maternal changes in pregnancy im exam POV with detailed explanation for 5marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have rich, comprehensive data from the textbooks. Let me compile the full exam-oriented answer.
Maternal Changes in Pregnancy - 5 Marks Exam Answer
Introduction
Pregnancy induces extensive physiological changes in virtually every organ system of the mother. These changes are adaptive, designed to meet the increased metabolic demands of the mother and fetus, sustain uteroplacental circulation, and prepare the body for labor and delivery.
1. CARDIOVASCULAR CHANGES
These are among the most significant changes and occur early in the first trimester.
| Parameter | Change |
|---|---|
| Cardiac output | +40% at term |
| Heart rate | +20% |
| Stroke volume | +30% |
| Blood volume | +35% |
| Plasma volume | +55% |
| Systolic BP | -5% |
| Diastolic BP | -15% |
| Peripheral vascular resistance | -15% |
Key points:
- Cardiac output rises due to increases in both heart rate and stroke volume. The greatest rise occurs during labor and immediately after delivery.
- Blood volume increases by 1000-1500 mL by term (total ~90 mL/kg), enabling the mother to tolerate blood loss at delivery (average 200-500 mL vaginally; 800-1000 mL at C-section).
- Plasma volume increases more (55%) than red cell mass (45%) - this produces dilutional (physiological) anemia of pregnancy. Hemoglobin remains >11 g/dL normally.
- Systemic vascular resistance falls from the first trimester (nadir in mid-second trimester) due to progesterone-mediated vasodilation and the low-resistance uteroplacental circuit.
- Aortocaval compression (Supine Hypotension Syndrome): After 20 weeks, the gravid uterus can compress the inferior vena cava in the supine position, reducing venous return and causing hypotension, pallor, sweating, and nausea - seen in ~5% of women. Managed by left lateral tilt (>15 degrees wedge under right hip).
- Electrocardiogram changes: Diaphragm elevation shifts the heart leftward, causing left axis deviation, T-wave changes, and apparent cardiomegaly on chest X-ray.
- Murmurs: A systolic ejection murmur (grade I-II) is heard in most pregnant women due to increased flow across the aortic and pulmonary valves - this is normal. Third and fourth heart sounds may also appear.
2. RESPIRATORY CHANGES
| Parameter | Change |
|---|---|
| Oxygen consumption | +20 to 50% |
| Minute ventilation | +50% |
| Tidal volume | +40% |
| Respiratory rate | +15% |
| PaCO2 | -15% (28-32 mmHg) |
| HCO3 | -15% (compensatory) |
| PaO2 | +10% |
| FRC | -20% |
| Airway resistance | -35% |
Key points:
- Minute ventilation increases 50% (mainly due to tidal volume increase). This is driven by elevated progesterone, which stimulates the respiratory center directly.
- Physiological hyperventilation causes a mild respiratory alkalosis (PaCO2 falls to 28-32 mmHg). This is compensated by renal bicarbonate excretion (HCO3 falls to ~20 mEq/L) - so pH is only mildly elevated.
- The P50 of hemoglobin increases (27 to 30 mmHg) due to elevated 2,3-DPG, facilitating oxygen unloading to fetal tissues.
- FRC decreases 20% at term due to uterine elevation of the diaphragm reducing expiratory reserve volume.
- The combination of decreased FRC + increased O2 consumption means pregnant women desaturate very rapidly during apnea - hence mandatory pre-oxygenation before general anesthesia.
- Upper airway: Mucosal edema, vascular engorgement, and capillary congestion of the respiratory mucosa predisposes to bleeding and obstruction. Smaller endotracheal tubes (6-6.5 mm) should be used.
- The diaphragm rises ~4 cm, but chest anteroposterior diameter increases to compensate. Vital capacity is minimally affected.
3. HEMATOLOGICAL CHANGES
- Dilutional anemia: Plasma volume rises more than RBC mass, causing Hb to fall but remain >11 g/dL.
- Hypercoagulable state: Fibrinogen and Factors VII, VIII, IX, X, XII all increase (+30 to 250%). Factor XI may decrease. This is protective against hemorrhage at delivery but predisposes to DVT.
- Leukocytosis: WBC rises to as high as 21,000/μL in the third trimester (physiological).
- Platelets: Mild decrease (~10%) due to dilution and increased consumption.
- Iron and folate deficiency anemia can develop due to fetal utilization - supplementation is essential.
- Fibrinolysis accelerates late in the third trimester.
4. RENAL CHANGES
| Parameter | Change |
|---|---|
| GFR | +50% |
| Renal plasma flow | Increases |
| Serum creatinine | Decreased (as low as 0.5 mg/dL) |
| BUN | Decreased (as low as 9 mg/dL) |
Key points:
- GFR increases 50% due to increased renal plasma flow and cardiac output. So normal creatinine and BUN values are lower in pregnancy - a creatinine of 1.0 mg/dL (normal in non-pregnant) may indicate renal impairment in a pregnant woman.
- Glycosuria (1-10 g/day) is common and physiological - due to reduced tubular threshold for glucose.
- Mild proteinuria (<300 mg/day) is normal; >300 mg/day raises concern for preeclampsia.
- Plasma osmolality decreases by 8-10 mOsm/kg.
- Hydronephrosis and hydroureter (more common on the right) occur due to uterine compression and progesterone-induced smooth muscle relaxation.
5. GASTROINTESTINAL CHANGES
- Gastric emptying is delayed from early pregnancy. Progesterone relaxes smooth muscle throughout the GI tract.
- Lower esophageal sphincter (LES) tone decreases due to progesterone + mechanical upward displacement of the stomach by the uterus. This causes:
- Gastroesophageal reflux (heartburn - very common)
- High risk of regurgitation and pulmonary aspiration during anesthesia (Mendelson's syndrome)
- Constipation is common due to reduced gut motility.
- Gallstones: Elevated progesterone inhibits cholecystokinin release, causing incomplete gallbladder emptying. Together with altered bile composition, this predisposes to cholesterol gallstone formation.
6. HEPATIC CHANGES
- Overall hepatic function and blood flow are unchanged.
- Mild elevations in serum transaminases and LDH in third trimester.
- Serum alkaline phosphatase elevated - due to placental secretion (not hepatic disease).
- Serum albumin decreases (dilutional) - reduces colloid oncotic pressure and affects drug protein binding.
- Pseudocholinesterase activity decreases 25-30% at term - clinical significance for succinylcholine metabolism is minimal but may prolong action. Does not return to normal until 6 weeks postpartum.
7. CNS CHANGES
- MAC (minimum alveolar concentration) decreases 40% by term for all volatile anesthetic agents - due to elevated progesterone (sedating effect) and β-endorphin surge.
- Sensitivity to local anesthetics increases - neural blockade occurs at reduced concentrations (MLAC reduced ~30% for epidural anesthesia). This is hormonally mediated and also due to epidural venous engorgement.
- Engorged epidural veins reduce epidural space volume, increasing cephalad spread of spinal/epidural blocks.
8. METABOLIC AND ENDOCRINE CHANGES
- Insulin resistance increases (diabetogenic state) due to placental secretion of human placental lactogen (hPL/human chorionic somatomammotropin). Insulin levels rise progressively. Pancreatic beta cells undergo hyperplasia.
- Gestational diabetes mellitus (GDM) can occur in susceptible women.
- Thyroid: Thyroid gland hypertrophies; thyroid-binding globulin increases (due to hCG and estrogens), so total T3 and T4 levels rise, but free T3 and T4 remain normal - pregnancy is a euthyroid state.
- Calcium metabolism: Parathyroid hormone and 1,25-dihydroxyvitamin D3 increase to support fetal skeletal development.
- Adrenal changes: Cortisol levels rise with elevated corticosteroid-binding globulin.
9. SKIN AND MUSCULOSKELETAL CHANGES
- Pigmentation increases (chloasma/melasma - "mask of pregnancy," linea nigra) due to elevated MSH and estrogens.
- Striae gravidarum - stretch marks on abdomen, breasts, thighs due to skin stretching and cortisol effects on collagen.
- Spider angiomas and palmar erythema - due to elevated estrogens causing vascular dilation.
- Edema is common, especially in the lower limbs (venous stasis from IVC compression).
- Relaxin hormone loosens ligaments, especially in the pelvis (pubic symphysis, sacroiliac joints) to facilitate delivery. Can cause lower back pain and gait changes.
Quick Summary Table for Exam
| System | Key Change | Clinical Significance |
|---|---|---|
| CVS | CO +40%, BV +35%, SVR falls | Physiological anemia, supine hypotension |
| Respiratory | MV +50%, FRC -20%, PaCO2 falls | Rapid desaturation, alkalosis |
| Haematology | Hypercoagulable, dilutional anemia | DVT risk, Hb >11 g/dL normal |
| Renal | GFR +50%, creatinine falls | Glycosuria/proteinuria normal |
| GIT | LES tone falls, gastric emptying delayed | Aspiration risk in GA |
| Hepatic | Albumin falls, Alk.Phos. rises | Altered drug binding |
| CNS | MAC -40%, LA sensitivity up | Reduced anesthetic needs |
| Metabolic | Insulin resistance, euthyroid | GDM risk |
Sources: Morgan and Mikhail's Clinical Anesthesiology, 7e; Guyton and Hall Textbook of Medical Physiology
Enumerate the indications and types of vaccination during pregnancy. in exam Point of view with detailed explanation
Finding Sources
Finding Sources
Searching the Web
vaccines recommended during pregnancy indications types 2024 guidelines
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive, current data from Harrison's 2025, Red Book 2021, and CDC guidelines. Let me compile the full exam answer.
Vaccination During Pregnancy - Indications and Types (5 Marks Exam Answer)
Introduction
Vaccination during pregnancy serves a dual purpose: it protects the mother from vaccine-preventable diseases and provides passive immunity to the neonate via transplacental IgG transfer. Neonates are most vulnerable in the first few weeks of life before their own immunization schedule begins - hence maternal immunization is a critical bridge.
The basic principle governing vaccines in pregnancy is:
- Inactivated vaccines / toxoids / subunit vaccines = generally SAFE
- Live attenuated vaccines = generally CONTRAINDICATED (risk of fetal infection)
CLASSIFICATION OF VACCINES IN PREGNANCY
A. ROUTINELY RECOMMENDED DURING EVERY PREGNANCY
1. Tdap (Tetanus, Diphtheria, Acellular Pertussis)
Type: Inactivated toxoid + acellular subunit
Timing: 27 to 36 weeks of gestation (preferably early in this window)
Given in EVERY pregnancy, regardless of prior Tdap history.
Indication and rationale:
- Neonatal/infant pertussis (whooping cough) is a major killer in the first 2 months of life - before the infant can be vaccinated.
- Administering Tdap at 27-36 weeks maximizes the transplacental transfer of maternal IgG antibodies to the fetus before delivery.
- The earlier in the 27-36 week window, the more antibody reaches the neonate.
- If not given during pregnancy, Tdap should be administered immediately postpartum (to at least protect via cocooning strategy).
- Household contacts and caregivers of newborns who have not previously received Tdap should also be vaccinated ("cocoon strategy").
Key fact for exam: Tdap should be repeated in EVERY subsequent pregnancy - not just once in a lifetime.
2. Inactivated Influenza Vaccine (IIV) / Recombinant Influenza Vaccine (RIV)
Type: Inactivated / recombinant subunit
Timing: Any trimester; ideally September-October each year. Third trimester vaccination can be considered in July-August if available.
Indication and rationale:
- Pregnant women are at high risk of severe influenza complications (pneumonia, hospitalization, preterm labor) due to physiological immunosuppression, altered cell-mediated immunity, and pulmonary changes.
- Maternal IgG crosses the placenta and protects the newborn for the first 6 months (until the infant can be vaccinated).
- Live attenuated influenza vaccine (LAIV) is given intranasally and is CONTRAINDICATED in pregnancy.
- Only inactivated or recombinant influenza vaccines are safe.
3. COVID-19 Vaccine
Type: mRNA (Pfizer-BioNTech, Moderna) or protein subunit - inactivated platforms
Timing: Any trimester; staying up to date with updated boosters recommended.
Indication and rationale:
- Pregnant women are at significantly increased risk of severe COVID-19 including ICU admission, mechanical ventilation, preterm birth, and maternal death.
- mRNA vaccines have been confirmed safe in pregnancy through large real-world data (no increased risk of miscarriage, preterm birth, or congenital anomalies).
- Maternal IgG is transferred to the neonate.
- ACOG, CDC, WHO, and AAP all recommend COVID-19 vaccination during pregnancy.
4. RSV (Respiratory Syncytial Virus) Vaccine - Abrysvo (Pfizer)
Type: Bivalent recombinant protein subunit
Timing: 32 to 36 weeks of gestation (during September to January, i.e., RSV season)
Indication and rationale:
- RSV is the leading cause of bronchiolitis and lower respiratory tract disease in infants under 6 months.
- Maternal vaccination transfers RSV-specific IgG to the fetus, protecting the neonate in the first months of life.
- Alternative approach: infant administration of nirsevimab (a long-acting monoclonal antibody) at birth - used when maternal vaccination was not given.
- Timing is restricted to the RSV season window to optimize protection during the infant's most vulnerable period.
B. RECOMMENDED FOR SPECIFIC INDICATIONS (Not All Pregnancies)
5. Hepatitis B Vaccine (HepB)
Type: Recombinant subunit (HBsAg)
Indication: Recommended if the pregnant woman has not previously been vaccinated (universal adult vaccination is now recommended for ages 19-59 years).
Rationale:
- Prevents mother-to-child transmission of HBV.
- HBV infection during pregnancy increases risk of preterm birth, low birth weight, and vertical transmission to the neonate (especially during delivery).
- Safe in all trimesters.
6. Hepatitis A Vaccine (HepA)
Type: Inactivated
Indication: Recommended if pregnant and at risk for HAV infection or severe outcome, and not previously vaccinated.
Risk groups include: travelers to endemic areas, those with chronic liver disease, IV drug users, household contacts of infected persons.
7. Meningococcal Vaccines (MenACWY, MenB)
Type: Conjugate (MenACWY) / Protein subunit (MenB)
Indication: May be used if otherwise indicated (e.g., asplenia, complement deficiency, travel to endemic areas, college outbreaks).
- MenACWY: May be given if indicated.
- MenB: Pregnancy is a precaution; administered only if benefit outweighs risk.
8. Pneumococcal Vaccine (PCV/PPSV23)
Type: Conjugate / polysaccharide
Indication: Generally no recommendation for routine use in pregnancy. May be used if the woman has a high-risk condition (asplenia, chronic disease) and was not previously vaccinated.
9. Travel Vaccines (Situation-specific)
| Vaccine | Status in Pregnancy |
|---|---|
| Cholera | No data - use if benefit outweighs risk |
| Japanese Encephalitis | No data - use if benefit outweighs risk |
| Typhoid (inactivated IM) | May be used if risk is high |
| Typhoid (oral live) | Contraindicated |
| Rabies (post-exposure) | No contraindication; PEP should never be withheld |
| Yellow Fever (live) | Use only if travel is unavoidable and risk is high; weigh carefully |
C. CONTRAINDICATED VACCINES IN PREGNANCY
These are live attenuated vaccines - contraindicated because of the theoretical risk of vaccine virus replication causing congenital infection or adverse fetal effects.
| Vaccine | Reason |
|---|---|
| MMR (Measles-Mumps-Rubella) | Live virus; risk of congenital rubella syndrome if rubella virus replicates |
| Varicella (Varivax) | Live virus; risk of congenital varicella syndrome |
| MMRV (combined) | Live; same as above |
| Live Attenuated Influenza (LAIV - nasal) | Live virus; contraindicated |
| HPV Vaccine (Gardasil 9) | Not recommended; delay until after pregnancy (no evidence of harm but insufficient data) |
| Recombinant Zoster (Shingrix) | No recommendation; consider delaying until after pregnancy |
| Oral Typhoid | Live virus; contraindicated |
| Yellow Fever | Live; only if absolutely unavoidable due to travel |
| Adenovirus | Contraindicated |
Management: Women who receive MMR or varicella inadvertently in early pregnancy should be counseled - but termination is NOT recommended as no cases of congenital rubella or varicella syndrome have been confirmed from vaccine strains.
Rubella and varicella seronegative women should receive MMR and varicella vaccines immediately postpartum before discharge from hospital.
D. POSTPARTUM VACCINATION (Catch-up)
Women who missed vaccines during pregnancy should receive them in the immediate postpartum period:
- Tdap - if not given during pregnancy, give immediately postpartum
- MMR - if seronegative for rubella/measles; give postpartum
- Varicella - if seronegative; give postpartum
- Influenza - if non-immunized breastfeeding women
- All vaccines can be given while breastfeeding (safe), except yellow fever (precaution - avoid or temporarily suspend breastfeeding for 2 weeks)
Summary Table for Exam
| Category | Vaccine | Timing | Given Every Pregnancy? |
|---|---|---|---|
| Routinely Recommended | Tdap | 27-36 weeks (early) | YES |
| Inactivated Influenza | Any trimester | YES (seasonal) | |
| COVID-19 (mRNA/subunit) | Any trimester | YES (stay up to date) | |
| RSV vaccine (Abrysvo) | 32-36 weeks (Sept-Jan) | YES (if in season) | |
| Specific Indications | Hepatitis B | Any trimester | If not vaccinated |
| Hepatitis A | Any trimester | If at risk | |
| Meningococcal | Any trimester | If indicated | |
| CONTRAINDICATED | MMR, Varicella, LAIV | - | Give postpartum |
| HPV, Yellow Fever, Oral Typhoid | - | Delay/avoid |
Key Mnemonics for Exam
"TIC-R" = Routinely recommended in pregnancy:
- T - Tdap (27-36 weeks)
- I - Influenza (any trimester, inactivated only)
- C - COVID-19 (any trimester)
- R - RSV (32-36 weeks)
"MVVH" = Contraindicated (Live vaccines):
- M - MMR
- V - Varicella
- V - Varivax (combined MMRV)
- H - (HPV - not recommended, delay)
Sources: Harrison's Principles of Internal Medicine 22E (2025); Red Book 2021 - Committee on Infectious Diseases (AAP); CDC Guidelines for Vaccinating Pregnant Women (2024); ACOG Maternal Immunization Schedule
Development of placenta with detailed explanation in exam Pov
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content and diagrams needed. Here is the complete, exam-oriented answer:
Development of Placenta - Detailed Exam Answer
Introduction
The placenta is a fetomaternal organ - it has two components:
- Fetal part - derived from the chorionic sac (chorion frondosum)
- Maternal part - derived from the endometrium (decidua basalis)
It forms the transport system for gases, nutrients, and waste between mother and fetus. By the end of Week 3, the structural basis for physiological exchange is already established; by Week 4, a complex vascular network is functional.
STEP 1: IMPLANTATION AND TROPHOBLAST DIFFERENTIATION (Days 6-9)
After fertilization, the blastocyst reaches the uterine cavity by Day 4-5 and begins implantation around Day 6-7, typically on the posterior wall of the upper uterine body.
The trophoblast (outer layer of the blastocyst) differentiates into two layers:
| Layer | Structure | Function |
|---|---|---|
| Cytotrophoblast (CTB) | Inner layer - distinct cell boundaries, mitotically active | Proliferates to supply cells to syncytiotrophoblast |
| Syncytiotrophoblast (STB) | Outer layer - multinucleated, no cell boundaries | Invasive; erodes maternal tissues and decidua |
The syncytiotrophoblast aggressively invades the decidua, eroding maternal capillaries and glands. By Days 8-9, fluid-filled spaces called lacunae develop within the syncytiotrophoblast. These lacunae are the forerunners of the intervillous space.
STEP 2: DECIDUAL REACTION (Week 2)
The uterine endometrium in a pregnant woman is called the decidua. In response to rising progesterone, endometrial stromal cells enlarge, filling with glycogen and lipid to form decidual cells - this transformation is the decidual reaction.
The decidua is divided into three regions based on their relation to the implantation site:
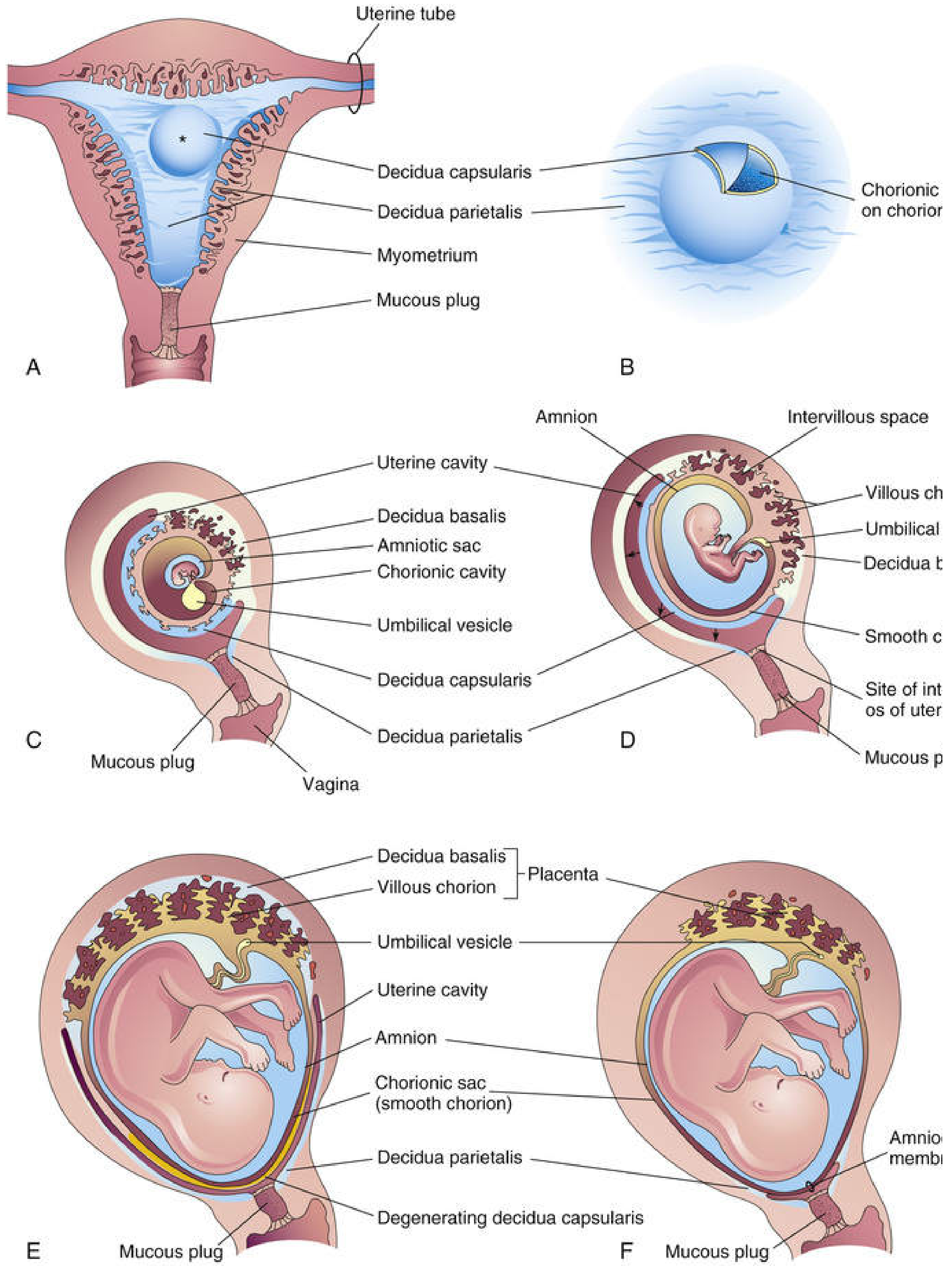
Development of the placenta and decidua at various gestational ages (The Developing Human)
| Region | Location | Fate |
|---|---|---|
| Decidua basalis | Deep to the implanted conceptus | Forms the maternal part of the placenta |
| Decidua capsularis | Superficial, overlying the conceptus | Degenerates by Week 22 as the fetus grows |
| Decidua parietalis | All remaining endometrium | Fuses with decidua capsularis by Month 3 - obliterates uterine cavity |
STEP 3: FORMATION OF CHORIONIC VILLI (Weeks 2-3)
This is the most important and most examined part of placental development. Chorionic villi develop in three sequential stages:
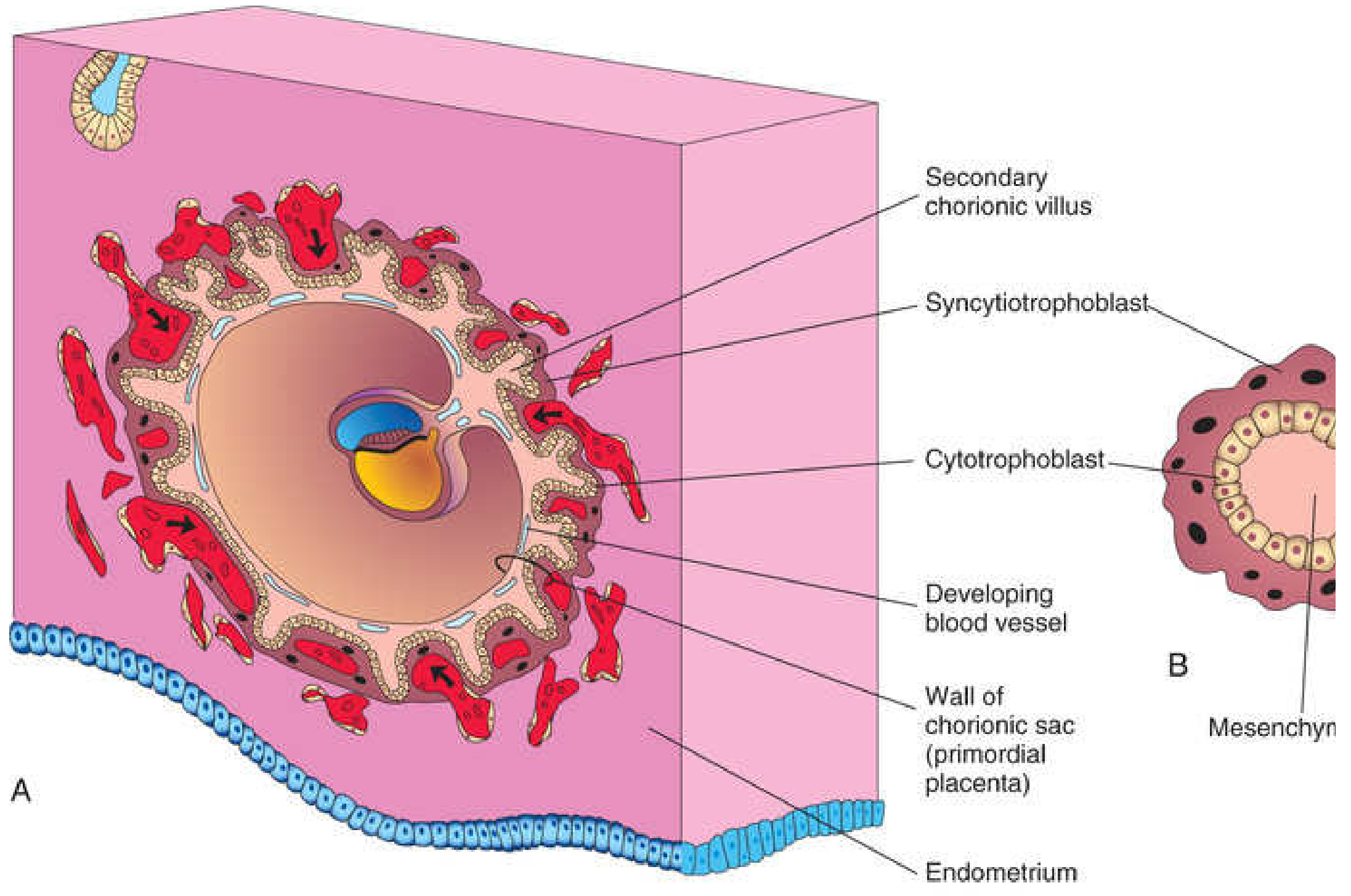
Secondary chorionic villus formation (The Developing Human, Moore & Persaud)
Stage 1: Primary Chorionic Villi (End of Week 2)
- Cytotrophoblastic cells proliferate and invade the syncytiotrophoblast, forming finger-like projections - the primary chorionic villi.
- Structure: Core of cytotrophoblast covered by syncytiotrophoblast.
- At this stage, villi are solid cellular projections with no mesenchyme or blood vessels.
Stage 2: Secondary Chorionic Villi (Early Week 3)
- Extraembryonic mesoderm (from the extraembryonic coelom) invades the primary villi.
- This forms a central mesenchymal core inside each villus.
- Structure: Syncytiotrophoblast → Cytotrophoblast → Mesenchyme (centre)
- At this stage, villi cover the entire chorionic sac surface.
Stage 3: Tertiary Chorionic Villi (End of Week 3)
- Mesenchymal cells within the secondary villi differentiate into capillaries and blood cells (vasculogenesis).
- When blood vessels are visible within the villi = tertiary chorionic villi.
- The fetal capillary network connects with the embryonic heart via vessels in the connecting stalk.
- By end of Week 3, embryonic blood begins to flow through the villi.
- Gaseous exchange begins: O2 and nutrients diffuse from maternal blood in the lacunae → through villus walls → into fetal blood.
STEP 4: FORMATION OF THE INTERVILLOUS SPACE
- Maternal spiral arteries are eroded by the invasive syncytiotrophoblast.
- By Days 12-15, syncytiotrophoblast penetrates the endothelial lining of small spiral arteries - creating direct communication between lacunae and maternal blood vessels.
- The multiple lacunae merge into one large intercommunicating space = the intervillous space.
- Maternal blood (from ~120 spiral arteries) enters the intervillous space in pulsatile spurts and bathes the chorionic villi directly.
- The fetal villi project into this space "like a forest of trees" arising from the chorionic plate (analogous to soil).
STEP 5: DIFFERENTIATION INTO CHORION FRONDOSUM AND CHORION LAEVE (Week 8 onwards)
- Initially, chorionic villi cover the entire chorionic sac.
- As the chorionic sac grows:
- Villi associated with decidua capsularis get compressed, lose their blood supply, and degenerate → forming the smooth, bare chorion laeve (smooth chorion)
- Villi associated with decidua basalis become larger, branch profusely, and proliferate → forming the chorion frondosum (villous/bushy chorion)
| Region | Name | Fate |
|---|---|---|
| Villi over decidua basalis | Chorion frondosum | Becomes the fetal part of the placenta |
| Villi over decidua capsularis | Chorion laeve | Degenerates; becomes smooth chorion |
The placenta = Chorion frondosum (fetal) + Decidua basalis (maternal)
STEP 6: MATURE PLACENTA STRUCTURE
Gross Anatomy (at term)
- Disc-shaped organ, ~15-20 cm diameter, ~2-3 cm thick, weighs ~500 g
- Fetal surface (chorionic plate): smooth, covered by amnion, umbilical cord attaches (usually centrally)
- Maternal surface (basal plate): rough, cotyledons visible (15-30 irregular lobes separated by decidual septa)
Cotyledons
- The maternal surface is divided into 15-30 cotyledons by decidual septa projecting from the decidua basalis.
- Each cotyledon contains 1-4 main stem villi (anchoring villi) and their branches.
- Each cotyledon is a functional vascular unit.
Types of Villi
| Type | Attachment | Function |
|---|---|---|
| Stem villi (Anchoring villi) | Attach to the cytotrophoblastic shell on the maternal side | Structural support |
| Branch villi (Free villi) | Float freely in the intervillous space | Main site of feto-maternal exchange |
STEP 7: THE PLACENTAL BARRIER (Hemochorial Placenta)
The human placenta is hemochorial - meaning maternal blood is in direct contact with the chorionic villi (no maternal endothelium or connective tissue intervenes).
Layers separating fetal blood from maternal blood in early pregnancy (4 layers):
- Syncytiotrophoblast (with brush border microvilli facing maternal blood)
- Cytotrophoblast
- Connective tissue / mesenchyme of villus
- Fetal capillary endothelium
In late pregnancy, the cytotrophoblast layer becomes discontinuous (thins out), leaving effectively 3 layers and reducing the diffusion distance, increasing efficiency of exchange.
The syncytiotrophoblast forms the brush border with abundant microvilli facing maternal blood, maximizing surface area for exchange.
STEP 8: PLACENTAL CIRCULATION
Fetal Circulation
- Umbilical arteries (2) carry deoxygenated blood from fetus to placenta
- Blood passes through fetal capillaries in the chorionic villi
- Umbilical vein (1) carries oxygenated blood back to the fetus
Maternal Circulation
- ~120 spiral arteries open into the intervillous space
- Blood enters under arterial pressure, rises toward the chorionic plate, then percolates around the villi
- Drains back through endometrial veins
- Fetal and maternal circulations are SEPARATE - do not normally mix
STEP 9: PLACENTAL HOMEOBOX GENE REGULATION
- Homeobox genes (HLX, MSX2, DLX3) expressed in the trophoblast and its blood vessels induce trophoblastic invasion and regulate placental development - relevant for understanding abnormal placentation (placenta accreta, preeclampsia).
TIMELINE SUMMARY TABLE
| Time | Event |
|---|---|
| Day 6-7 | Blastocyst implantation begins |
| Day 8-9 | Lacunae appear in syncytiotrophoblast |
| Day 12-15 | Lacunae connect with spiral arteries; primary chorionic villi form |
| Week 3 (early) | Secondary chorionic villi (mesenchyme invades) |
| Week 3 (late) | Tertiary chorionic villi (capillaries form); fetal circulation begins |
| Week 8 | Differentiation into chorion frondosum and chorion laeve begins |
| Week 10 | Decidua capsularis starts to degenerate |
| Week 12 (~Month 3) | Decidua capsularis fuses with decidua parietalis; uterine cavity obliterated |
| Term (40 weeks) | Mature placenta: disc-shaped, ~500 g, 15-30 cotyledons |
CLINICAL CORRELATES (High-yield for exams)
| Condition | Mechanism |
|---|---|
| Placenta previa | Blastocyst implants in lower uterine segment instead of upper posterior wall |
| Placenta accreta/increta/percreta | Defective decidua basalis - trophoblast invades beyond normal depth into myometrium/serosa |
| Hydatidiform mole | Abnormal trophoblast proliferation; most are 46,XX (complete mole) or triploid (partial mole) |
| Ectopic pregnancy | Implantation outside uterus (usually ampulla of uterine tube) |
| Preeclampsia | Inadequate trophoblastic invasion of spiral arteries → poor uteroplacental blood flow |
| Circumvallate placenta | Chorion laeve fails to degenerate; chorionic plate smaller than basal plate |
Key Mnemonic
"Primary → Secondary → Tertiary" = "P-S-T" = "Plain - Stroma - Tubes"
- Primary = cytotrophoblast core only (no mesenchyme)
- Secondary = Stroma (mesenchyme) invades
- Tertiary = Tubes (blood vessels/capillaries) appear inside
Sources: The Developing Human: Clinically Oriented Embryology (Moore, Persaud & Torchia); Medical Physiology (Boron & Boulpaep); Histology: A Text and Atlas (Ross & Pawlina); Junqueira's Basic Histology 17e
This is a shared conversation. Sign in to Orris to start your own chat.