Anuerysmal bone cyst
Reading File
Finding Sources
Searching PubMed
"aneurysmal bone cyst"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Aneurysmal Bone Cyst (ABC)
Definition
An aneurysmal bone cyst is a locally destructive, blood-filled, reactive lesion of bone - not a true neoplasm. It consists of multiloculated, hemorrhagic cystic spaces within an expanding shell of bone.
Epidemiology
- Primarily affects patients younger than 20 years (1st-2nd decades)
- Slight female predominance
- Any bone can be involved
Common Locations
| Site | Notes |
|---|---|
| Proximal humerus | Most common long bone site |
| Distal femur | Frequent |
| Proximal tibia | Frequent |
| Spine (posterior elements) | 15-20% of cases; may extend into vertebral body |
| Flat bones | Less common |
The lesion arises eccentrically in the metaphysis and does not cross the growth plate.
Pathogenesis
Two mechanisms are recognized:
1. Primary (de novo):
Spindle-shaped cells show rearrangements of chromosome 17p13, causing fusion of USP6 gene coding sequences to regulatory elements of COL1A1 (most common) or other genes. This leads to USP6 overexpression - a deubiquitinating enzyme that upregulates NF-kB, which in turn increases matrix metalloprotease expression, causing cystic bone resorption.
2. Secondary (up to 30% of cases):
ABC-like changes arise within other bone tumors, including:
- Giant cell tumors
- Chondroblastomas
- Osteoblastomas
- Fibrous dysplasia
- Nonossifying fibromas
- Chondromyxoid fibromas
A local circulatory disturbance causing increased venous pressure and hemorrhage has also been proposed.
Morphology
Radiography
- Eccentric, expansile, lytic, metaphyseal lesion with well-defined margins
- Thin shell of overlying cortical bone (periosteum elevated but intact)
- May occasionally have a permeative appearance mimicking malignancy
CT
- Delineates complex anatomy (spine, pelvis)
- Identifies the thin cortical rim
- Shows multiloculated architecture
MRI (most informative)
- Fluid-fluid levels - the hallmark finding (arrow in image below)
- Double-density fluid levels + intralesional septations distinguish ABC from unicameral bone cyst
- Multiloculated cavities clearly demonstrated
Bone Scan
- Diffuse or peripheral tracer uptake with central area of decreased uptake ("doughnut sign")
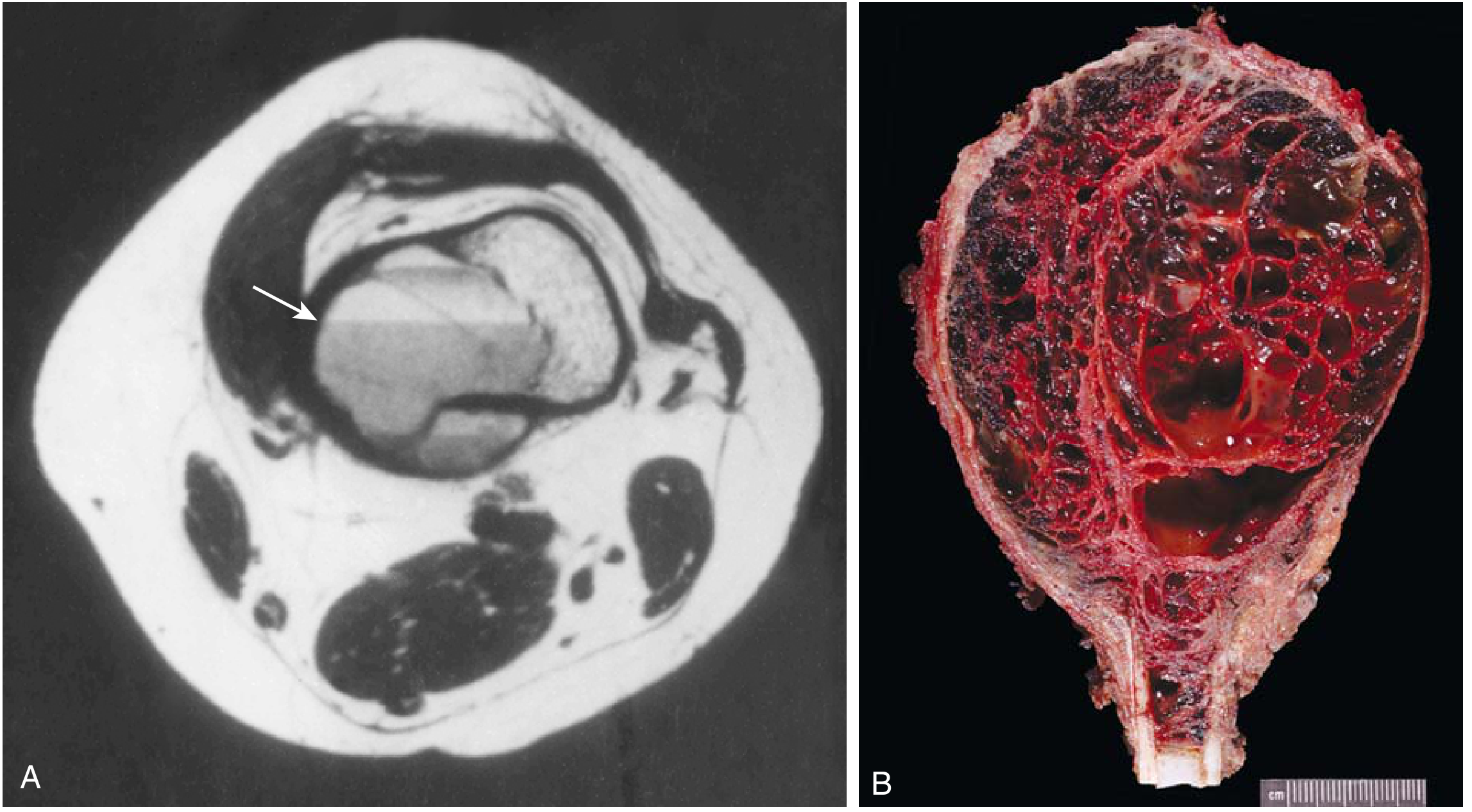
Gross
- Multiple blood-filled cystic spaces separated by thin tan-white septa
- Surrounded by a thin layer of bone covered by raised periosteum
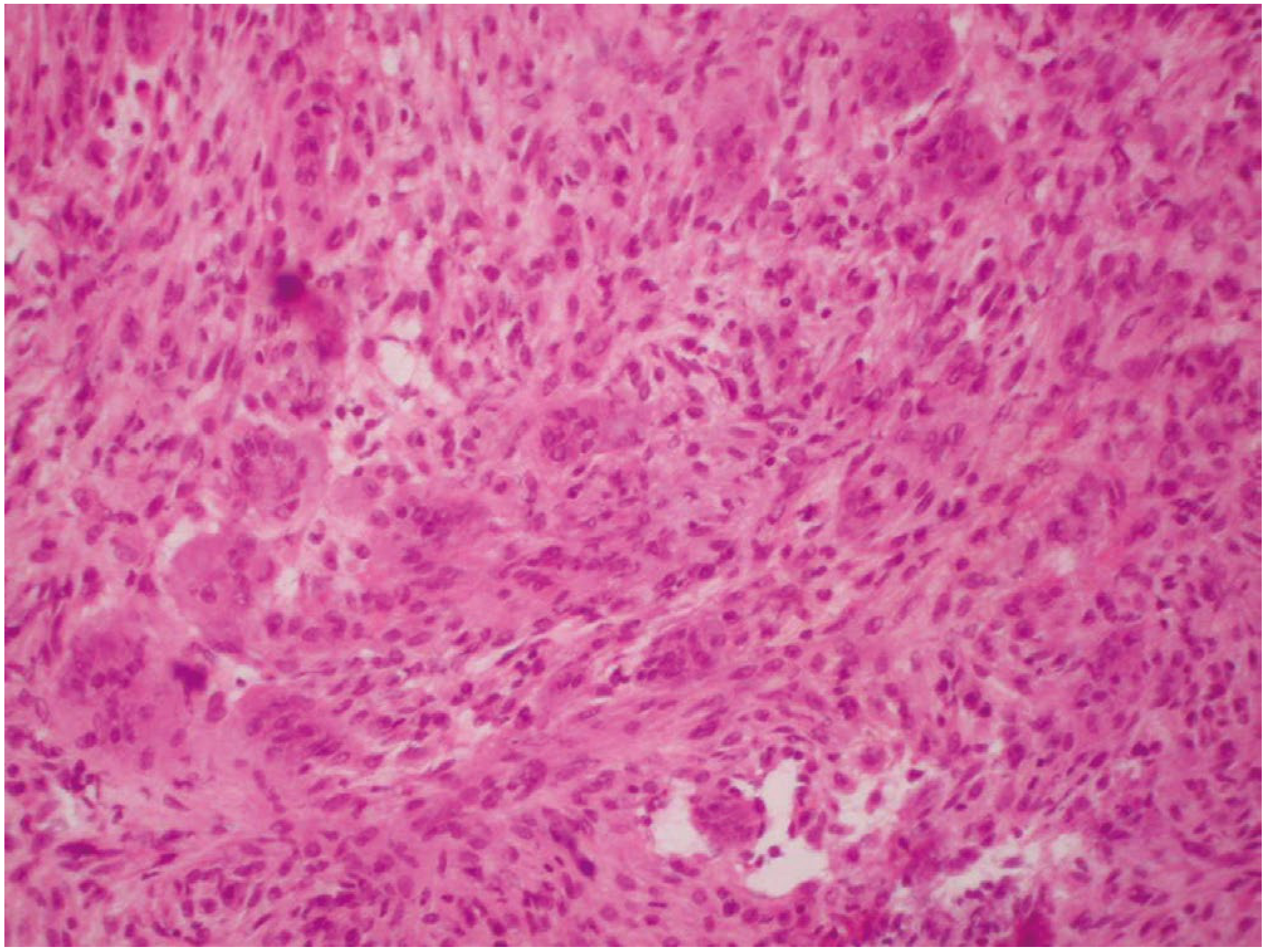
Microscopy
- Cystic spaces lack an endothelial lining
- Septa contain:
- Plump uniform fibroblasts and histiocytes
- Multinucleate osteoclast-like giant cells
- Hemosiderin-laden macrophages
- Reactive woven bone
- Chronic inflammatory cells
Clinical Features
- Localized pain and swelling (present for weeks to months)
- Limitation of motion
- Rapid growth can mimic a malignancy clinically
- Spinal lesions may cause neurologic deficits or radicular pain
- Although benign, ABCs are locally aggressive
Differential Diagnosis
The radiographic and clinical appearance overlaps with:
- Giant cell tumor - most important mimic (especially in adults)
- Enchondroma
- Unicameral (simple) bone cyst - distinguished by centrally located unilocular cyst with clear fluid
- Telangiectatic osteosarcoma - most dangerous mimic; biopsy mandatory
Solid Variant
A solid variant of ABC exists, frequently referred to as giant cell reparative granuloma, which lacks the classic blood-filled spaces.
Treatment
| Setting | Preferred Treatment |
|---|---|
| Standard long bone lesion | Extended curettage + bone graft substitute |
| Expendable bones | Marginal resection |
| Spine/pelvis | Preoperative arterial embolization to minimize blood loss, then curettage |
| Inaccessible lesions | Percutaneous sclerotherapy (fluoroscopic guidance) |
| High surgical risk | Denosumab (anti-RANKL monoclonal antibody) |
| Historical/rarely used | Low-dose radiation (risk of malignant transformation precludes routine use) |
Key surgical note: Tourniquet control is advised due to heavy bleeding potential.
Recurrence
- After curettage: 10-20% recurrence rate (Robbins: up to 50% in some series)
- Risk factors for recurrence:
- Age younger than 15 years
- Centrally located cysts
- Incomplete removal of cystic cavity contents
- Recurrent cysts can be retreated with the same approach
Summary Comparison: ABC vs Unicameral Bone Cyst
| Feature | ABC | Unicameral BC |
|---|---|---|
| Age | 1st-2nd decade | 1st-2nd decade |
| Sex | Slight female predominance | Male:female 2:1 |
| Location | Eccentric, metaphyseal | Central, metaphyseal |
| Common sites | Proximal humerus, distal femur, tibia, spine | Proximal humerus, proximal femur |
| MRI | Fluid-fluid levels, double-density, septa | Simple cyst, no septa |
| Fluid | Blood-filled | Straw-colored fluid |
| Presentation | Pain | Usually silent; pathologic fracture |
| Treatment | Extended curettage | Observation/aspiration/injection |
Sources:
- Robbins & Kumar Basic Pathology, p. 787 (Robbins Pathology)
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 1172, 4548-4549
- Grainger & Allison's Diagnostic Radiology, p. 1959
This is a shared conversation. Sign in to Orris to start your own chat.