Aortic Coarctation
Reading File
Finding Sources
Finding Sources
Searching PubMed
"coarctation of the aorta" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to write a detailed response on aortic coarctation. Let me compile this into a thorough answer.
Aortic Coarctation
Definition and Prevalence
Coarctation of the aorta (CoA) is a localized or tubular narrowing of the aorta, almost always congenital in origin. First described by Morgagni in 1760, it accounts for approximately 5-8% of all congenital heart defects and represents a generalized arteriopathy - not merely a focal obstruction - with decreased aortic compliance that persists even after successful repair.
- Braunwald's Heart Disease, p. 898
Anatomy and Location
The coarctation is typically juxtaductal - at the junction of the distal aortic arch and the descending aorta, just distal to the left subclavian artery origin, opposite or adjacent to the ductus arteriosus. It forms as a posterior/lateral shelf in the aortic wall.
Classification by position relative to the ductus:
| Type | Location | Clinical significance |
|---|---|---|
| Preductal | Proximal to ductus arteriosus | Rarer; ductal-dependent circulation in neonates; differential cyanosis |
| Juxtaductal | At the level of the ductus | Most common |
| Postductal | Distal to ductus arteriosus | Often presents later in life with hypertension |
The coarctation can also be classified by position relative to the left subclavian artery (proximal or distal).
- Frameworks for Internal Medicine, p. 524
- ROSEN's Emergency Medicine, p. 1357
Associated Anomalies
CoA is rarely an isolated lesion. Common associations include:
-
Bicuspid aortic valve (BAV): 50-85% of cases (most common association)
-
Ventricular septal defect (VSD)
-
Mitral valve abnormalities
-
Subaortic obstruction
-
Anomalous origin of the right subclavian artery
-
Intracranial (Berry) aneurysms in the Circle of Willis
-
Turner syndrome, Noonan syndrome, Williams-Beuren syndrome
-
Shone syndrome: CoA + parachute mitral valve + supramitral ring + multilevel left-sided LVOTO
-
Braunwald's Heart Disease, p. 898
Pathophysiology
Two main mechanisms underlie hemodynamic disturbance:
- Mechanical obstruction: reduces flow to the lower body, causing lower extremity hypoperfusion.
- Pressure overload proximal to the narrowing: causes upper-body hypertension and LV pressure overload.
Over time, collateral vessels develop (internal mammary, intercostal, posterior mediastinal arteries) to bypass the obstruction and maintain lower-body perfusion. The ductus arteriosus also acts as a bypass in neonates - its closure precipitates cardiovascular collapse in severe preductal coarctation.
In preductal coarctation with a patent ductus arteriosus: the lower body receives deoxygenated blood via right-to-left ductal shunting, producing differential cyanosis (pink upper body, cyanotic lower body).
- Grainger & Allison's Diagnostic Radiology, p. 222
- ROSEN's Emergency Medicine, p. 1360
Clinical Presentation
CoA follows a bimodal distribution:
Neonates and Infants (Severe Coarctation)
- Cardiovascular collapse and shock when the ductus closes
- Congestive heart failure, tachycardia, poor feeding
- Differential cyanosis (preductal type)
Older Children and Adults (Milder Coarctation)
- Asymptomatic hypertension - most common presentation
- Headache
- Leg claudication / cold legs
- Discovered incidentally on murmur or hypertension workup
Key Physical Findings:
- Brachial-femoral delay (palpate both pulses simultaneously)
- BP differential: systolic BP right arm > lower extremities by ≥15-20 mmHg
- Reduced femoral pulses
- Systolic murmur best heard over the back / interscapular area
- Continuous interscapular murmurs suggest collateral flow
- S4 gallop from LV hypertrophy
- Hypertensive retinopathy on fundoscopy
If the left subclavian artery is sacrificed during repair, left arm BP can be misleadingly low - always use the right arm for BP measurement.
- Braunwald's Heart Disease, p. 898; Frameworks for Internal Medicine, p. 524
Investigations
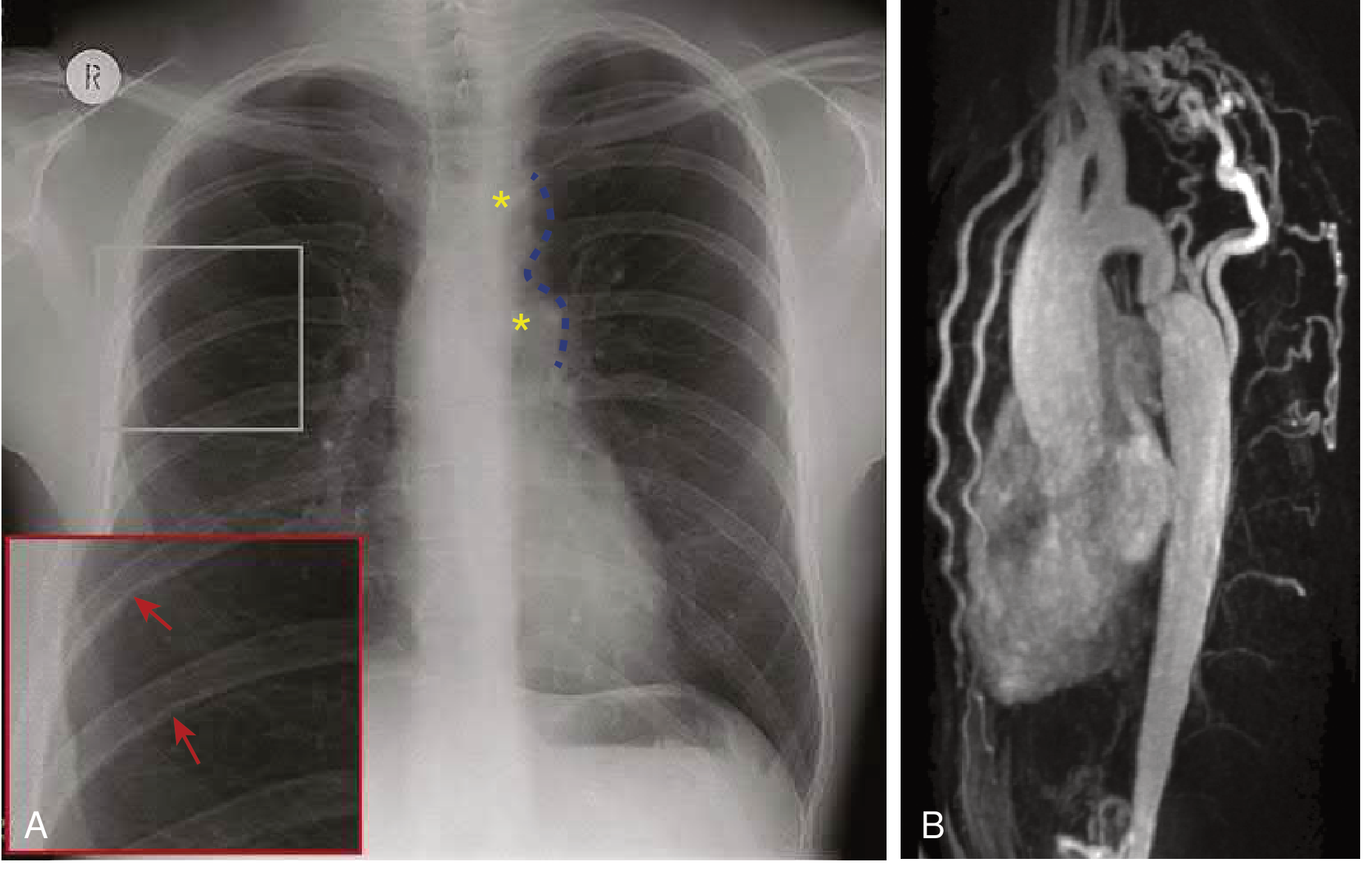
Chest X-Ray
- Rib notching: erosion of the inferior border of the posterior 3rd-9th ribs (from dilated intercostal collaterals) - typically bilateral, rarely seen before age 5
- "Figure 3" sign: mediastinal silhouette showing pre-stenotic dilation of the aortic arch + post-stenotic dilation of the descending aorta
ECG
- Left ventricular hypertrophy
- Left atrial enlargement
- Ischemic changes (in adults)
Echocardiography
- Assesses coarctation site, aortic valve, LV function and mass
- Continuous wave Doppler from suprasternal view: increased velocity at coarctation, diastolic tail in descending aorta, and continuous flow in abdominal aorta suggest significant stenosis
Cardiac MRI (CMR) - Primary imaging modality
- Quantifies LV mass, arch hypoplasia, collateral flow, coarctation severity
- Identifies post-repair complications (aneurysms, recoarctation, dissection)
- Preferred over CT if no contraindications
Cardiac CT
- Better for assessing stent lumen integrity, fracture, and coronary arteries
Cardiac Catheterization
-
Peak-to-peak gradient ≥20 mmHg across the coarctation (in the absence of well-developed collaterals) = hemodynamically significant
-
Braunwald's Heart Disease, p. 898; Grainger & Allison's Diagnostic Radiology, p. 228
Natural History (Untreated)
Without correction:
-
Mean life expectancy: 35 years
-
90% of patients die before age 50
-
Causes of death: coronary artery disease, stroke, aortic dissection, congestive heart failure, intracranial hemorrhage from aneurysm rupture
-
Frameworks for Internal Medicine, p. 524
Management
Neonates/Infants (Ductal-Dependent)
- Prostaglandin E1 (PGE1) to maintain ductal patency until surgical repair
- Primary surgical repair in infancy
Children
- Surgery: resection + end-to-end anastomosis (preferred in infants/young children)
- Balloon angioplasty may be considered for native or recurrent coarctation
Adults - Intervention Indications:
Intervention is indicated when:
- Hypertensive patient with invasive peak-to-peak gradient ≥20 mmHg
- Coarctation diameter ≤50% of aortic diameter at the diaphragm in a hypertensive patient (regardless of gradient)
- Normotensive patient with gradient ≥20 mmHg
Adult Treatment of Choice:
- Endovascular stenting - preferred over surgery in adults when technically feasible
- Covered stents preferred to prevent/treat acute wall injury
- Surgery reserved for complex anatomy (interrupted arch, long-segment coarctation, aneurysmal disease) - options include interposition graft, ascending-to-descending aorta bypass conduit
Medical Management:
-
Antihypertensives: beta-blockers, ACE inhibitors, ARBs (first-line)
-
Aggressive BP and lipid control to prevent atherosclerotic complications
-
Braunwald's Heart Disease, p. 898; Frameworks for Internal Medicine, p. 524
Post-Repair Complications and Follow-Up
Even after successful repair, CoA is NOT cured - it requires lifelong surveillance:
| Complication | Details |
|---|---|
| Persistent/recurrent hypertension | >50% of adults, especially if repaired late; aortic compliance permanently reduced |
| Recoarctation | Up to 35% after balloon dilation; less with primary stenting |
| Aortic aneurysm | Especially after Dacron patch aortoplasty (opposite wall becomes aneurysmal) |
| Aortic dissection | Late risk, related to aortopathy |
| BAV complications | Aortic stenosis/regurgitation, ascending aortic dilation |
| Coronary artery disease | From chronic hypertension |
| Exercise-induced hypertension | Linked to adverse LV remodeling |
Cross-sectional imaging (CMR) should be performed at intervals of at least 3-5 years lifelong.
- Braunwald's Heart Disease, p. 898; Grainger & Allison's Diagnostic Radiology, p. 234
Key Summary Points
| Feature | Detail |
|---|---|
| Most common site | Juxtaductal (distal to left subclavian artery) |
| Most common association | Bicuspid aortic valve (50-85%) |
| Classic CXR findings | Rib notching + "figure 3" sign |
| Classic physical exam | Brachial-femoral delay + upper > lower extremity BP |
| Significant gradient | ≥20 mmHg peak-to-peak |
| Adult treatment of choice | Endovascular stenting |
| Untreated life expectancy | ~35 years |
Sources:
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, Ch. 82
- Frameworks for Internal Medicine, p. 524
- ROSEN's Emergency Medicine, Ch. 165
- Grainger & Allison's Diagnostic Radiology, Ch. 13
This is a shared conversation. Sign in to Orris to start your own chat.