Viral conjunctivitis
Reading File
Finding Sources
Searching PubMed
"viral conjunctivitis" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of viral conjunctivitis, drawn from Kanski's Clinical Ophthalmology, the Wills Eye Manual, and Tintinalli's Emergency Medicine.
Viral Conjunctivitis
Etiology
Adenovirus is the most frequent cause, accounting for ~90% of cases. It is a non-enveloped, double-stranded DNA virus. Other causative agents include:
| Virus | Clinical Association |
|---|---|
| Adenovirus serovars 3, 4, 7 | Pharyngoconjunctival fever (PCF) |
| Adenovirus serovars 8, 19, 37 | Epidemic keratoconjunctivitis (EKC) |
| Adenovirus serovar 11 | Acute hemorrhagic conjunctivitis |
| Enterovirus 70, Coxsackievirus A24 | Acute hemorrhagic conjunctivitis (tropical) |
| Herpes simplex virus (HSV) | Follicular conjunctivitis (usually primary infection, unilateral) |
| Varicella-zoster virus | Conjunctivitis in ophthalmic shingles |
| Molluscum contagiosum (poxvirus) | Chronic follicular conjunctivitis via lid margin shedding |
| Rhinovirus, EBV, influenza | Sporadic cases, especially in children |
Spread occurs via contact with respiratory or ocular secretions and fomites (towels, instruments). Viral particles survive on dry surfaces for weeks, and viral shedding precedes clinical features - making containment difficult.
Clinical Variants
1. Non-specific Acute Follicular Conjunctivitis
The most common form. Unilateral onset of watering, redness, irritation, mild photophobia; the fellow eye is typically involved 1-2 days later, usually less severely. Mild systemic symptoms (sore throat, cold) may accompany it.
2. Pharyngoconjunctival Fever (PCF)
- Adenovirus serovars 3, 4, 7
- Spread by droplets in family clusters with upper respiratory tract infections
- Fever + prominent sore throat + conjunctivitis + preauricular lymphadenopathy
- Keratitis in ~30% (usually not severe)
3. Epidemic Keratoconjunctivitis (EKC)
- Adenovirus serovars 8, 19, 37; the most severe form
- Marked keratitis in ~80%; photophobia can be prominent
- Subepithelial infiltrates (SEIs) develop 1-2 weeks post-onset
- May cause significant visual morbidity; pseudomembranes can form
4. Acute Hemorrhagic Conjunctivitis
- Enterovirus 70, Coxsackievirus A24; more common in tropical regions
- Rapid onset, prominent subconjunctival hemorrhages, chemosis
- Resolves in 1-2 weeks; enterovirus 70 is rarely followed by a polio-like paralysis
5. Chronic/Relapsing Adenoviral Conjunctivitis
- Rare; chronic non-specific follicular/papillary picture persisting over years; eventually self-limiting
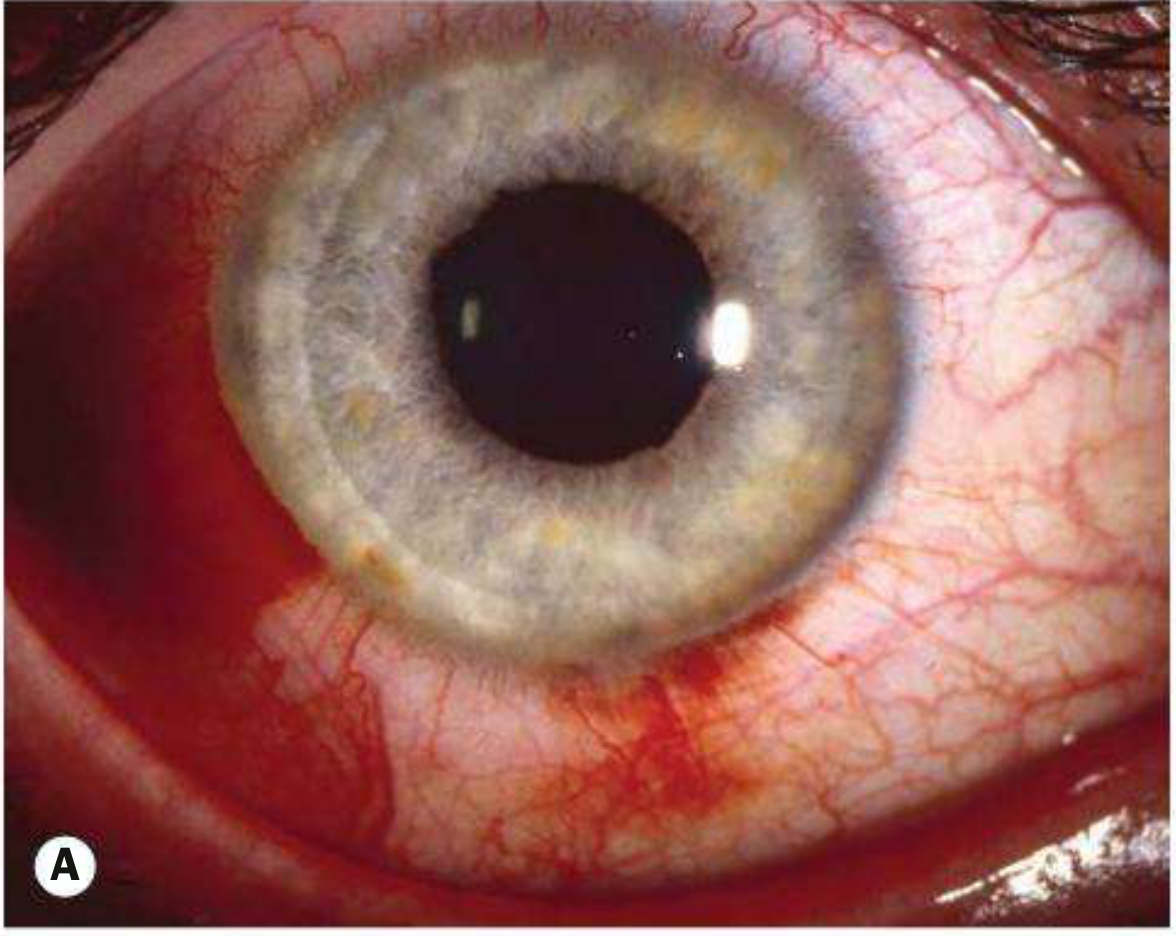
Signs & Symptoms
Symptoms: Itching, burning, tearing, foreign body/gritty sensation, photophobia; history of recent URTI or contact with infected individual; often starts unilaterally.
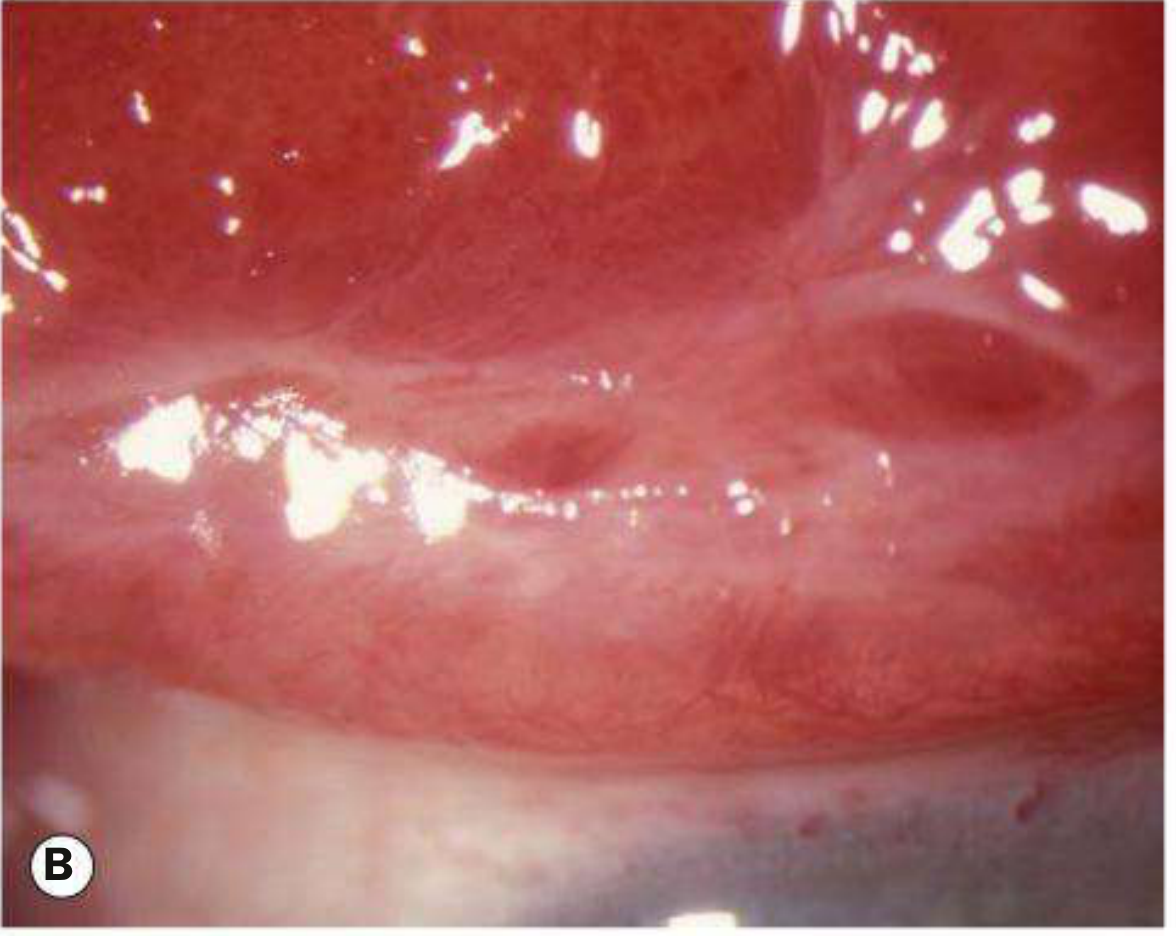
Critical signs:
- Inferior palpebral conjunctival follicles (lymphocyte aggregations around vessels)
- Tender palpable preauricular lymph node
Other signs:
- Watery (not purulent) discharge
- Red, edematous eyelids
- Petechial subconjunctival hemorrhages
- Punctate keratopathy / epithelial erosions in severe cases
- Membranes or pseudomembranes (severe inflammation)
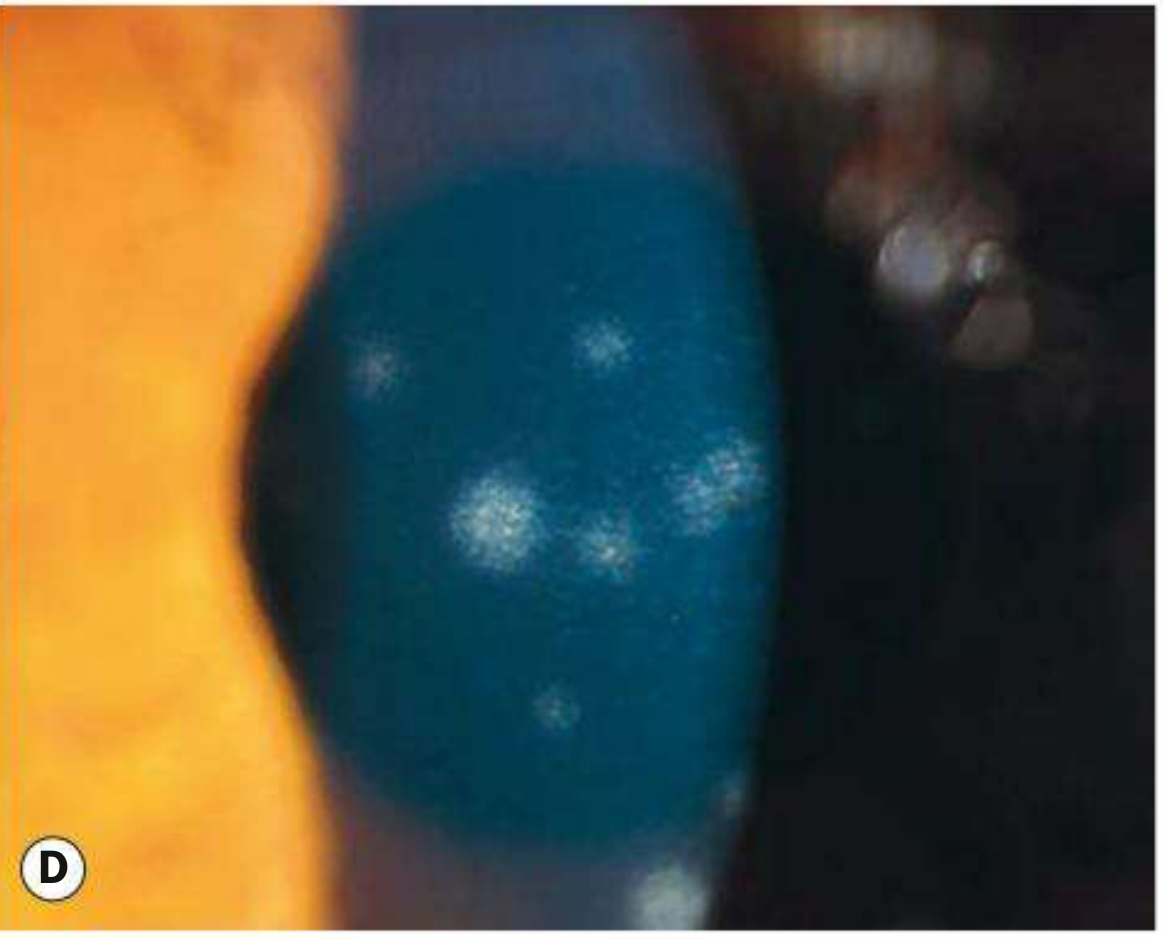
- Fine intraepithelial microcysts (early corneal sign helpful in diagnosis)
- SEIs (subepithelial infiltrates) developing 1-2 weeks after onset, possibly persisting for months to years

Investigation
Generally unnecessary. Consider if diagnosis is uncertain or resolution fails:
- PCR (NAAT) - sensitive and specific for viral DNA; preferred
- Point-of-care immunochromatography - detects adenoviral antigen in tears in 10 minutes; excellent sensitivity and specificity
- Giemsa stain - predominantly mononuclear cells in adenoviral infection; multinucleated giant cells in HSV
- Viral culture - reference standard but slow (days to weeks) and expensive
- Serology (IgM/rising IgG) - rarely used in practice
- Consider testing for chlamydia in non-resolving cases
Treatment
Supportive (all viral conjunctivitis)
- Counsel the patient: self-limited, typically worsens for first 4-7 days, may take 2-3 weeks to resolve (longer with corneal involvement)
- Preservative-free artificial tears 4-8x/day; single-use vials reduce transmission
- Cool compresses several times per day for symptomatic relief
- Topical antihistamines (e.g., epinastine 0.05% b.i.d.) if itching is severe
- Discontinue contact lens wear until full resolution
Do NOT prescribe
- Topical antibiotics are not indicated - no evidence of protection against secondary infection, and there is suspicion of harm. Use only if secondary bacterial infection is confirmed or corneal erosions are present.
For Membranes/Pseudomembranes
- Gently peel with a cotton-tip applicator or smooth forceps to improve comfort, reduce corneal defects, and prevent symblepharon
- Topical steroids: loteprednol 0.5% or prednisolone acetate 1% q.i.d. (more frequent/stronger dose)
- Consider steroid ointment (e.g., fluorometholone 0.1% ointment q.i.d.) when significant tearing would reduce drop exposure time
For SEIs Reducing Vision / Causing Photophobia
- Weaker steroid at lower frequency: loteprednol 0.2% or 0.5% b.i.d.
- Caution: Steroids may hasten symptom resolution but prolong the infectious period and necessitate long-term taper; SEIs often recur during/after taper. Do not prescribe without slit-lamp examination. Monitor IOP if prolonged use.
- NSAIDs have unclear benefit but may help during steroid weaning without promoting viral replication
Infection Control
- Contagious for 10-12 days from onset (while eyes are red/discharging)
- Meticulous hand hygiene; avoid eye rubbing, towel/pillow sharing
- Restrict work/school during active infection
- Disinfect instruments and surfaces with sodium hypochlorite or povidone-iodine
- Povidone-iodine is effective against free adenovirus and may reduce infectivity
Follow-up
- Routine: 2-3 weeks
- Sooner if worsening significantly or if topical steroids are prescribed
Key Differentiating Features from Bacterial Conjunctivitis
| Feature | Viral | Bacterial |
|---|---|---|
| Discharge | Watery | Mucopurulent |
| Follicles | Present | Absent (papillae) |
| Preauricular node | Often present | Absent (except Neisseria) |
| Bilateral involvement | Sequential (1-2 days) | Often simultaneous |
| Associated URTI | Common | Uncommon |
Sources: Kanski's Clinical Ophthalmology 10e | Wills Eye Manual | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.