Pheochromocytoma and anaesthesia management
Reading File
Finding Sources
Finding Sources
Searching PubMed
pheochromocytoma anesthesia perioperative management
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching the Web
pheochromocytoma anaesthesia management 2024 2025 guidelines alpha blockade
I now have a complete and authoritative picture from multiple textbooks plus current evidence. Let me compile the comprehensive response.
Pheochromocytoma and Anaesthesia Management
1. Overview and Relevance to Anaesthesia
Pheochromocytomas (and their extra-adrenal counterparts, paragangliomas) are catecholamine-secreting tumors of chromaffin tissue. Historically they carried a perioperative mortality of 25-50%; with modern preoperative preparation and anaesthetic technique, this has fallen below 1-3%. The anaesthesiologist must manage three sequential threats:
- Pre-vein ligation - paroxysmal catecholamine surges causing severe hypertension, tachycardia, and arrhythmias
- Post-vein ligation - sudden catecholamine withdrawal causing profound hypotension
- Postoperative - hypoglycaemia, delayed hypotension, residual hypertension
The "10% rule": ~10% are malignant, 10% bilateral, 10% extra-adrenal, 10% familial (MEN 2a/2b, von Hippel-Lindau, NF-1). It is now recognised that all pheochromocytomas carry some malignant potential.
2. Preoperative Assessment
Symptoms to evaluate
- Classic triad: paroxysmal hypertension, headache, sweating (plus palpitations)
- Spells triggered by positional change, anxiety, medications (especially opioids, metoclopramide)
- Catecholamine-induced cardiomyopathy (may be severe and reversible)
- Chronic hypovolaemia (vasoconstricted vascular bed, contracted plasma volume)
Investigations
- 24-hour urinary fractionated metanephrines/catecholamines (>98% sensitivity/specificity for low-suspicion patients)
- Plasma fractionated metanephrines (sensitivity 96-100%, preferred in high-suspicion or familial cases)
- ECG - ST-T changes, arrhythmias
- Echocardiogram if cardiomyopathy suspected (longstanding, high catecholamine burden)
- Localisation: MRI/CT; MIBG scan
Roizen Criteria for preoperative readiness (1980s, still referenced)
- BP < 165/90 mmHg
- Orthostatic hypotension present (SBP still > 80/45 mmHg)
- No new ST-T changes on ECG
- < 1 PVC per 5 minutes
The 2014 Endocrine Society guidelines set tighter targets: sitting BP < 130/80 mmHg (standing SBP > 90 mmHg); resting HR 60-70 bpm (standing 70-80 bpm).
3. Preoperative Medical Preparation
This is the most critical element. Duration: typically 7-14 days minimum before surgery (up to 2-4 weeks for severe disease or significant cardiac/renal comorbidity). Preparation starts at least 1-2 weeks preoperatively as outpatient, then 1-2 days inpatient for IV volume restoration.
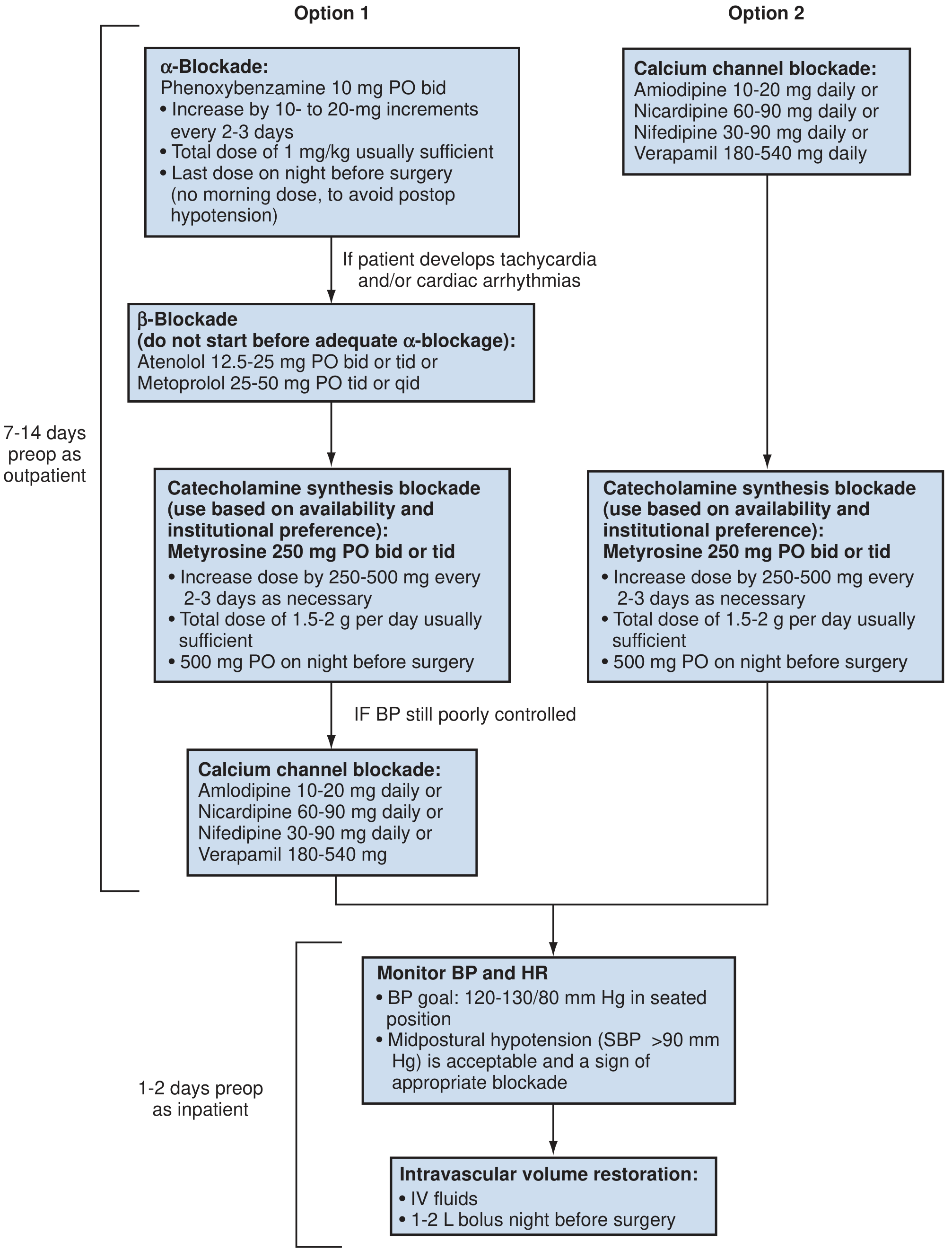
Fig. 106.20 - Campbell Walsh Wein Urology: Preoperative medical management pathways with alpha-blockade (Option 1) and calcium channel blockade (Option 2)
Alpha-blockers (first-line)
| Drug | Type | Dose | Notes |
|---|---|---|---|
| Phenoxybenzamine | Non-selective, irreversible | 10 mg BD, titrate up by 10-20 mg every 2-3 days; total ~1 mg/kg | Gold standard; causes significant orthostasis; omit morning dose on day of surgery to avoid postop hypotension |
| Doxazosin | Selective α₁ | 2-16 mg/day | Gradual shift toward this; fewer side effects; but 2025 data show prolonged use (>30 days) associated with more hypertensive crises intraoperatively |
| Prazosin | Selective α₁ | 2-5 mg 2-3 times daily | Alternative |
Key rule: Alpha blockade MUST precede beta blockade. Starting a beta-blocker first causes unopposed alpha stimulation (no vasodilation, only reduced cardiac output) - this precipitates a hypertensive crisis.
Beta-blockers (second-line, only after alpha is established)
- Added only if persistent tachycardia or arrhythmias develop after alpha blockade
- Atenolol 12.5-25 mg BD/TDS or Metoprolol 25-50 mg TDS/QDS
- Propranolol (traditional) - can cause profound bradycardia, myocardial depression; use cautiously
Calcium Channel Blockers (alternative to or adjunct with alpha blockade)
- Option 2 in the algorithm above (especially if patient cannot tolerate orthostasis from alpha blockers)
- Nicardipine, amlodipine (10-20 mg/day), nifedipine, verapamil
- Amlodipine shown to be an efficacious alternative to alpha blockade for preventing intraoperative haemodynamic instability
Metyrosine (catecholamine synthesis inhibitor)
- Tyrosine hydroxylase inhibitor; reduces catecholamine production 50-80%
- Dose: 250 mg BD/TDS, titrate by 250-500 mg every 2-3 days; 500 mg the night before surgery
- Reserved for refractory cases (severe hypertension not controlled by blockade), metastatic disease, or perioperative catecholamine storms
- Causes profound sedation; not routinely stocked
Volume Restoration
- High sodium diet (3-5 g/day) + liberal fluid intake during alpha blockade reverses catecholamine-induced volume contraction
- 1-2 L IV fluid bolus the night before surgery (inpatient)
- A falling haematocrit during alpha blockade confirms appropriate volume expansion
4. Intraoperative Management
Monitoring
- Arterial line (mandatory) - placed before induction for beat-to-beat BP monitoring
- Large-bore IV access (x2 minimum)
- Central venous access - when postoperative vasoactive infusions anticipated (not routine)
- Transesophageal echocardiography (TOE) or pulmonary artery catheter - in patients with ventricular dysfunction or significant cardiac disease
- Urinary catheter, temperature, glucose monitoring
Premedication
- Benzodiazepines or dexmedetomidine for anxiolysis - reduces catecholamine surges on arrival/transfer
Induction
- Slow, controlled induction; intubation only after deep anaesthetic level achieved
- Propofol or etomidate - both safe
- Ketamine - AVOID (stimulates sympathetic nervous system, triggers catecholamine release)
- Adequate depth before laryngoscopy; consider topical lidocaine to the airway to blunt the intubation response
Maintenance
- All inhalational agents acceptable except desflurane (can cause transient tachycardia) - best avoided
- Halothane - AVOID (sensitises myocardium to catecholamine-induced arrhythmias)
- Isoflurane, sevoflurane commonly used
- Neuromuscular blockers: Most acceptable; pancuronium - AVOID (vagolytic, causes tachycardia and can cause hypertension)
- Opioids: Most are safe; avoid large doses of morphine (histamine release) and atracurium at large bolus doses (histamine release)
- Epidural analgesia: Can supplement for postoperative pain control, but does not reliably attenuate intraoperative hypertensive crises and risks postoperative hypotension
Drugs to AVOID Summary
| Drug | Reason |
|---|---|
| Ketamine | Sympathomimetic; triggers catecholamine release |
| Desflurane | Transient sympathetic activation, tachycardia |
| Halothane | Sensitises myocardium to arrhythmias |
| Pancuronium | Vagolytic; promotes tachycardia and hypertension |
| Morphine (large bolus) / atracurium (large bolus) | Histamine release |
| Ephedrine | Indirectly releases catecholamines |
| Droperidol, metoclopramide | Can precipitate catecholamine crisis |
5. Intraoperative Haemodynamic Crises
Pre-vein ligation: Hypertensive crises
Triggered by induction, intubation, positioning, and especially direct tumour manipulation.
Preferred drugs (short-acting, titratable):
| Drug | Mechanism | Notes |
|---|---|---|
| Clevidipine | Calcium channel blocker (CCB), ultra-short-acting | First-line IV agent; highly titratable |
| Nicardipine | CCB | Widely used; effective |
| Sodium nitroprusside | Direct vasodilator | Rapid onset/offset; cyanide toxicity risk with prolonged use |
| Nitroglycerine | Vasodilator | Less potent than nitroprusside |
| Phentolamine | Non-selective alpha blocker | Historically used; prolonged onset/duration makes it less preferred now |
| Esmolol | Beta-1 blocker | For intraoperative tachycardia/arrhythmia control |
| Magnesium sulphate | Direct vasodilator; membrane stabiliser; inhibits catecholamine release from tumour | Loading dose 2-4 g IV before induction, then 1-2 g/h infusion during resection - widely used, very effective |
| Lidocaine | Antiarrhythmic | For ventricular arrhythmias |
Magnesium deserves special mention - it is now commonly used as it both vasodilates and directly reduces catecholamine release from the tumour.
Post-vein ligation: Hypotension
Once the venous drainage is ligated, catecholamines drop abruptly. The combination of:
- Residual alpha blockade
- Hypovolaemia
- Loss of catecholamine-mediated vascular tone ...produces profound hypotension.
Management:
- Aggressive IV fluid loading begins before vein ligation (anticipate the drop)
- Phenylephrine - first-line vasopressor (alpha-1 agonist, easy to use)
- Norepinephrine or epinephrine infusions if phenylephrine insufficient
- Choice of vasopressor can be guided by the tumour's dominant catecholamine secretion (e.g., norepinephrine if elevated normetanephrines preoperatively)
- Vasopressin and methylene blue - for vasopressor-refractory cases
Glucose management
- Intraoperative hyperglycaemia: catecholamine excess causes insulin resistance and decreased secretion - correct judiciously (residual insulin effect causes postop hypoglycaemia)
- Post-vein ligation: rebound hypoglycaemia risk (especially with epinephrine-secreting tumours)
6. Postoperative Management
| Issue | Management |
|---|---|
| ICU monitoring | Routine for all; HDU acceptable for haemodynamically stable patients after laparoscopic resection |
| Hypotension | Continue vasopressors as needed; usually resolves within 24-48 h |
| Hypoglycaemia | Monitor glucose every 1-2 hours for first 6-24 h; rebound hyperinsulinaemia especially with epinephrine-secreting tumours |
| Residual hypertension | ~50% remain hypertensive for 1-3 days (residual elevated plasma catecholamines declining); most normalise over weeks, but 25% remain permanently hypertensive (essential hypertension unmasked or residual/metastatic disease) |
| Pain | IV analgesia; epidural if placed (note hypotension risk) |
7. Special Scenarios
Undiagnosed pheochromocytoma discovered intraoperatively
- Unexpected severe hypertension + tachycardia during abdominal manipulation
- Treat with nitroprusside + esmolol; convert to controlled resection if feasible
- Abort surgery if haemodynamic control unachievable; prepare formally and reschedule
Bilateral pheochromocytoma / MEN 2
- Risk of postoperative adrenal insufficiency - steroid cover required
- Consider cortisol-sparing approach; partial adrenalectomy may be appropriate in hereditary cases
Pregnancy
- Rare but life-threatening; maternal and foetal mortality high if undiagnosed
- Alpha blockade (phenoxybenzamine) after 1st trimester; surgical resection before 24 weeks if possible; otherwise deliver then resect
- 2025 BJA Education review highlights evolving management (Management of phaeochromocytoma in pregnancy)
Catecholamine-induced cardiomyopathy
- May be severe but is reversible after resection
- Preoperative echocardiogram mandatory when suspected
- Cautious fluid management; TOE intraoperatively
- Heart failure may improve markedly within weeks after tumour removal
8. Key Messages - Quick Reference
| Phase | Key Points |
|---|---|
| Preop | Alpha-block first (minimum 7-14 days) → then beta-block if needed → volume load; target BP <130/80 mmHg |
| Induction | Arterial line pre-induction; deep anaesthesia before intubation; propofol or etomidate |
| Avoid | Ketamine, halothane, desflurane, pancuronium, large-bolus morphine/atracurium, ephedrine |
| Hypertension | Clevidipine, nicardipine, nitroprusside, phentolamine, esmolol, Mg sulphate |
| Post-ligation | Aggressive fluids; phenylephrine/norepinephrine; watch glucose |
| Postop | ICU; glucose q1-2h; expect residual hypertension 1-3 days; 50% normalize BP |
Sources:
- Miller's Anesthesia, 10th Edition, pp. 4240-4246 (Chapter on Pheochromocytoma - preoperative, intraoperative, postoperative management)
- Morgan & Mikhail's Clinical Anesthesiology, 7th Edition, pp. 1431-1432 (Catecholamine Excess - Anesthetic Considerations)
- Campbell Walsh Wein Urology, 3-Volume Set (Fig. 106.20 - Preoperative medical management pathways)
- Fischer's Mastery of Surgery, 8th Edition, pp. 1338 (Pheochromocytoma preoperative preparation)
- Mulholland & Greenfield's Surgery, 7th Edition, p. 4182-4183 (Treatment and intraoperative management)
- 2025 European Clinical Guidance: European guidance on adrenal management - confirms alpha blockade ≥7-14 days before surgery as cornerstone
Recent evidence note (2025): A Frontiers in Endocrinology study found that prolonged alpha-blockade >30 days and doxazosin use were associated with more hypertensive crises intraoperatively and greater vasopressor requirements postoperatively compared to phenoxybenzamine and shorter preparation - suggesting the timing and agent choice matters more than simply "longer is better." This aligns with the Miller's note (PMID data) that >30-day preoperative blockade correlates with intraoperative bradycardia and postoperative hypotension.
This is a shared conversation. Sign in to Orris to start your own chat.