Gorrila face in acromega
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Excellent - I now have rich textbook content and images. Here is the complete answer:
"Gorilla Face" in Acromegaly
The term gorilla face (also called simian face) describes the characteristic coarse, ape-like facial appearance that develops in acromegaly due to chronic excess growth hormone (GH), which acts via IGF-1 to drive bony and soft-tissue overgrowth.
Clinical Image - Serial Progression
The photographs below (from Goldman-Cecil Medicine) show the progressive coarsening of facial features in a woman with acromegaly over a 9-year period (1997 to 2006), alongside her pituitary MRI:
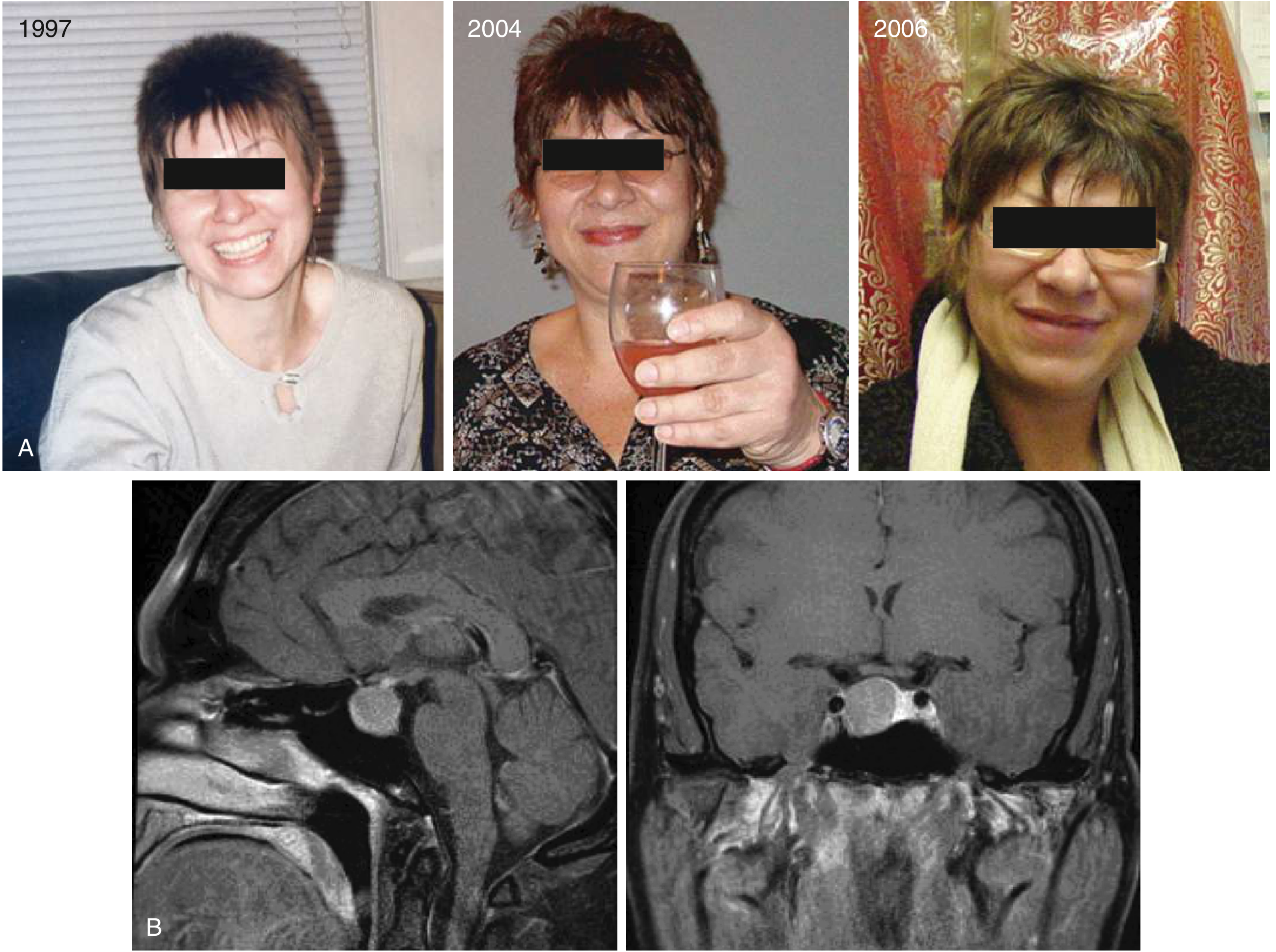
Goldman-Cecil Medicine - Progressive coarsening of facial features including enlargement of nose and lips, development of prognathism, and enlarged hands
Bony Changes (the "Gorilla" Skeleton)
The image below shows a patient (A) and an acromegalic skull (B), illustrating the classic bony remodeling:
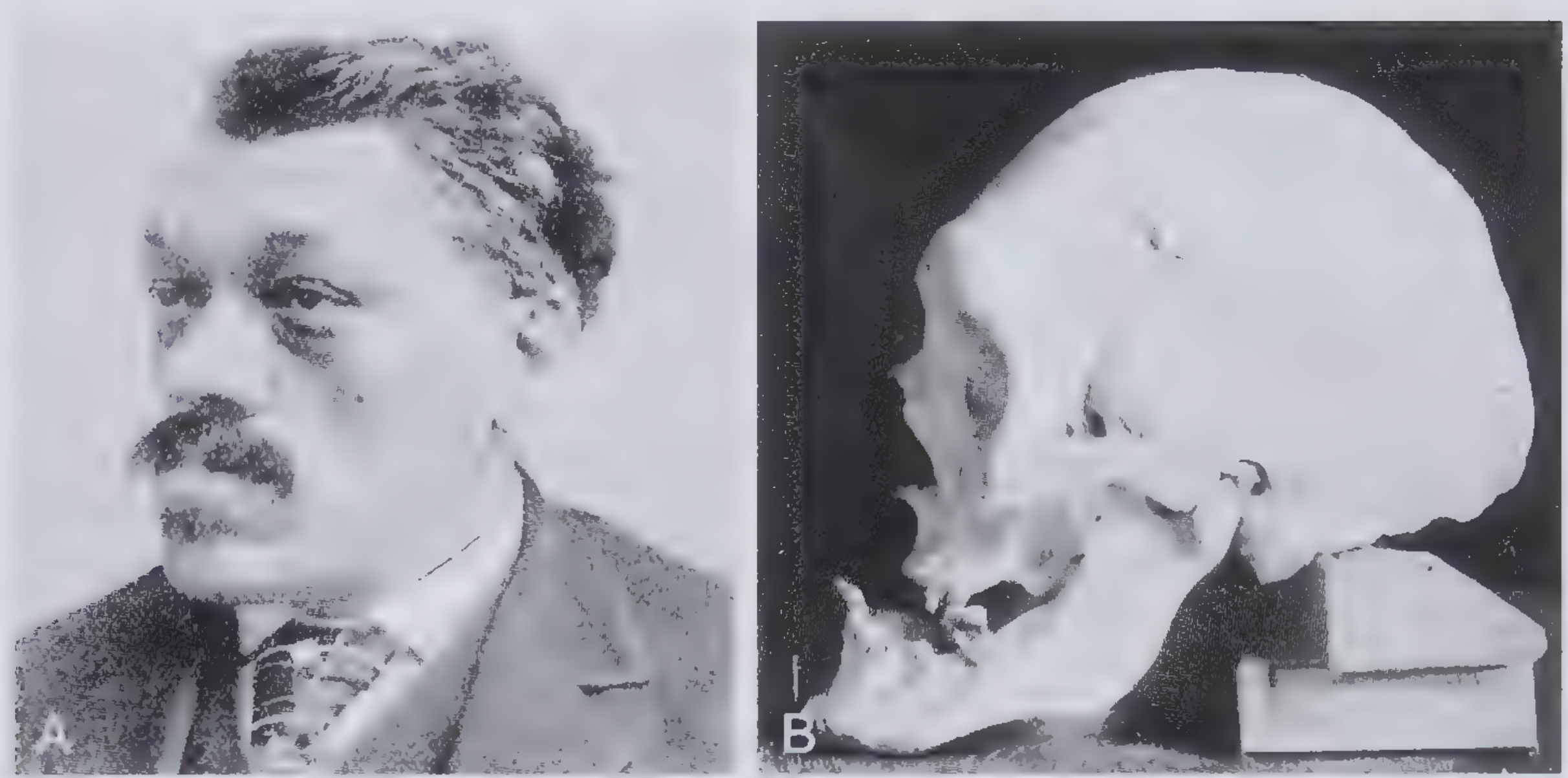
Frameworks for Internal Medicine - Frontal bossing, protruding jaw, and skull changes in acromegaly
Specific Facial Features
| Feature | Mechanism |
|---|---|
| Frontal bossing (prominent supraorbital ridges) | Bony overgrowth of the frontal bone |
| Mandibular prognathism (protruding lower jaw) | Alveolar + mandibular enlargement |
| Macrognathia (widened jaw) | Bony overgrowth of maxilla and mandible |
| Broad/bulbous nose | Nasal bone hypertrophy + soft-tissue thickening |
| Macroglossia (enlarged tongue) | Soft tissue overgrowth |
| Thick lips | Soft tissue hypertrophy |
| Deep nasolabial folds | Skin thickening + doughy texture from glycosaminoglycan deposition |
| Coarse, doughy skin | Dermal glycosaminoglycan and collagen deposition |
| Enlarged paranasal sinuses | Bony expansion |
| Tooth separation / malocclusion | Alveolar enlargement |
| Prominent forehead grooves | Cutis verticis gyrata-like changes; exaggerated skin folds |
| Hyperhidrosis + oily skin | GH effect on sweat glands |
Why "Gorilla Face"?
The combination of prominent brow ridges + prognathic jaw + broad flat nose + thick lips + coarse skin folds produces a resemblance to a gorilla's facial structure - all driven by unchecked periosteal bone growth and soft-tissue hypertrophy from GH/IGF-1 excess.
Andrews' Diseases of the Skin notes that the clinical changes may also suggest the leonine facies (lion face) of leprosy (Hansen's disease), Paget disease, myxedema, and pachydermoperiostosis - important differentials to keep in mind.
Pathophysiology
- Cause: In 98% of cases, a GH-secreting pituitary adenoma (somatotroph adenoma)
- Mediator: IGF-1 (somatomedin C) produced by the liver in response to GH
- Onset: Insidious; mean time to diagnosis is ~8 years
- Diagnosis: IGF-1 level + GH suppression after oral glucose load (failure to suppress = acromegaly) + pituitary MRI
Differentials for "Gorilla/Coarse" Face
- Leonine facies of leprosy
- Myxedema (hypothyroidism)
- Paget disease of bone
- Pachydermoperiostosis
- Acromegaloid facial appearance syndrome (normal GH, hereditary)
- Pseudoacromegaly (severe insulin-resistant diabetes, long-term minoxidil)
Sources: Andrews' Diseases of the Skin; Cummings Otolaryngology Head & Neck Surgery; Goldman-Cecil Medicine; Fitzpatrick's Dermatology; Scott-Brown's Otorhinolaryngology; Brenner & Rector's The Kidney; Frameworks for Internal Medicine
Show me more clear image of gorilla face
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here are the clearest clinical images of the "gorilla face" in acromegaly, directly from authoritative medical textbooks:
Image 1 - Frontal & Lateral View (Fitzpatrick's Dermatology, Fig. 137-16)
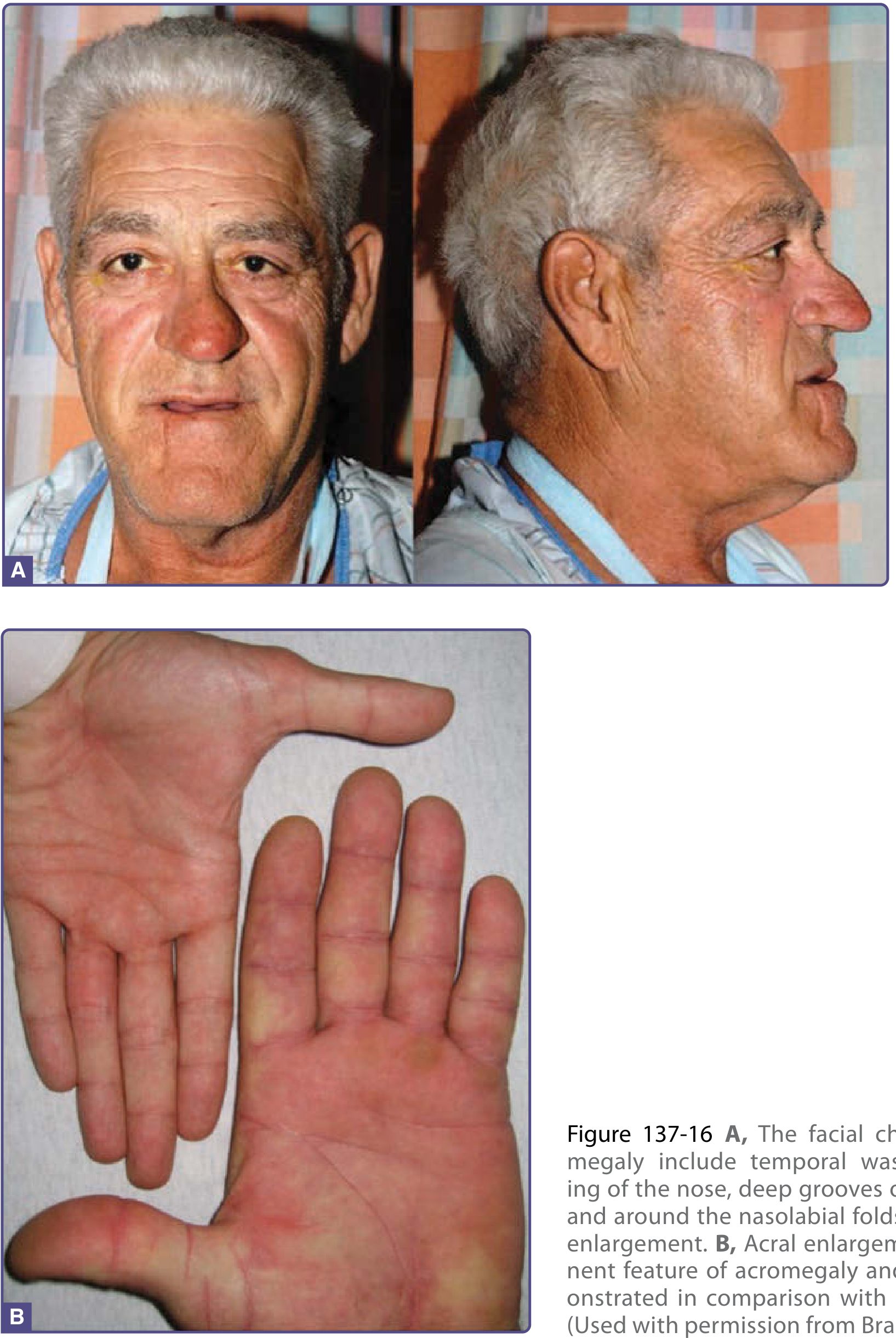
This image shows both frontal and lateral (profile) views - the profile is particularly striking. You can clearly see:
- Temporal wasting (sunken temples)
- Broadened, bulbous nose
- Deep nasolabial folds and forehead grooves
- Prognathic (protruding) jaw - most visible in the lateral view
- Thick lips
- Enlarged, spade-like hand (bottom panel, Panel B) - "doughy" texture with sausage-like fingers
Image 2 - Close-up Frontal View (Comprehensive Clinical Nephrology, Fig. 40.6)
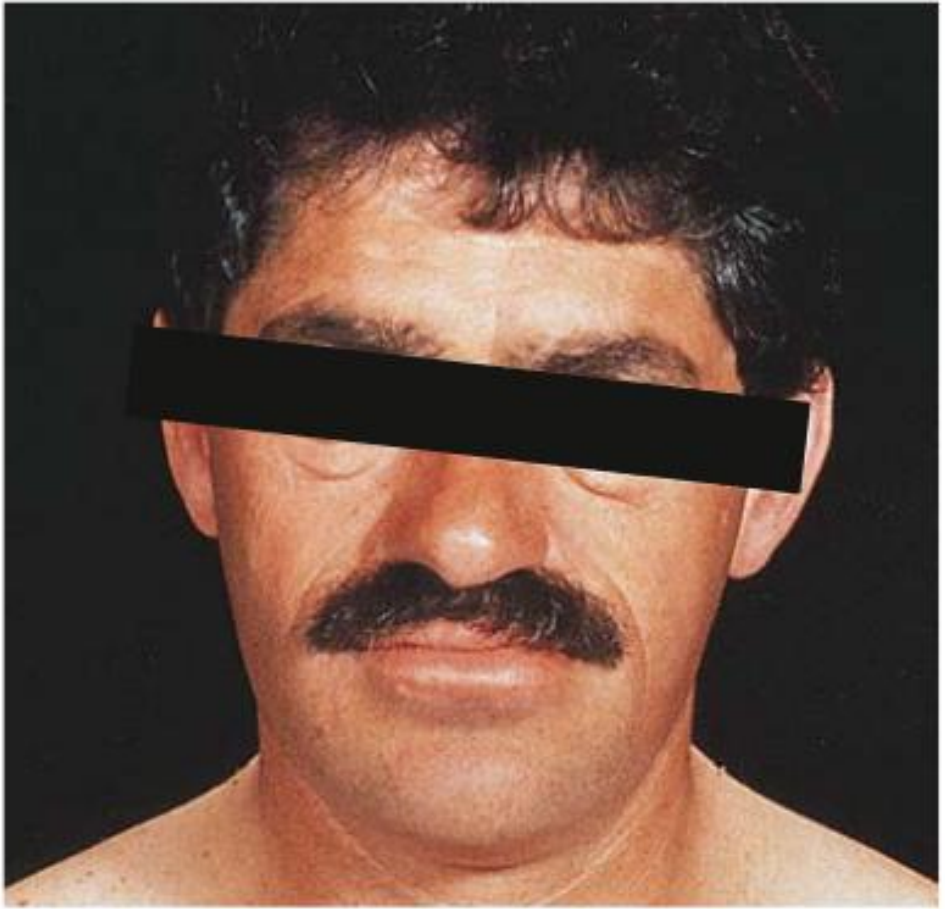
This close-up frontal shot shows:
- Enlarged, prominent brow/supraorbital ridges (frontal bossing)
- Wide, flattened nose with nasal bone hypertrophy
- Widened jaw (macrognathia)
- Thick skin with coarse texture
- Thick lips
Why It Resembles a "Gorilla Face"
The lateral profile in Image 1 is the most visually striking - the combination of a projecting brow ridge + flat broad nose + protruding jaw is the classic ape-like silhouette. This is all bony overgrowth driven by excess GH/IGF-1 acting on periosteal bone, cartilage, and soft tissues over many years.
Sources: Fitzpatrick's Dermatology (Fig. 137-16A,B); Comprehensive Clinical Nephrology, 7th Ed. (Fig. 40.6)
What is the atrophy of adrenal cortex
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer with the key image already fetched.
Atrophy of the Adrenal Cortex
Definition
Adrenal cortical atrophy is the shrinkage and loss of functional cortical tissue of the adrenal gland, leading to adrenocortical insufficiency - inability to produce adequate glucocorticoids, mineralocorticoids, and adrenal androgens.
Gross Pathology Image (Robbins, Fig. 18.31)
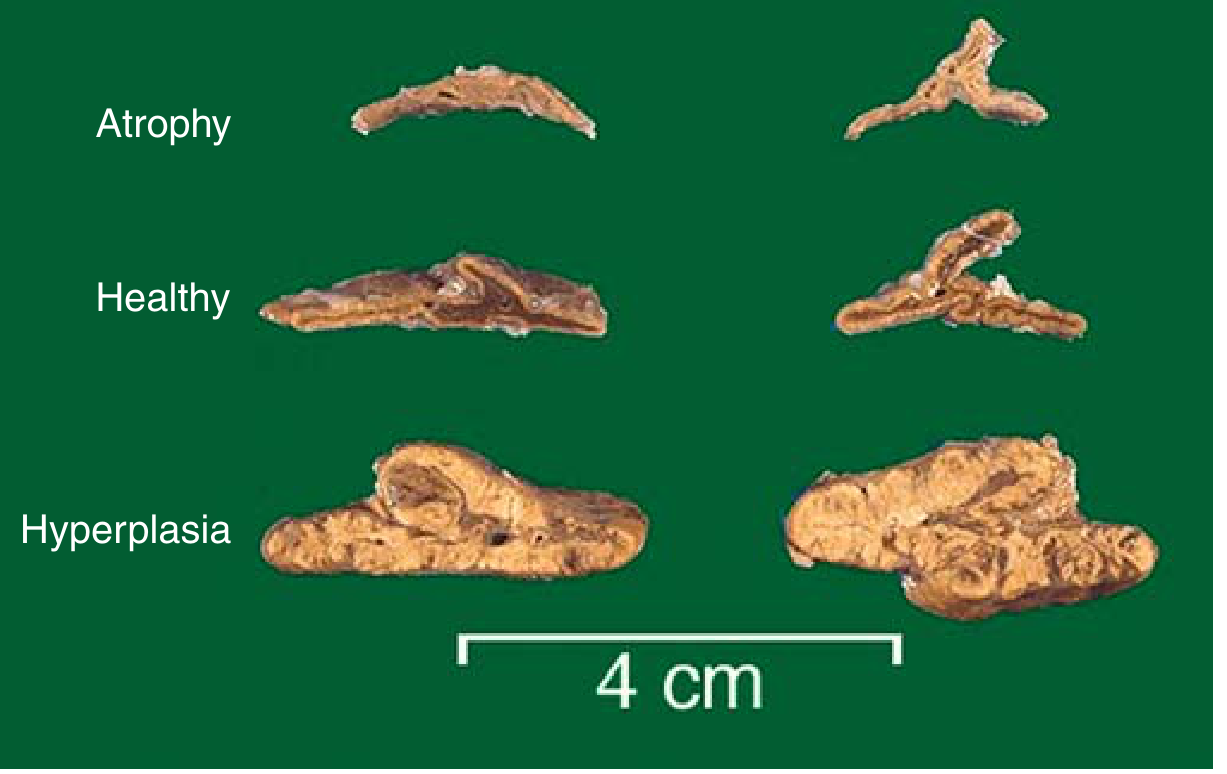
The image shows (scale bar = 4 cm):
- Top row (Atrophy): Markedly shrunken, thin, flattened glands
- Middle row (Healthy): Normal-sized adrenal glands
- Bottom row (Hyperplasia): Enlarged, yellow, nodular glands (ACTH-dependent Cushing syndrome)
The atrophic gland shown was from a patient on prolonged exogenous steroids.
Types of Adrenal Cortical Atrophy
1. Primary (Addison's Disease) - due to direct adrenal destruction
The most common causes (>90% of all cases):
| Cause | Details |
|---|---|
| Autoimmune adrenalitis | 70-90% in developed countries; isolated or part of Autoimmune Polyglandular Syndrome (APS1/APS2) |
| Tuberculosis | Once the #1 cause worldwide; granulomatous destruction; still common in developing countries |
| AIDS-related infections | CMV, Mycobacterium avium-intracellulare, fungal |
| Fungal infections | Histoplasma capsulatum, Coccidioides immitis |
| Metastatic carcinoma | Lung and breast most common; adrenals enlarged (not shrunken) |
2. Secondary (ACTH Deficiency) - the cortex atrophies from lack of trophic stimulation
| Cause | Details |
|---|---|
| Exogenous glucocorticoids | Most common cause in clinical practice - suppresses ACTH via negative feedback |
| Pituitary disease | Tumor, infarction (Sheehan's syndrome), irradiation, infection |
| Hypothalamic disease | Reduced CRH output |
3. Functional atrophy from contralateral tumor
When a unilateral cortisol-secreting adrenal adenoma/carcinoma produces autonomous cortisol, it suppresses ACTH, and the contralateral adrenal cortex undergoes atrophy.
Which Zones are Affected?
| Zone | ACTH-dependent? | Affected by ACTH suppression? |
|---|---|---|
| Zona glomerulosa (mineralocorticoids) | NO | Spared - normal thickness |
| Zona fasciculata (glucocorticoids) | YES | Atrophies |
| Zona reticularis (androgens) | YES | Atrophies |
The zona glomerulosa is regulated by the renin-angiotensin system, not ACTH, so it is the only zone that does NOT atrophy on ACTH deficiency or exogenous steroid use. - Campbell-Walsh Wein Urology
Histological Features (Morphology)
Primary autoimmune adrenalitis:
- Irregularly shrunken glands - may be too small to identify within periadrenal fat
- Scattered residual cortical cells in a collapsed connective tissue network
- Lymphoid infiltrate in the cortex, may extend into medulla
- Medulla is preserved
Secondary / ACTH-deficient atrophy:
- Small, flattened glands retaining yellow color (small residual lipid)
- Thin rim of atrophic yellow cortex surrounding a normal central medulla
- Atrophy predominantly of zona fasciculata and zona reticularis
- Loss of cytoplasmic lipid in cortical cells
Tuberculosis/fungal:
- Adrenal architecture effaced by granulomatous inflammation
Clinical Features of Adrenocortical Insufficiency
Symptoms typically appear only after >90% of the cortex is destroyed:
- Weakness, fatigue (most common early symptom)
- Anorexia, nausea, vomiting, weight loss, diarrhea
- Hyperpigmentation of skin and mucosae (face, axillae, nipples, perineum) - only in PRIMARY insufficiency, due to elevated ACTH/MSH (both derived from POMC)
- Hypotension (aldosterone deficiency - sodium loss, volume depletion)
- Hyperkalemia, hyponatremia (mineralocorticoid deficiency)
- Hypoglycemia (glucocorticoid deficiency - impaired gluconeogenesis)
Secondary insufficiency differs: no hyperpigmentation, aldosterone near-normal, so no hyperkalemia.
Adrenal (Addisonian) Crisis - Acute Emergency
Precipitated by stress (infection, surgery, trauma) in a patient with chronic insufficiency:
- Intractable vomiting, abdominal pain
- Severe hypotension, vascular collapse
- Coma
- Fatal if not treated immediately with IV hydrocortisone
Special form: Waterhouse-Friderichsen Syndrome - bilateral massive adrenal hemorrhage in overwhelming sepsis (classically Neisseria meningitidis), causing acute adrenal insufficiency via cortical destruction.
Sources: Robbins & Kumar Basic Pathology (Figs. 18.31, 18.35); Fitzpatrick's Dermatology; Campbell-Walsh Wein Urology; Tietz Textbook of Laboratory Medicine; Ganong's Review of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.