Neonatal mortality indetail from spm
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive data. Let me compile the full detailed answer.
Neonatal Mortality - Park's Textbook of Preventive and Social Medicine
1. Definition
Neonatal deaths are deaths occurring during the neonatal period - commencing at birth and ending 28 completed days after birth.
Neonatal Mortality Rate (NMR) = Number of deaths of children under 28 days of age in a year / Total live births in the same year × 1000
- Park's SPM, p. 657
2. Classification
Neonatal mortality is divided into two phases:
| Period | Definition |
|---|---|
| Early neonatal | Deaths in the first 7 days of life (day 0-6) |
| Late neonatal | Deaths from day 7 to 27 |
Neonatal mortality is a measure of the intensity with which "endogenous factors" (e.g., low birth weight, birth injuries) affect infant life. It is directly related to birth weight and gestational age.
3. Causes of Neonatal Mortality
Global Distribution (Fig. 13, 2018 data):
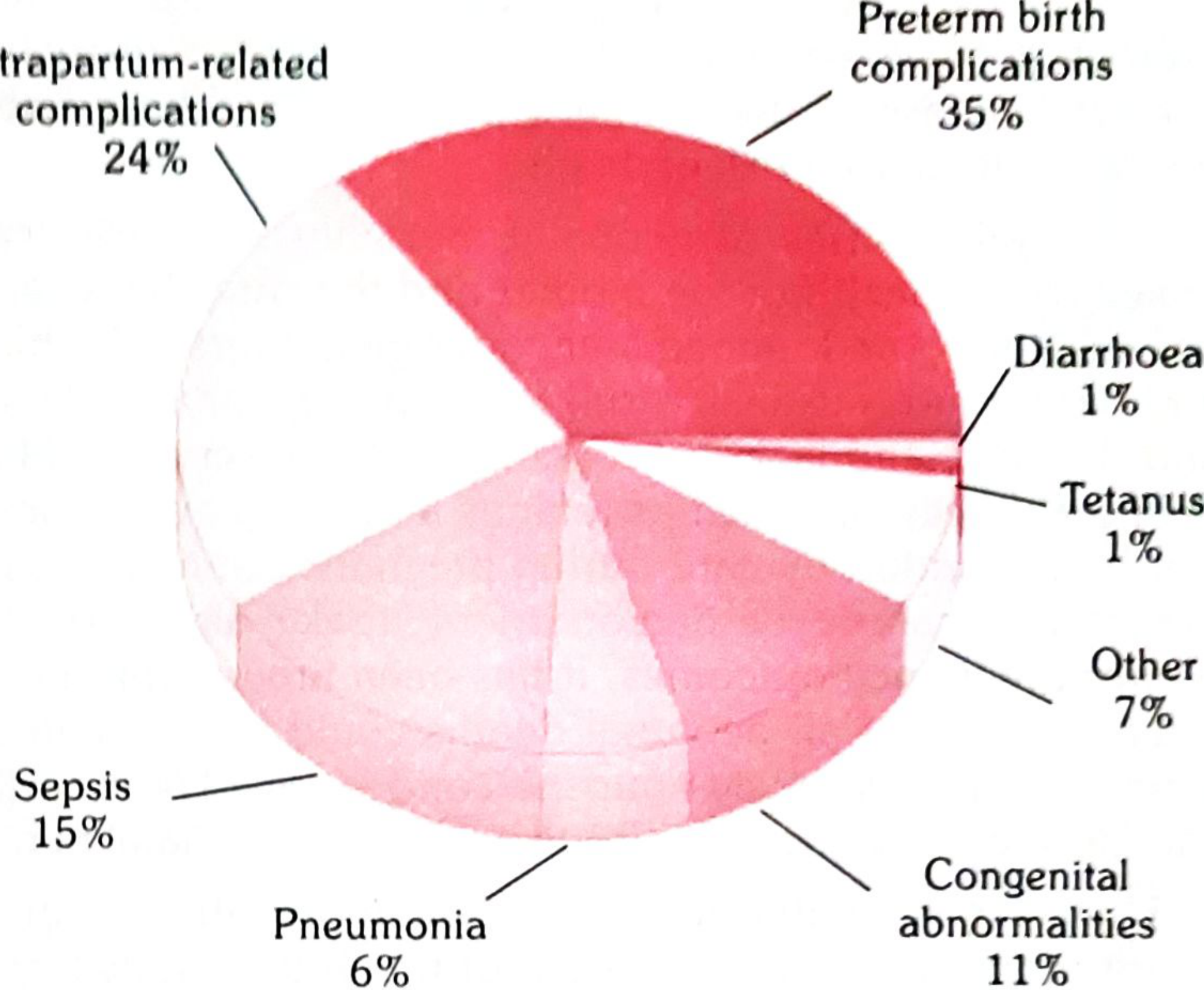
| Cause | Percentage |
|---|---|
| Preterm birth complications | 35% |
| Intrapartum-related complications (birth asphyxia) | 24% |
| Sepsis | 15% |
| Congenital abnormalities | 11% |
| Pneumonia | 6% |
| Other | 7% |
| Tetanus | 1% |
| Diarrhoea | 1% |
- Park's SPM, p. 657-658
Key Points on Causes:
- Intrapartum complications + low birth weight + preterm birth together account for 60% of neonatal deaths
- Prematurity + congenital anomalies account for about 60% of newborn deaths - mostly in the first week of life
- Asphyxia accounts for a further quarter of neonatal deaths - also mainly in the first week
- In the late neonatal period (after first week), infections (including diarrhoea and tetanus) predominate
- The contribution of tetanus to neonatal death has diminished sharply due to intensified immunization efforts
4. Determinants / Risk Factors
Biological / Endogenous:
- Low birth weight (LBW)
- Preterm birth / prematurity
- Birth injuries / asphyxia
- Congenital anomalies
Sociodemographic:
- Maternal education - NMR of babies born to mothers with no education is nearly twice as high as those born to mothers with secondary or higher education
- Family wealth - remains a powerful determinant of inequities in NMR
- Rural vs. urban residence - significant inequity
- Child marriage and adolescent pregnancy - increase the risk of newborn mortality
- Short birth intervals - increase risk
Healthcare Access:
- Lack of antenatal care (in the least developed countries, ~50% of pregnant women have no ANC)
- Delivery without a trained birth attendant (~7 out of 10 in least developed countries)
- Malnutrition and high parity of the mother
5. India-Specific Data
- India's NMR for 2018 was approximately 9 per 1000 live births (total), with both rural and urban rates also at 9 per 1000 live births
- India remains among the high infant mortality rate countries (IMR = 32 per 1000 live births in 2018)
International Comparison of IMR (1990 vs 2018):
| Country | 1990 | 2018 |
|---|---|---|
| India | 88 | 32 |
| Bangladesh | 100 | 25 |
| Pakistan | 106 | 57 |
| China | 42 | 7 |
| Nepal | 99 | 27 |
| Sri Lanka | 18 | 6 |
| UK | 8 | 4 |
| Japan | 5 | 2 |
| World | 63 | 29 |
- Park's SPM, Table 23, p. 659
6. Priority Areas to Improve Newborn Health
Before and During Pregnancy:
- Delayed child-bearing
- Well-timed, well-spaced, and wanted pregnancies
- Well-nourished and healthy mother
- Pregnancy free of drug abuse, tobacco, and alcohol
- Tetanus and rubella immunization
- Prevention of mother-to-child transmission of HIV
- Female education
During Pregnancy:
- Early contact with health systems
- Birth and emergency preparedness
- Early detection and treatment of maternal complications
- Monitoring of foetal well-being
- Prevention and treatment of anaemia
- Prevention and treatment of infections (malaria, hookworm, syphilis, STIs)
- Good diet; prevention of violence against women
During and Soon After Delivery:
- Safe and clean delivery by skilled attendant
- Early detection and prompt management of delivery complications
- Newborn resuscitation
- Newborn care ensuring warmth and cleanliness
- Newborn cord, eye and skin care
- Early initiation of exclusive breast-feeding
- Special care for preterm/LBW infants
- Prevention and control of infections
During the First Month of Life:
-
Early post-natal contact
-
Protection, promotion and support of exclusive breast feeding
-
Prompt detection and management of diseases
-
Immunization
-
Protection of girl child
-
Park's SPM, p. 658
7. Home Based Newborn Care (HBNC)
HBNC is a key national strategy aimed at improving newborn survival. Universal access to HBNC must complement the strategy of institutional delivery to achieve significant reduction in neonatal mortality and morbidity.
Providers: Anganwadi workers, ANM, ASHA (main provider)
Objectives of HBNC:
- Provision of essential newborn care and prevention of complications
- Early detection and special care of preterm and LBW newborns
- Early identification of illness and appropriate referral
- Support family for adoption of healthy practices and build confidence of the mother
ASHA's Responsibilities in HBNC:
- Mobilize all pregnant mothers for full antenatal care
- Undertake birth planning and birth preparedness
- Provide newborn care through home visits including: weighing the newborn, measuring temperature, ensuring warmth, supporting exclusive breast-feeding, promoting handwashing, providing skin/cord/eye care
- Assess high-risk babies (preterm/LBW) and increase visits for them
- Detect signs of sepsis, provide first-level care, and refer
- Recognize postpartum complications in the mother
- Counsel couples for family planning
- Provide immediate newborn care for home deliveries
ASHA Visit Schedule:
Visits to all newborns up to 42 days of life as per a specified schedule.
8. SDG Target
By 2030 (SDG 3.2): End preventable deaths of newborns and children under 5, with all countries aiming to reduce NMR to at least 12 per 1000 live births and under-5 mortality to at least 25 per 1000 live births.
- Park's SPM, Table 4
9. Factors Explaining Decline in Infant Mortality
- Improved obstetric and perinatal care (oxygen availability, foetal monitoring, better labour management)
- Improvement in quality of life (economic and social progress)
- Better control of communicable diseases (immunization, ORS)
- Advances in chemotherapy, antibiotics, and insecticides
- Better nutrition (emphasis on breast feeding)
- Family planning (birth spacing)
Key note: In developed countries, the dominant factor was economic and social progress; in developing countries, medical services made the major impact. Further reduction in neonatal mortality in developing countries depends on socio-economic development.
All content sourced from Park's Textbook of Preventive and Social Medicine, Chapter on Demography and Vital Statistics, pp. 657-659.
Infant mortality rate indetail from spm and explain indetail abt causes in flow chart and make a graph for infant mortality raye
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Running Command
Reading File
Reading File
Infant Mortality Rate (IMR) - Park's SPM - Complete Notes
1. Definition
IMR = "The ratio of infant deaths registered in a given year to the total number of live births registered in the same year; usually expressed as a rate per 1000 live births." (Park's SPM, p. 658)
Formula:
IMR = (Deaths of children < 1 year in a year ÷ Live births in same year) × 1000
2. Importance of IMR
IMR is universally regarded as:
- The most important indicator of health status of a community
- A measure of the level of living of people in general
- A measure of the effectiveness of MCH (Mother & Child Health) services in particular
Why infant mortality is treated separately by demographers:
- Infant mortality is the largest single age-category of mortality
- Deaths at this age are due to a peculiar set of diseases and conditions to which adults are less exposed or vulnerable
- Infant mortality is affected quickly and directly by specific health programmes and can change more rapidly than the general death rate
3. Components of IMR
| Component | Period | Causes |
|---|---|---|
| Neonatal mortality | 0-28 days | Endogenous - prematurity, LBW, birth asphyxia, congenital anomalies |
| Post-neonatal mortality | 29 days - 1 year | Exogenous - infections (diarrhoea, pneumonia), malnutrition |
- In developing countries: high IMR is mainly due to low birth weight + infections (diarrhoea, respiratory infections) + malnutrition
- In developed countries: mainly due to congenital anomalies, anoxia and hypoxia
4. Causes Flowchart
Flowchart Download:
flowchart
Image · PNG
5. Factors Affecting Infant Mortality (Detailed)
A. BIOLOGICAL FACTORS
(a) Birth Weight
- Major determinant of infant and perinatal mortality
- Babies of LBW (<2.5 kg) and high birth weight (>4 kg) are at special risk
- Virtually all infants <1000g at birth succumb
- Key cause: poor maternal nutrition - not just during pregnancy but even before
- A mother well-nourished during her own growing-up years has an excellent chance of delivering a normal-sized baby
(b) Age of the Mother
- IMR is greatest when mother is:
- Very young (below 19 years) - teen mothers
- Relatively older (over 30 years)
- Very young mothers tend to be poorer and less educated
(c) Birth Order
- Highest mortality: first born
- Lowest mortality: second born
- Risk escalates after the third birth
- The 5th and later children always have worse outcomes than the 3rd child
- IMR from nutritional deficiencies is 3-4 times higher for 5th+ birth order vs. first three
(d) Birth Spacing
- Repeated pregnancies cause malnutrition and anaemia in the mother → LBW → higher infant death
- The premature weaning of a displaced youngest baby leads to:
- (a) Protein Energy Malnutrition (PEM)
- (b) Diarrhoea and dehydration
- Khanna Study (India): IMR was highest for interval of 1 year, lower for 2-3 years, lowest for 4 years
- World Fertility Survey: Babies born within 1 year of each other have 2-4 times higher risk than those born >2 years apart
- Wider birth spacing is considered as important as immunization
(e) Multiple Births
- Higher risk due to greater frequency of LBW among twins/multiples
(f) Family Size
- IMR increases with family size
- Larger families = more infectious diarrhoea, malnutrition, respiratory infections
- Duration of illness is longer in families with 3 or more children
- Deprivation of maternal care is also found in large families
(g) High Fertility
- High fertility and high infant mortality go together - one of the most important factors
B. ECONOMIC FACTORS
- Socio-economic status is the single most important variable affecting IMR (both directly and indirectly)
- Quality of healthcare and child environment are closely related to socio-economic status
- IMR is highest in slums and lowest in richer residential localities
- Major improvements in health status and fall in IMR require continuing socio-economic development including provision of health services
C. CULTURAL AND SOCIAL FACTORS
(a) Breast-feeding
- Breast milk contains nutritional content and natural immunizing agents
- Early weaning and bottle-fed infants under poor hygienic conditions are more prone to die than breast-fed infants under similar conditions
(b) Religion and Caste
- Differences attributed to socio-cultural patterns - habits, customs, traditions affecting cleanliness, eating, clothing, and child care
(c) Early Marriages
- Baby of a teenage mother has the highest risk for both neonatal and post-neonatal mortality
(d) Sex of the Child
- In most parts of India, female infants receive far less attention than males
- Female infant mortality is higher than male infant mortality overall
- But when split: neonatal death rate is higher for males; post-neonatal death rate is higher for females
- Birth of a female child is unwelcome in many families → lack of nutrition and medical care
(e) Quality of Mothering
- Even in extreme poverty, children survive if they have an efficient mother
- "Quality of mothering" helps reduce IMR
(f) Maternal Education
- Illiteracy is the greatest barrier to health improvement
- Mother's education is a key determinant of children's health (Kerala experience)
- Educated women: marry later, delay childbearing, practice family planning, have fewer children with wider spacing
(g) Quality of Health Care
- Inadequate prenatal care and infrequent attendance at delivery
- High percentage of deliveries attended by untrained persons in rural India
- Only 47% of deliveries are attended by trained birth attendants in India
(h) Broken Families
- Infant mortality tends to be high where the mother or father has died or separated
(i) Illegitimacy
- A child born out of wedlock is generally unwanted → does not receive adequate nutrition or medical care
(j) Brutal Habits and Customs
- Depriving the baby of colostrum (first milk)
- Frequent purgation
- Branding the skin
- Application of cowdung to the umbilical cord stump
- Faulty feeding practices and early weaning
(k) The Indigenous Dai (Untrained Midwife)
- Greatly responsible for high IMR in India
- Usually illiterate, devoid of knowledge of hygiene
- Unhygienic delivery practice is an important cause of high IMR
(l) Bad Environmental Sanitation
- Lack of safe water supply, poor housing, bad drainage, overcrowding, insect breeding
- All increase the risk of infant mortality
6. International Comparison Graph
Graph Download:
imr graph
Image · PNG
| Country | 1990 | 2018 | % Reduction |
|---|---|---|---|
| India | 88 | 32 | 64% |
| Bangladesh | 100 | 25 | 75% |
| Nepal | 99 | 27 | 73% |
| Myanmar | 78 | 37 | 53% |
| Pakistan | 106 | 57 | 46% (least reduced) |
| China | 42 | 7 | 83% |
| Thailand | 30 | 8 | 73% |
| Sri Lanka | 18 | 6 | 67% |
| Japan | 5 | 2 | 60% (best globally) |
| UK | 8 | 4 | 50% |
| USA | 9 | 6 | 33% |
| World Average | 63 | 29 | 54% |
- World average IMR (2018) = 29 per 1000 live births
- Developed countries: 4 per 1000
- Least developed countries: 46 per 1000
- South Asian average: 35 per 1000
7. Factors Responsible for Decline in IMR
(a) Improved obstetric and perinatal care - oxygen availability, foetal monitoring, better labour induction techniques
(b) Improvement in quality of life - economic and social progress
(c) Better control of communicable diseases - immunization and ORS
(d) Advances in chemotherapy, antibiotics, and insecticides
(e) Better nutrition - emphasis on breast-feeding
(f) Family planning - birth spacing
Key point: In industrialized countries, dominant factor = economic and social progress. In developing countries, dominant factor = medical services (mass disease control, immunization, antibiotics). Therefore IMR is reluctant to fall below 100 in many developing countries without socio-economic development.
8. Preventive and Social Measures to Reduce IMR
Since IMR is multifactorial, a multipronged approach is essential:
| # | Measure | Key Points |
|---|---|---|
| 1 | Prenatal Nutrition | Extra 500 kcal + 10g protein in last 4 weeks → +300g birth weight (Indian study); ICDS programme |
| 2 | Prevention of Infection | Immunization; Universal Immunization Programme (1985) for 9 vaccine-preventable diseases |
| 3 | Promotion of Breast-feeding | Most effective measure; safeguard against GI + respiratory infections and PEM |
| 4 | Growth Monitoring | Monthly weighing; growth charts to identify at-risk children early |
| 5 | Family Planning | Birth spacing + limiting family size; risk greatly enhanced if last child born <2 yrs ago |
| 6 | Sanitation | Safe water, hygienic housing, vector control |
| 7 | Primary Health Care | High-risk antenatal detection; special care baby units for <2000g; referral services |
| 8 | Socio-economic Development | Ultimate solution - female education, nutrition standards, safe water, housing, agriculture, commerce |
| 9 | Education | Tamil Nadu study: mid-day meals + women's healthcare → IMR fell from 90 (1984) to 57 (1991) |
All content from Park's Textbook of Preventive and Social Medicine, pp. 658-663
Infant mortality rate indetail causes explain in flow chart
Running Command
Reading File
Running Command
Reading File
The flowchart is clean, complete and fully readable. Here is your full answer:
IMR Causes — Detailed Flowchart
Download the flowchart here:
imr causes flowchart final
Image · PNG
How to Read the Flowchart
The chart flows top → bottom in 5 levels:
IMR (Definition & Formula)
↓
Multifactorial Aetiology
↙ ↓ ↘
[A] [B] [C]
Biological Economic Cultural & Social
Factors Factors Factors
↓ (all converge)
Proximate Causes
(Infections · Malnutrition · LBW · Poor Health Care)
↓
INFANT DEATH
↓
Preventive Measures (9 key interventions)
Summary of All Causes (from Park's SPM)
A. Biological Factors (7 sub-factors)
| Factor | Key Detail |
|---|---|
| Low Birth Weight (<2.5 kg) | Major determinant; <1000g = near 100% death |
| Age of Mother | <19 yrs or >30 yrs = highest risk |
| Birth Order | 1st born = highest; escalates after 3rd birth |
| Birth Spacing <2 yrs | 2-4x higher risk (Khanna Study) |
| Multiple Births | Higher LBW → higher death |
| Family Size | More children = more infections, less maternal care |
| High Fertility | Always co-exists with high IMR |
B. Economic Factors (5 sub-factors)
| Factor | Key Detail |
|---|---|
| Socio-economic Status | Single most important variable |
| Slum vs. Affluent | IMR highest in slums |
| Access to Health Care | Tied to income level |
| Poverty → Malnutrition | Low income → LBW → death |
| Unemployment | Limits nutrition, housing, medicines |
C. Cultural & Social Factors (10 sub-factors)
| Factor | Key Detail |
|---|---|
| Breast-feeding failure | Early weaning → GI/respiratory infections + PEM |
| Early marriage | Teenage mother = highest neonatal risk |
| Sex of child (India) | Female infants neglected |
| Maternal education | Illiteracy = greatest barrier; Kerala model |
| Quality of mothering | Efficient mother reduces IMR even in poverty |
| Untrained birth attendants | Only 47% trained in India |
| Broken families/illegitimacy | Neglect → increased IMR |
| Brutal customs | Discarding colostrum, cow-dung on cord |
| Bad environmental sanitation | Unsafe water, overcrowding, poor housing |
| Religion & caste | Socio-cultural practices affecting child care |
Source: Park's Textbook of Preventive and Social Medicine, pp. 658-663
This is a shared conversation. Sign in to Orris to start your own chat.