Shoulder abduction
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Here is a thorough overview of shoulder abduction based on authoritative anatomy and orthopaedics textbooks.
Shoulder Abduction
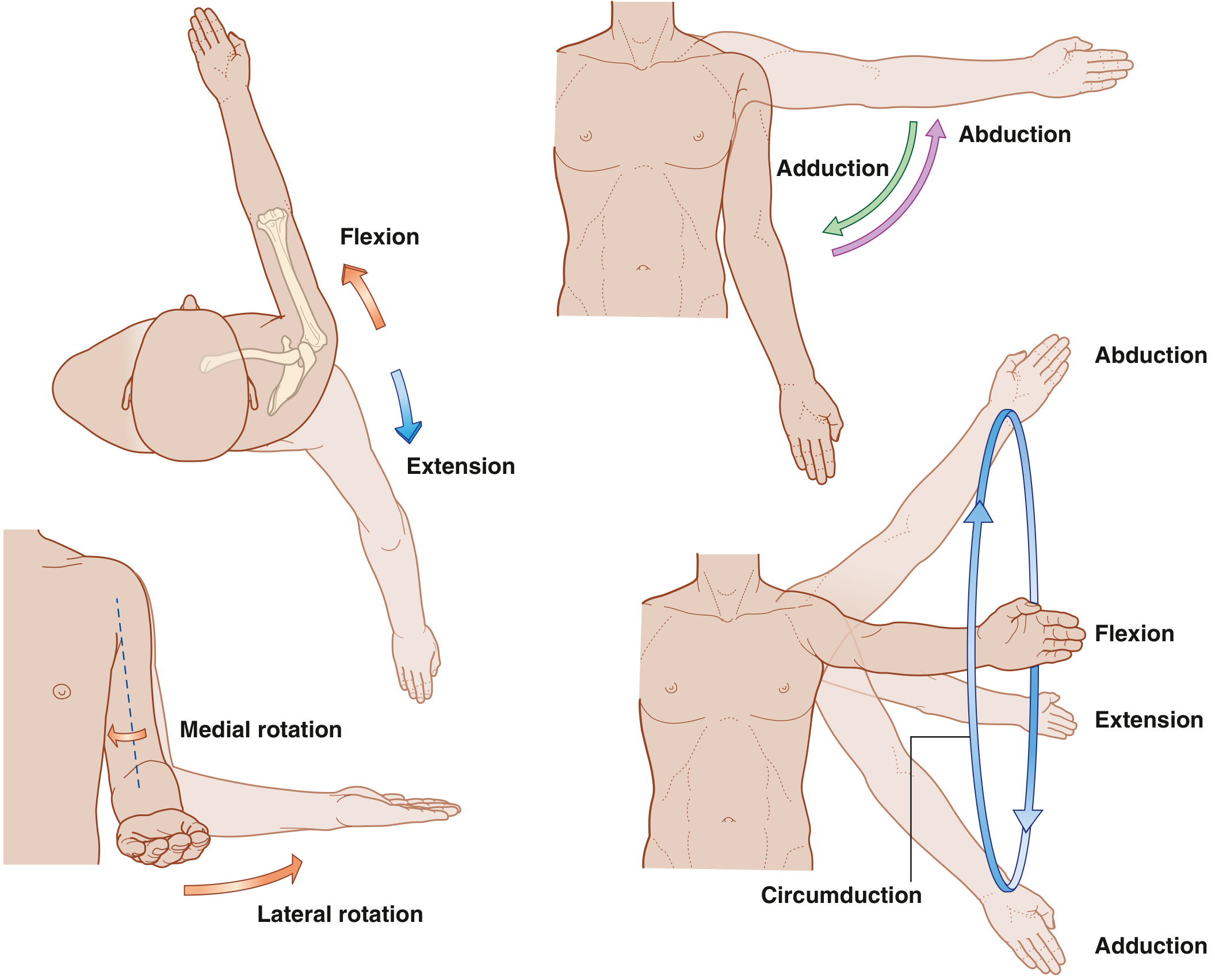
Shoulder abduction is the movement of the arm away from the body in the frontal (coronal) plane, from 0° at rest to approximately 180° at full elevation. It is one of six movements at the glenohumeral joint (along with flexion, extension, adduction, medial rotation, lateral rotation, and circumduction).
Joints Involved
Full shoulder abduction requires coordinated motion at two joints:
- Glenohumeral joint - the ball-and-socket joint where the humeral head articulates with the glenoid fossa of the scapula. It provides the primary arc of motion.
- Scapulothoracic "joint" - the functional articulation where the scapula slides and rotates on the thoracic wall. As elevation increases above 90°, the proportion of scapulothoracic motion relative to glenohumeral motion increases. This coordinated ratio is called the scapulohumeral rhythm; disturbance of it leads to impaired biomechanics and secondary impingement. - Rheumatology, 2-Volume Set (Elsevier), p. 700
The sternoclavicular and acromioclavicular joints also contribute to the full arc by allowing clavicular and scapular elevation.
Muscles and their Roles
Primary abductors
| Muscle | Role | Nerve Supply |
|---|---|---|
| Supraspinatus | Initiates abduction from 0-10° to 15° - "kicks off" the movement | Suprascapular nerve (C5, C6) |
| Deltoid (middle fibers) | Takes over from ~15° onward and drives the majority of the arc | Axillary nerve (C5, C6) |
The supraspinatus must initiate abduction because, at 0°, the deltoid has poor mechanical advantage - its line of pull is nearly vertical and would compress the humeral head into the glenoid rather than raise the arm. Once the supraspinatus moves the arm into the early range, the deltoid gets its mechanical advantage and continues. - Gray's Anatomy for Students, p. 954
A clinical point: if the supraspinatus tendon is torn, the patient cannot initiate abduction. However, by leaning and tilting the trunk (lowering and tilting the glenohumeral joint inferiorly), the deltoid can be brought into a mechanically advantageous position and abduction can still occur, though with a characteristic "trick movement." Full abduction is possible even with deltoid paralysis, driven by supraspinatus, because of this complementary relationship. - Campbell's Operative Orthopaedics, 15th Ed.
Scapular stabilizers / force couples
For the glenohumeral abductors to work effectively, the scapula must be stabilized and upwardly rotated:
- Trapezius (upper and lower fibers) - upward rotation of scapula
- Serratus anterior - forward/lateral displacement and upward rotation of scapula; responsible for forward elevation after shoulder arthrodesis - Campbell's Operative Orthopaedics
- Levator scapulae and rhomboids also contribute to scapular control
Rotator cuff (SITS muscles)
The four rotator cuff muscles (Supraspinatus, Infraspinatus, Teres minor, Subscapularis) send tendinous expansions into the joint capsule and act to compress the humeral head into the glenoid - the "concavity-compression" mechanism. This keeps the humeral head centered during abduction, preventing it from riding up under the coracoacromial arch.
Subacromial Space During Abduction
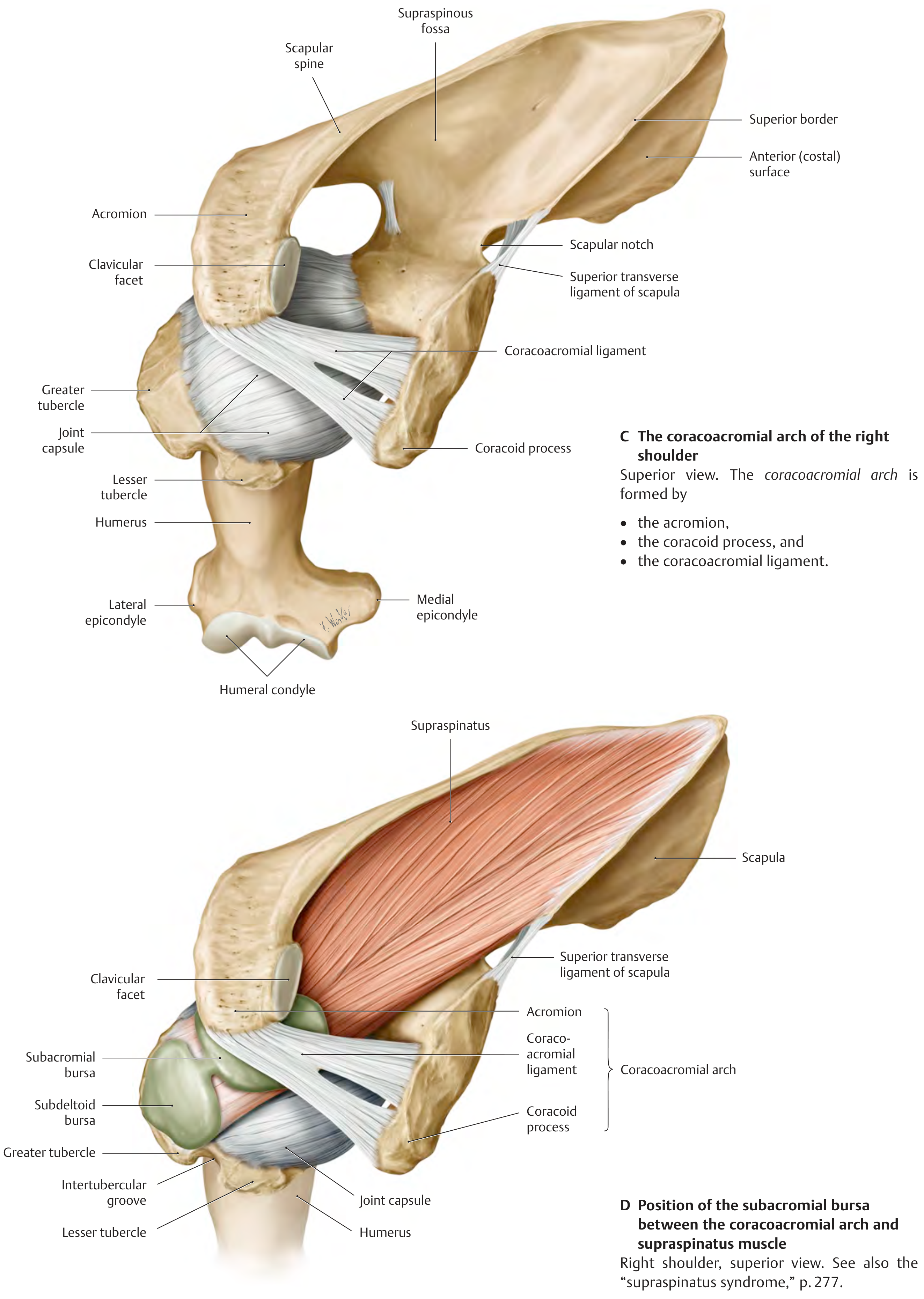
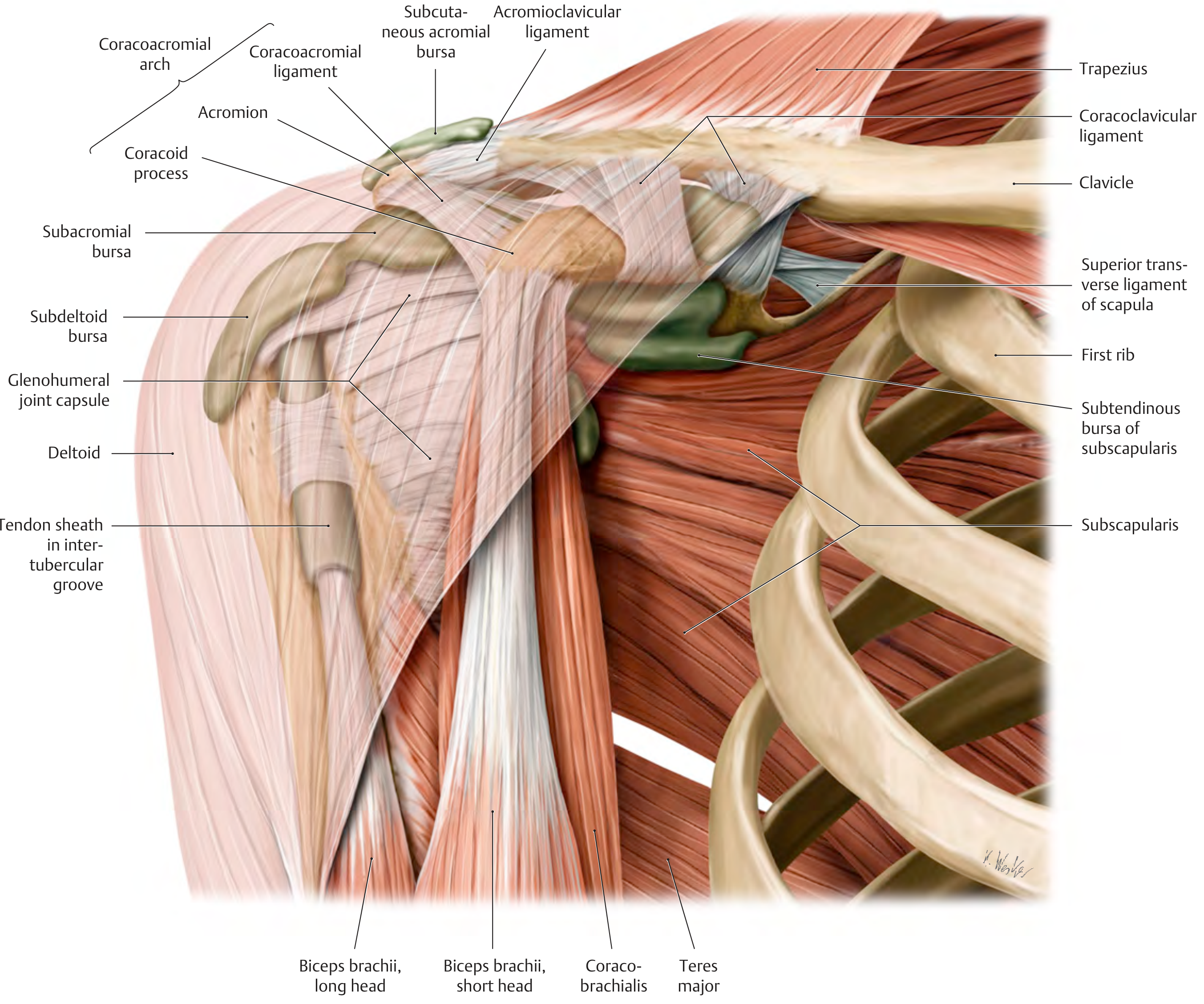
As the arm abducts, the supraspinatus tendon and the greater tubercle of the humerus pass beneath the coracoacromial arch (formed by the acromion, coracoacromial ligament, and coracoid process). The subacromial bursa (and its communicating subdeltoid bursa) sit in this space and allow frictionless gliding during movement.
If this space is reduced (due to bony spurs, rotator cuff thickening, or bursal inflammation), subacromial impingement occurs - producing a characteristic painful arc of abduction, typically between 60° and 120°.
Nerve Supply and Segmental Innervation
- Deltoid - axillary nerve (C5, C6)
- Supraspinatus - suprascapular nerve (C5, C6)
- The key nerve root for shoulder abduction is C5; an isolated C5 radiculopathy or upper brachial plexus (Erb-Duchenne) injury will impair abduction. - Textbook of Family Medicine 9e; Neuroanatomy through Clinical Cases 3rd Ed.
- Upper brachial plexus lesions (C5-C6) also paralyze biceps, brachioradialis, and brachialis, producing the classic "waiter's tip" posture.
Range of Motion
- 0-15°: supraspinatus dominant
- 15-90°: deltoid dominant, glenohumeral motion predominates
- 90-180°: increasing scapulothoracic contribution (upward rotation of scapula); the humerus also must externally rotate to clear the greater tubercle from under the acromion above 90°
Normal full abduction: 0-180° (approximately 120° at the glenohumeral joint + 60° from scapular rotation).
Clinical Testing
- Abduction against resistance tests C5 (and axillary/suprascapular nerve integrity)
- Painful arc (60-120°): subacromial impingement or rotator cuff tendinopathy
- Inability to initiate abduction: suggests supraspinatus tear
- Active > Passive restriction: rotator cuff pathology (pain on active but not passive abduction)
- Winging of the scapula during abduction: serratus anterior (long thoracic nerve) or trapezius (spinal accessory nerve) dysfunction disrupts the scapulohumeral rhythm
This is a shared conversation. Sign in to Orris to start your own chat.