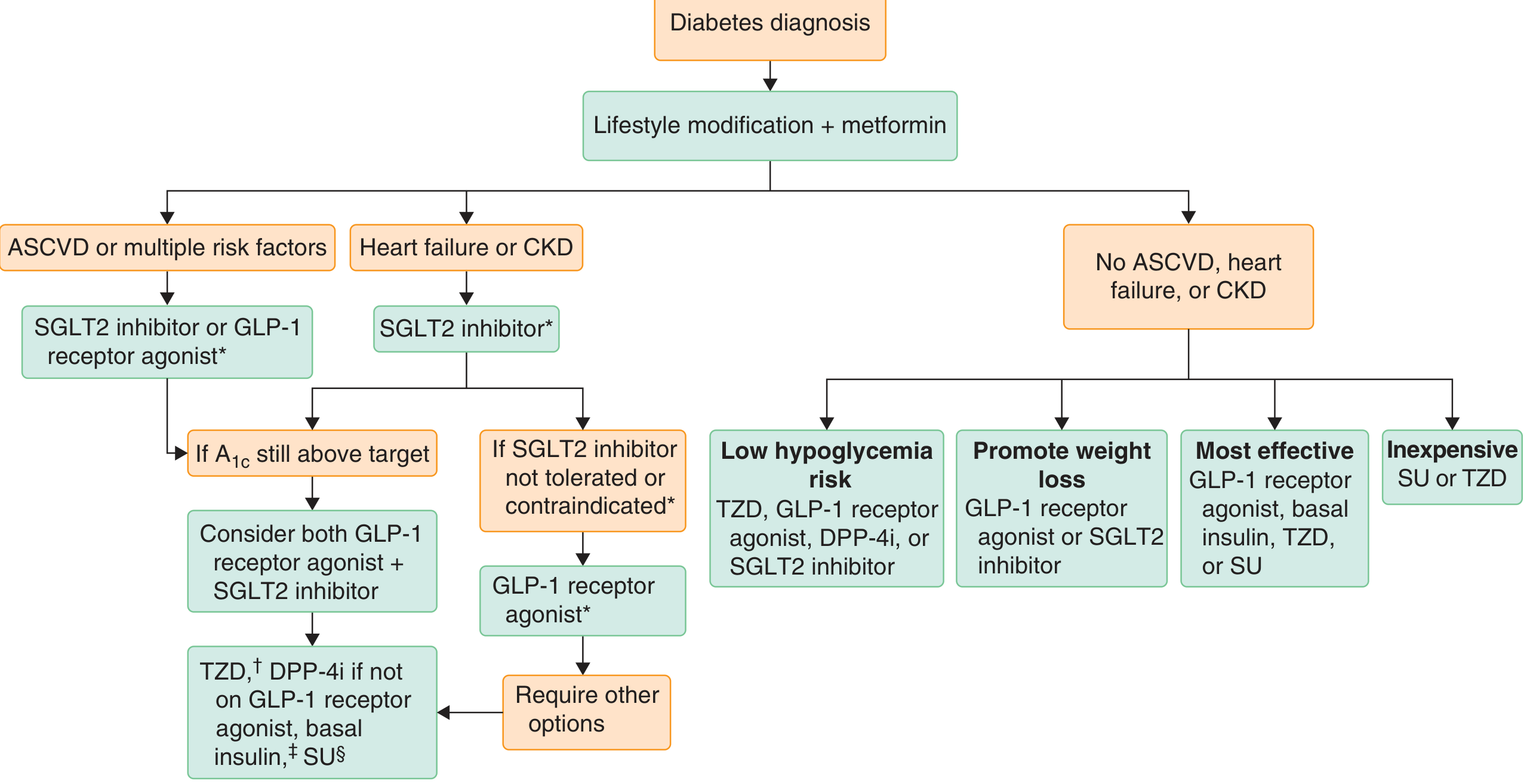
Drug Selection by Clinical Context
| Comorbidity / Priority | Preferred Add-on |
|---|---|
| ASCVD or high CV risk | SGLT2 inhibitor or GLP-1 receptor agonist |
| Heart failure or CKD | SGLT2 inhibitor (preferred); if not tolerated → GLP-1 RA |
| Minimize hypoglycemia risk | TZD, GLP-1 RA, DPP-4i, or SGLT2 inhibitor |
| Promote weight loss | GLP-1 RA or SGLT2 inhibitor |
| Most effective glycemic lowering | GLP-1 RA, basal insulin, TZD, or SU |
| Cost-conscious | Sulfonylurea (SU) or TZD |
- Goldman-Cecil Medicine, International Edition
Step 3 - Specific HbA1c-Based Intensification
HbA1c 7-9% (above target, no symptoms):
- Add second or third oral agent
- Options: SGLT2 inhibitor, GLP-1 RA, DPP-4 inhibitor, TZD, or sulfonylurea
HbA1c ≥ 9.0% with symptomatic hyperglycemia (polyuria, polydipsia, weight loss):
- Consider short-term intensive insulin therapy (2 weeks to 3 months)
- This can help "rest" the beta cells and improve subsequent oral agent response
- Goldman-Cecil Medicine
HbA1c persistently above target despite multiple agents:
- Add basal insulin (e.g., insulin glargine, degludec)
- If still inadequate, intensify to basal-bolus insulin regimen
HbA1c Reduction Expected from Each Drug Class
| Drug Class | HbA1c Reduction |
|---|---|
| Metformin | ~1.5% |
| GLP-1 receptor agonists | ~1.0-1.2% |
| Oral semaglutide | ~0.8-1.3% |
| Tirzepatide (GIP + GLP-1 agonist) | > GLP-1 RA alone (most potent) |
| SGLT2 inhibitors | ~0.5-1.0% |
| TZDs (e.g., pioglitazone) | ~1.0% |
| DPP-4 inhibitors | ~0.6-0.8% |
| Sulfonylureas | ~1.0-1.5% |
| Insulin (basal) | Variable, titrated to target |
- Goldman-Cecil Medicine; Katzung's Pharmacology, 16th Ed.
Type 1 DM
- Insulin is mandatory - no oral agents replace it
- Basal-bolus regimen is the standard
- HbA1c target: < 7.0% for most; some guidelines accept < 7.5% if hypoglycemia is a concern
- Recent meta-analysis (PMID: 40852189, 2025) confirmed GLP-1 agonists reduce HbA1c and insulin dose in T1DM as an adjunct
Key Points
-
HbA1c is checked every 3 months when treatment is being adjusted, then every 6 months once stable
-
The eAG formula: eAG (mg/dL) = (28.7 × HbA1c) - 46.7 (e.g., HbA1c 7% ≈ average glucose 154 mg/dL)
-
Treatment intensification should happen promptly when HbA1c is above target - therapeutic inertia is a recognized problem in practice (PMID: 41966902, 2026 systematic review)
-
Tietz Textbook of Laboratory Medicine, 7th Ed.; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.