Rcc its staging staging and role mri and ct scan
Reading File
Finding Sources
Finding Sources
Searching PubMed
"renal cell carcinoma"[MeSH Terms] AND "staging"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-cited answer. Here it is:
Renal Cell Carcinoma (RCC): Staging, CT, and MRI
Overview
Renal cell carcinoma (RCC) is the most common malignant renal tumor in adults, accounting for 2-3% of all adult malignancies. It is not a single disease - it encompasses a group of histologically distinct entities with different genetic profiles and metastatic potential:
- Clear cell RCC - 65% of tumors, accounts for 90% of metastases; chromosome 3 abnormalities; most virulent
- Papillary RCC - chromosome 7, 17, or Y aberrations; more indolent
- Chromophobe RCC - more indolent
- Collecting duct / medullary carcinoma - rare, aggressive
- Oncocytoma - benign (10% of all renal tumors)
Over 50% of RCCs are now diagnosed incidentally on cross-sectional imaging. The classic triad (flank pain + gross hematuria + palpable mass) is seen in fewer than 5% of patients today. Despite this, 30% still present with metastatic disease.
TNM Staging (AJCC 2017)
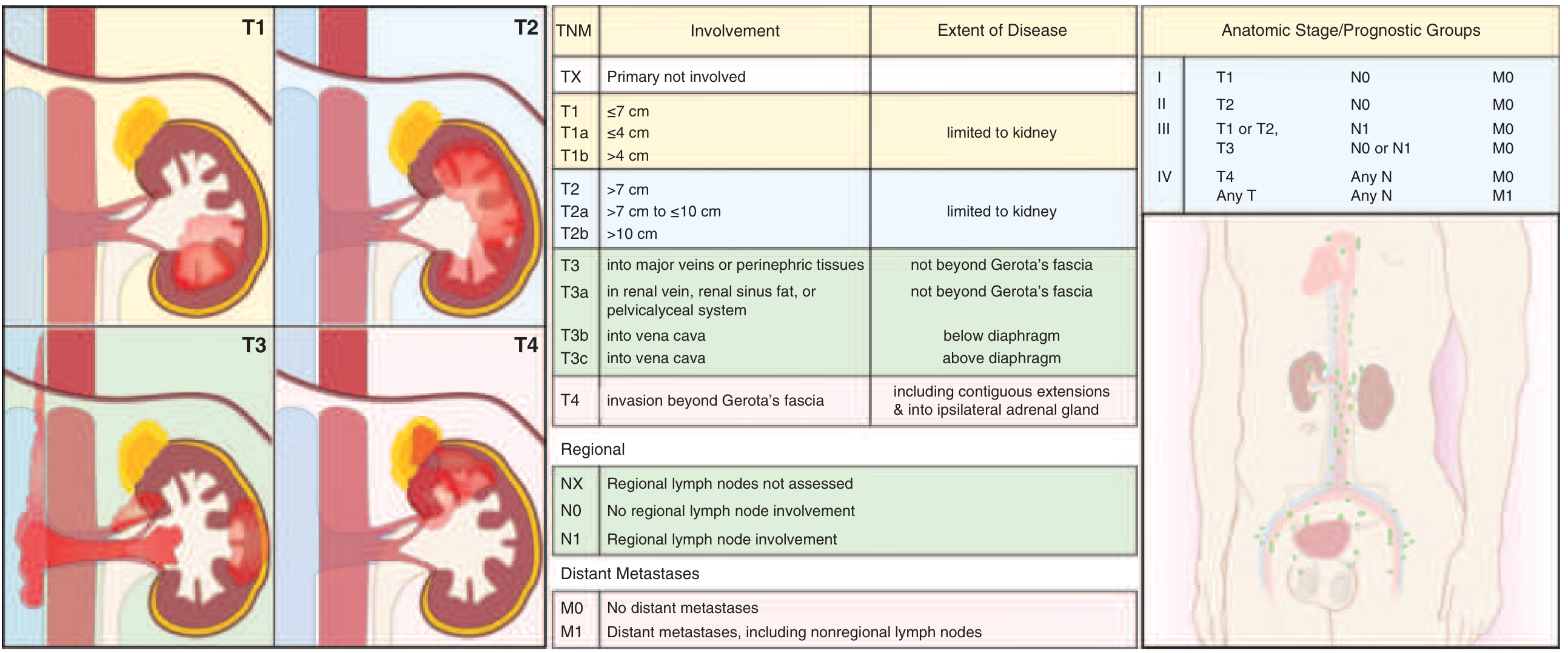
FIGURE: RCC staging - TNM system (Harrison's Principles of Internal Medicine, 22e)
T (Primary Tumor)
| Stage | Description |
|---|---|
| T1a | Tumor confined to kidney, <4 cm |
| T1b | Tumor confined to kidney, >4 cm but <7 cm |
| T2a | Tumor confined to kidney, >7 cm but ≤10 cm |
| T2b | Tumor confined to kidney, >10 cm |
| T3a | Spread to perinephric fat, renal sinus fat, renal vein, or pelvicalyceal system - not beyond Gerota's fascia |
| T3b | Tumor thrombus extends into IVC below the diaphragm |
| T3c | Tumor thrombus extends into IVC above the diaphragm, or invades the wall of the IVC |
| T4 | Spread outside Gerota's fascia, or contiguous infiltration of the ipsilateral adrenal gland |
N (Regional Lymph Nodes)
| Stage | Description |
|---|---|
| N0 | No regional lymph node involvement |
| N1 | Metastasis in regional lymph node(s) |
Note: Some older texts (Grainger & Allison) retain N1/N2 distinction (single vs. multiple nodes); the current 8th edition AJCC collapses this to N1 = any regional node involvement.
M (Distant Metastasis)
| Stage | Description |
|---|---|
| M0 | No distant metastases |
| M1 | Distant metastases (including non-regional lymph nodes) |
Anatomic Stage Groups
| Group | T | N | M |
|---|---|---|---|
| Stage I | T1 | N0 | M0 |
| Stage II | T2 | N0 | M0 |
| Stage III | T1 or T2 | N1 | M0 |
| T3 | N0 or N1 | M0 | |
| Stage IV | T4 | Any N | M0 |
| Any T | Any N | M1 |
Distribution at presentation: ~65% present Stage I/II, 15-20% Stage III, 15-20% Stage IV.
5-year survival: ~77% overall, but varies dramatically by stage (near 100% for Stage I vs. <15% for Stage IV).
Histologic Grading
Fuhrman nuclear grading system (Grade I to IV) is used for histologic grading. The WHO/ISUP grading system has now largely replaced it but uses similar principles based on nuclear size, contour, and nucleolar prominence.
Role of CT Scan
CT is the primary modality for both diagnosis and staging of RCC.
What CT Does Well:
- Detection: Contrast-enhanced CT identifies renal masses with high sensitivity. Enhancement of >20 HU after IV contrast is the hallmark of malignancy.
- Staging accuracy: Overall accuracy 72-90%.
- Perinephric/T3a disease: A discrete soft-tissue mass in the perinephric space is 98% specific for T3a disease (though sensitivity is only 46%). Perinephric fat stranding alone is nonspecific - present in T1/T2 disease due to edema or fibrosis.
- Vascular invasion (T3b/T3c): CT detects renal vein and IVC tumor thrombus with good accuracy, though IVC thrombus level (below vs. above diaphragm) is important for surgical planning.
- Lymph node staging: Based on size criterion (>1 cm = abnormal). Overall accuracy 83-89%. Micrometastases in normal-sized nodes are missed; reactive enlargement causes false positives.
- Distant metastases: CT of chest, abdomen, and pelvis detects lung, liver, adrenal, and nodal metastases. Chest CT is preferred over plain CXR when metastatic disease is clinically suspected.
- Calcification: CT is better than MRI at detecting small foci of calcification.
- Bosniak classification of cystic renal masses is based on CT appearances (Category I = simple cyst, 0% malignancy; Category IV = 70% malignancy risk).
CT Limitation:
- T2 vs. early T3a: CT is not accurate in distinguishing T2 from early T3a disease (though clinically significant mainly for nephron-sparing decisions).
- Less reliable for IVC thrombus level determination compared to MRI.
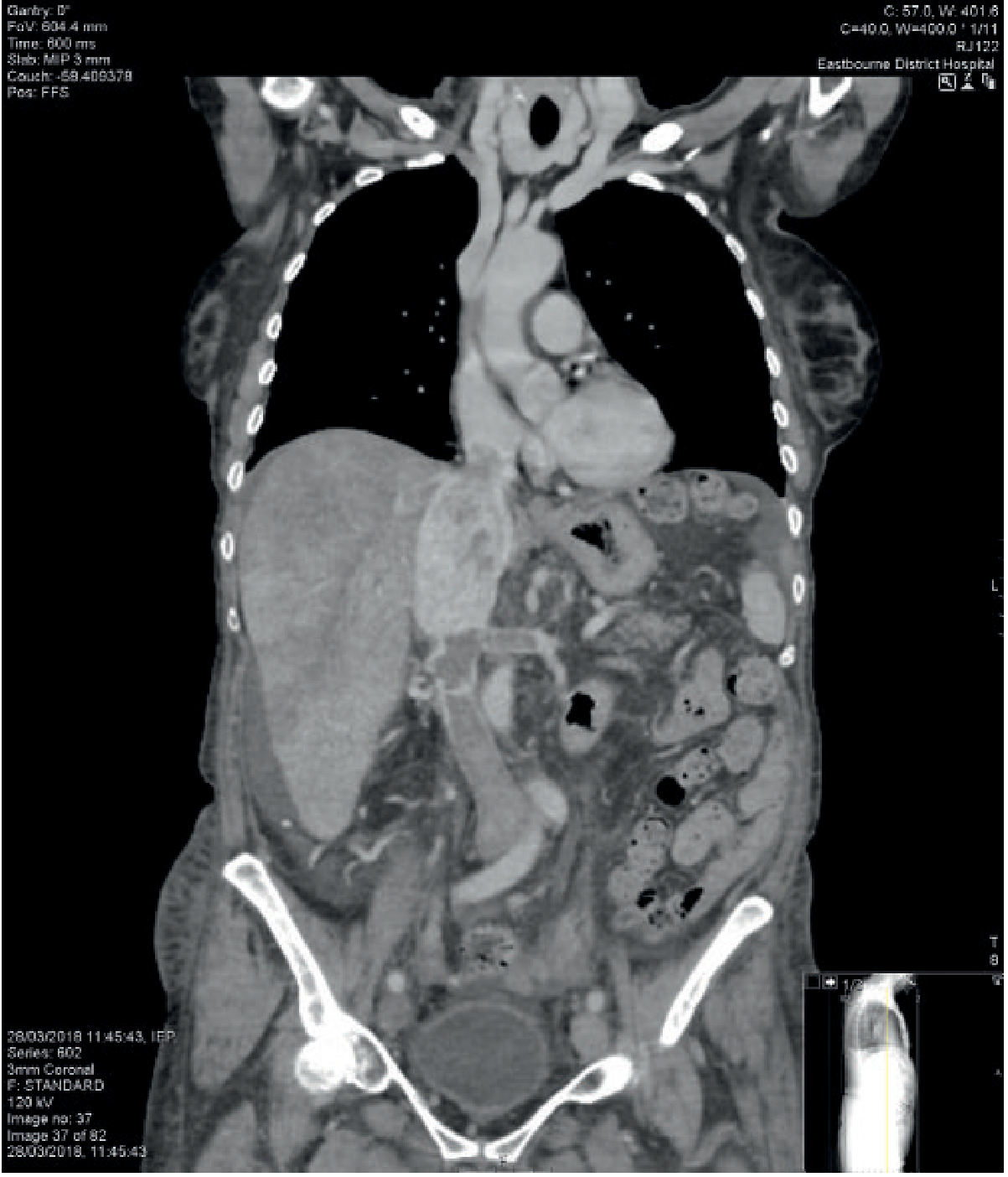
Fig: T3c RCC - Coronal CT showing extensive caval tumor extending into the right atrium from a right renal cell cancer. Note heterogeneous liver enhancement from hepatic vein obstruction. (Grainger & Allison's Diagnostic Radiology)
Role of MRI
MRI has a complementary and problem-solving role rather than being a first-line modality for RCC.
When MRI is Preferred or Indicated:
-
IVC tumor thrombus assessment (T3b/T3c): MRI is superior to CT for determining the precise cranial extent of IVC thrombus - critical for surgical planning (determines whether cardiac bypass is needed). This is its most important indication.
-
Contraindication to CT contrast: When iodinated contrast is contraindicated (e.g., severe renal impairment, contrast allergy), gadolinium-enhanced MRI is the alternative. Note: gadolinium-based contrast should also be used with caution in severe CKD (NSF risk).
-
Problem-solving for indeterminate masses: MRI helps characterize masses that are equivocal on CT - particularly for distinguishing fat-poor angiomyolipoma from RCC, or evaluating complex cystic lesions.
-
Pregnancy: Avoidance of ionizing radiation.
-
Surveillance after ablation (RFA/cryotherapy): MRI can assess residual enhancement at ablation sites.
MRI Signal Characteristics of RCC:
- T1-weighted: Isointense or hypointense compared to renal cortex
- T2-weighted: Slightly hyperintense
- Post-gadolinium: Heterogeneous enhancement immediately after injection, decreasing on delayed images. Small, low-grade tumors show more homogeneous enhancement.
MRI Limitations:
- Respiratory misregistration - more prone than CT to motion artifact
- Calcification detection: Inferior to CT for small calcification foci
- Lymph node assessment: Not significantly better than CT for nodal disease
- Cost, availability, scan time: Less practical as a first-line tool
Summary: CT vs MRI in RCC
| Feature | CT | MRI |
|---|---|---|
| First-line staging | Yes (preferred) | No (second line) |
| Detection sensitivity | High | Similar to CT |
| Calcification detection | Superior | Inferior |
| Perinephric extension | Good | Good |
| Renal vein invasion | Good | Good |
| IVC thrombus extent | Good | Superior |
| Lymph node staging | Based on size, 83-89% | Not better than CT |
| Problem-solving equivocal masses | Good | Superior |
| Contrast contraindicated | Replaced by MRI | First-line alternative |
| Respiratory artifact | Less prone | More prone |
| Availability/cost | Better | More limited |
Initial Workup Protocol
Standard evaluation per Harrison's (22e) and Sabiston:
- Contrast-enhanced CT abdomen and pelvis (primary staging)
- Chest radiograph (if negative for metastases, stop; if suspicious, add chest CT)
- Urinalysis and labs (CBC, metabolic panel, LFTs, LDH, corrected calcium)
- Bone scan / brain imaging - only if clinically indicated (bone pain, elevated alkaline phosphatase, neurologic symptoms)
- MRI abdomen - if IVC thrombus extent unclear, or contrast contraindicated
Sources: Grainger & Allison's Diagnostic Radiology; Harrison's Principles of Internal Medicine 22e; Sabiston Textbook of Surgery; Goldman-Cecil Medicine
For mr radiology long essay
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Rcc its staging staging and role mri and ct scan rdaiolong md long essqy
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Create a Word document with the complete MD radiology long essay on RCC staging, CT, and MRI
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.