Loose stools with undigested/ semidigested food in stool
Reading File
Finding Sources
Finding Sources
Searching the Web
loose stools undigested food causes malabsorption differential diagnosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to give a thorough answer. Let me compile it.
Loose Stools with Undigested/Semi-digested Food
Passage of undigested or semi-digested food in loose stools points to a problem somewhere along the continuum of digestion, absorption, or transit. The clinical term for fat in the stool is steatorrhea; when protein and carbohydrate are also affected, it reflects broader malabsorption. Clinically this presentation is classified under fatty/malabsorptive diarrhea.
Pathophysiological Framework
There are four broad mechanisms (Goldman-Cecil Medicine, Table 126-4):
| Mechanism | Key Examples |
|---|---|
| Impaired mixing | Post-gastrectomy, gastric bypass surgery |
| Impaired lipolysis (maldigestion) | Chronic pancreatitis, pancreatic cancer, gastrinoma, congenital lipase deficiency |
| Impaired micelle formation | Severe liver disease, bile acid deficiency, SIBO, ileal resection/Crohn's |
| Impaired mucosal absorption | Celiac disease, tropical sprue, Giardiasis, Whipple's disease, radiation enteritis, lymphoma, Crohn's, SIBO, short bowel syndrome |
| Impaired nutrient delivery | Intestinal lymphangiectasia, lymphoma, TB, constrictive pericarditis |
Causes - Differential Diagnosis
1. Pancreatic Exocrine Insufficiency (PEI)
- Seen in chronic pancreatitis, pancreatic cancer, cystic fibrosis
- Steatorrhea appears only when lipase output falls below 10% of normal (Schwartz's Surgery)
- Stools are large, bulky, fat-laden (>30 g fat/day), foul-smelling, oily, difficult to flush
- Often associated with abdominal pain and diabetes
2. Celiac Disease (Gluten-Sensitive Enteropathy)
- Autoimmune villous atrophy of the proximal small intestine
- Diarrhea with steatorrhea + weight loss + bloating; extraintestinal: dermatitis herpetiformis, iron/folate deficiency anemia, osteomalacia
- Diagnosis: anti-tissue transglutaminase IgA (anti-TTG IgA) + duodenal biopsy
3. Small Intestinal Bacterial Overgrowth (SIBO)
- Excess bacteria in small bowel deconjugate bile salts - impaired micelle formation
- Causes steatorrhea + B12 deficiency + bloating; often in setting of structural abnormalities, dysmotility, or post-surgical anatomy
- Diagnosed by glucose/lactulose H2 breath test or small bowel aspirate culture
4. Inflammatory Bowel Disease (Crohn's Disease)
- Transmural inflammation, particularly ileitis, reduces absorptive surface
- Undigested food, diarrhea, abdominal pain, weight loss, possible blood
- May present with perianal disease, fever, extraintestinal manifestations (arthritis, uveitis, erythema nodosum)
5. Giardiasis
- Most common protozoan cause of malabsorption worldwide
- Loose, greasy, foul-smelling stools; bloating, flatulence, abdominal cramps; NO blood in stool
- Exposure history: travel, contaminated water, children
- Diagnosis: stool PCR or antigen ELISA; empirical metronidazole trial is reasonable
6. Rapid Intestinal Transit / Dysmotility
- Hyperthyroidism, carcinoid syndrome, diabetic autonomic neuropathy, VIPoma
- Reduced contact time = incomplete digestion and absorption
- Even with rapid transit alone, mild steatorrhea up to 14 g fat/day can occur (Harrison's)
7. Bile Acid Malabsorption (BAD)
- Ileal disease/resection (<100 cm) leads to bile acid loss into colon, causing secretory + osmotic diarrhea
- Watery diarrhea with urgency; may have some fat malabsorption
8. Whipple's Disease
- Tropheryma whipplei infection; rare but classic
- Steatorrhea + arthralgia + lymphadenopathy + weight loss + CNS changes
- Duodenal biopsy: PAS-positive macrophages in lamina propria
9. Tropical Sprue
- Acquired enteropathy in endemic regions (tropics)
- Pale, bulky, frothy, foul-smelling stools; glossitis, weight loss, B12/folate deficiency (Sleisenger & Fordtran)
10. Short Bowel Syndrome
- Post-surgical reduction of absorptive surface
- Diarrhea worsens with eating (unlike secretory diarrhea which persists with fasting)
11. Lactase / Disaccharidase Deficiency
- Unabsorbed sugars cause osmotic diarrhea + fermentation gas
- Watery diarrhea, bloating after dairy/sugars - typically NOT steatorrhea
- H2 breath test after lactose challenge
Key Features on History
Harrison's emphasizes asking specifically about (Harrison's 22E):
- Relationship of diarrhea to food ingestion (worsening with eating suggests malabsorption/short bowel; secretory diarrhea persists with fasting)
- Presence of nocturnal episodes (organic > functional)
- Undigested food or fat in stool
- Consistency (Bristol Stool Scale)
- Weight loss (points to organic malabsorption)
- Floating/oily/foul-smelling stools (classic steatorrhea)
- Travel history, medication history, family history of celiac/IBD
Diagnostic Approach
Initial Workup
- CBC - anemia (iron, B12, folate deficiency)
- CRP/ESR - inflammation
- Anti-TTG IgA + total IgA - celiac screen
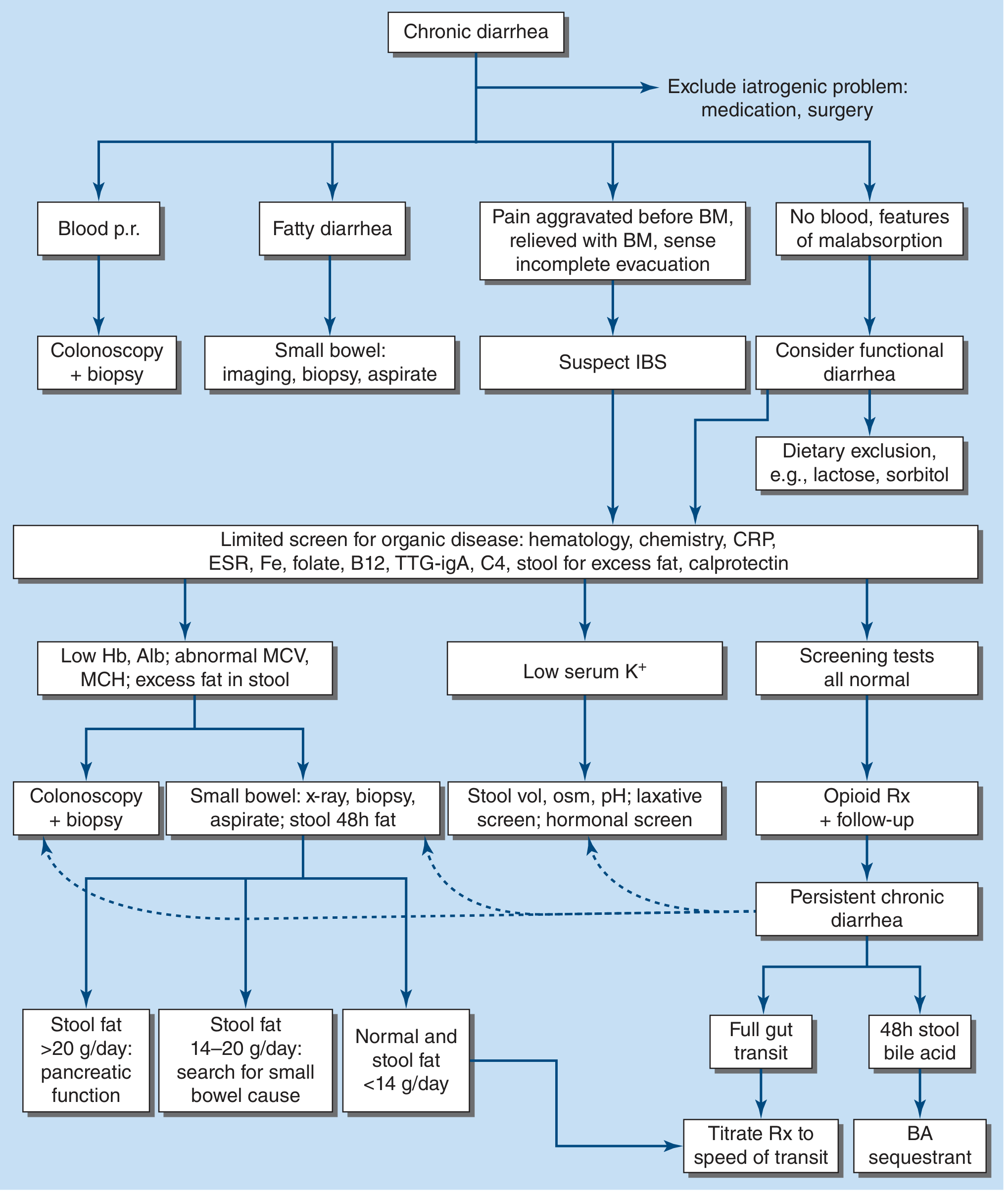
- Stool fat test (72h fecal fat on 70-100 g/day fat diet) - best screening test for malabsorption
- Stool fat >20 g/day → evaluate pancreatic function (stool elastase, imaging)
- Stool fat 14-20 g/day → evaluate small bowel (biopsy, imaging, SIBO breath test)
- Stool fat <14 g/day → rapid transit or functional cause more likely
- Stool PCR/ELISA for Giardia + ova and parasites
- Serum albumin, electrolytes, LFTs, TSH
- Stool calprotectin - screens for intestinal inflammation
Second-line Investigations
- CT/MR enterography - mucosal disease, structural abnormalities, lymphoma
- Upper endoscopy with duodenal biopsy - celiac, Whipple's, Giardia trophozoites
- Colonoscopy to terminal ileum - IBD, microscopic colitis, villous adenoma
- H2 breath test - SIBO, lactase deficiency
- Serum 7αC4 or fecal bile acids - bile acid diarrhea
- Stool elastase-1 - pancreatic exocrine insufficiency (sensitivity ~85-90% for severe PEI)
- Hormonal screen (VIP, gastrin, serotonin, calcitonin) if secretory neuroendocrine tumor suspected
Red Flags Requiring Urgent Investigation
- Weight loss >5 kg
- Nocturnal diarrhea
- Rectal bleeding
- Age >50 at onset
- Family history of colorectal cancer or IBD
- Anemia, hypoalbuminemia, edema
- Abdominal mass
Summary Table
| Cause | Stool Character | Key Clues |
|---|---|---|
| Pancreatic insufficiency | Bulky, oily, >30 g fat/day | Abdominal pain, diabetes, alcohol history |
| Celiac disease | Pale, loose, floating | Dermatitis herpetiformis, anemia, gluten exposure |
| SIBO | Variable steatorrhea | Bloating, B12 low, structural bowel disease |
| Crohn's disease | Loose ± blood | Pain, fever, perianal disease, weight loss |
| Giardiasis | Greasy, foul-smelling | Travel, no blood, flatulence |
| Bile acid malabsorption | Watery, urgent | Ileal disease/resection history |
| Rapid transit | Loose, poorly digested | Thyroid disease, carcinoid, diabetic neuropathy |
| Whipple's disease | Steatorrhea | Arthralgia, weight loss, CNS changes |
| Lactase deficiency | Watery, gassy | Bloating after dairy, no fat in stool |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine; Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.