Incision in total laryngectomy
Reading File
Finding Sources
Finding Sources
Searching Images
total laryngectomy incision surgical approach
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and diagrams. Here is a complete answer:
Incision in Total Laryngectomy
Incision Design Options
There are two principal incision designs (apron flap variants), plus a rarely used U-shaped option.
1. Long Apron Flap (Long-Flap Approach)
Fig. 109.1A — Cummings Otolaryngology
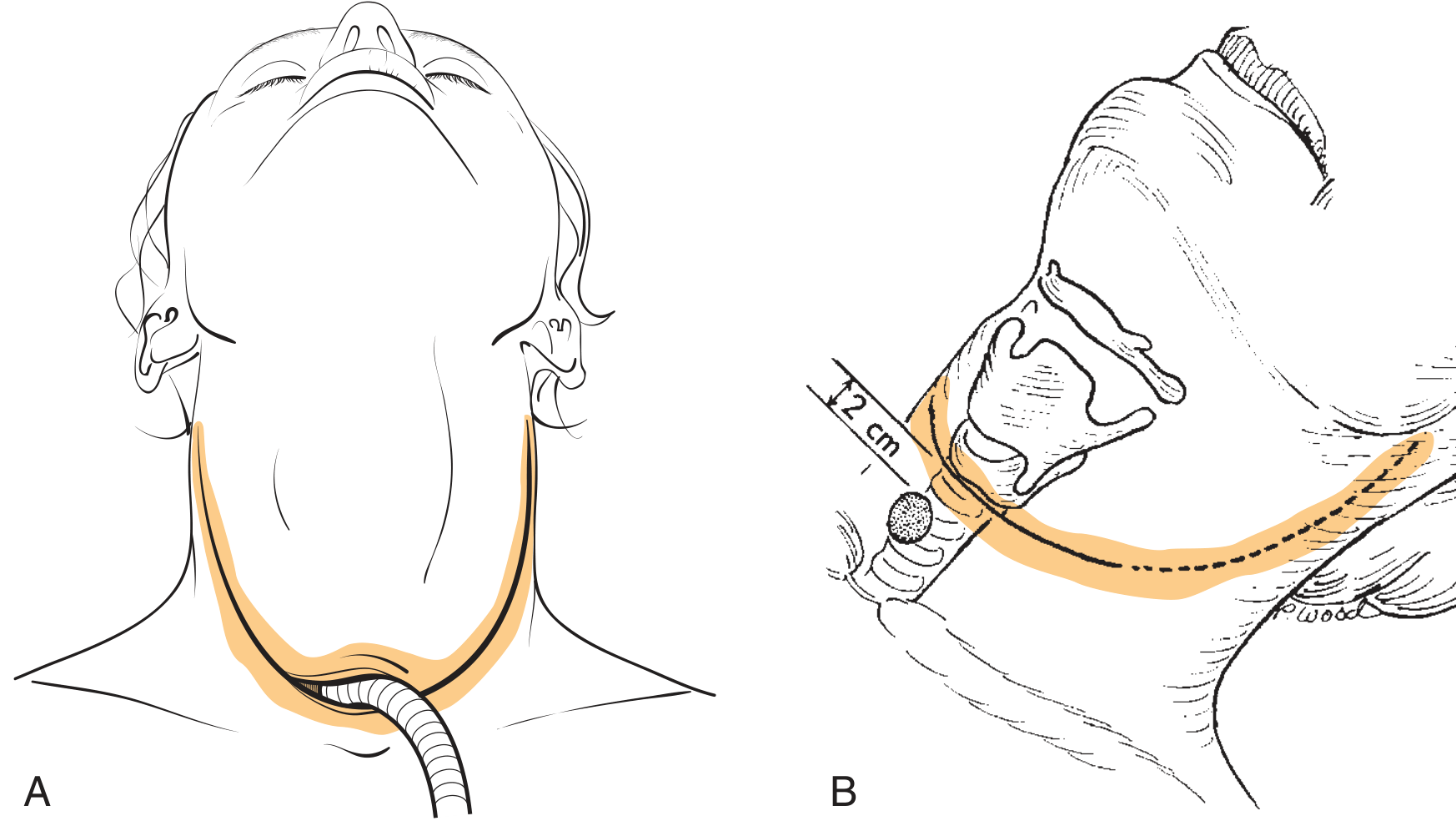
- A single, broad curvilinear horizontal incision running from mastoid tip to mastoid tip, intersecting the midline at approximately the level of the cricoid cartilage — usually about 2 cm above the sternal notch in the midline.
- The tracheostomy stoma is incorporated in the line of the incision itself (the tracheal end exits through the center of the lower flap).
- The superior flap is elevated to expose the entire laryngeal framework.
Advantages:
- More reliable stoma creation
- Avoids a bipedicled skin bridge between two separate incisions, which can cause stoma stenosis
- Preferred when concurrent bilateral neck dissections are performed (incision can be extended toward the mastoid tips)
Disadvantage:
- A technically demanding three-point closure is required at the stoma site (lower stoma edge is created within the flap)
- If pharyngocutaneous fistula occurs and requires diversion, the stoma may be involved in the resulting wound
2. Short Apron Flap with Separate Tracheostome Incision
Fig. 109.2 — Short flap with skin bridge

- The main flap incision is placed higher in the neck.
- The tracheostomy skin incision is made 2–3 cm inferior to the flap incision as a separate elliptical incision, creating a skin bridge between the two.
- The stoma is fashioned by excising a shield-shaped skin island from the lower neck in the midline, just above the sternal notch.
Advantages:
- If pharyngocutaneous fistula develops requiring wound diversion, the stoma is less likely to be involved — particularly important in previously irradiated patients
- Avoids the technically complex bilateral three-point closures at the stoma necessitated by the long-flap approach
- Simpler stoma construction
Disadvantage:
- The bipedicled skin bridge between flap and tracheostomy incision can lead to stomal stenosis
3. U-Shaped Incision
- Rarely used
- Feasible when neck dissection is not performed
- Not routinely recommended
Positioning and Planning Principles
- Patient is placed on a table with a head holder that allows the head to be cantilevered (extended), facilitating bilateral neck dissection.
- The operating table is turned 180° from the anesthesiologist to maximize surgeon access.
- Airway planning is coordinated with anesthesia preoperatively:
- Unobstructed airway → orotracheal intubation at induction; tube is removed at tracheotomy or left in until tracheal transection
- Obstructed airway / risk of tumour displacement → preliminary tracheotomy under local anesthesia, with the skin incision at the intended final stoma site
- The tracheotomy skin incision is made at the intended final stoma site — this is the same incision used for the permanent stoma.
Summary Table
| Feature | Long Apron Flap | Short Apron Flap |
|---|---|---|
| Extent | Mastoid tip to mastoid tip | Shorter, higher in neck |
| Stoma position | In the flap incision line | Separate, 2–3 cm below flap |
| Stoma stenosis risk | Lower | Higher (skin bridge) |
| Fistula-related stoma involvement | Higher | Lower |
| Preferred in irradiated patients | No | Yes |
| Closure complexity | Three-point stoma closure | Simpler |
Source: Cummings Otolaryngology Head and Neck Surgery, Chapter 109 (Fig. 109.1, 109.2)
This is a shared conversation. Sign in to Orris to start your own chat.