What's are the standard test for diagnosis of maleria
Reading File
Finding Sources
Searching the Web
standard tests diagnosis malaria WHO 2024
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of the standard tests used to diagnose malaria:
Standard Tests for Diagnosis of Malaria
Key principle: Malaria is NOT a clinical diagnosis. All fever cases in or returning from a malaria-endemic area must be confirmed by a laboratory test. - Harrison's Principles of Internal Medicine, 22E
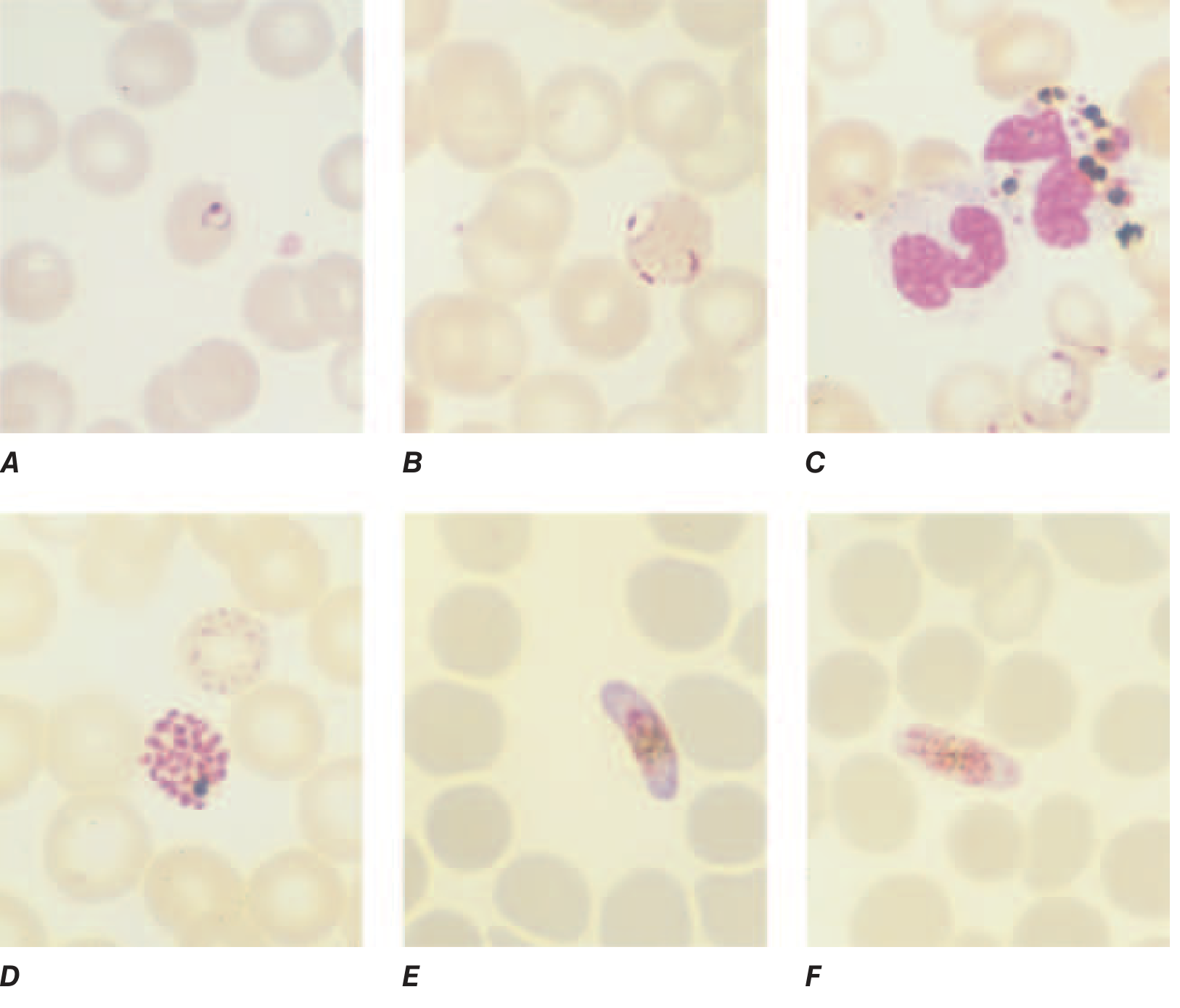
1. Blood Smear Microscopy (Gold Standard)
This is the definitive diagnostic method. Both thick and thin blood smears are prepared from a finger-prick sample and stained with Giemsa stain at pH 7.2 (preferred). Field's, Wright's, or Leishman's stain can also be used.
Thin Blood Smear
- Air-dried, fixed in anhydrous methanol, then stained
- Examined under oil immersion (x1000 magnification)
- Used to identify the Plasmodium species (P. falciparum, P. vivax, P. malariae, P. ovale, P. knowlesi) and determine parasitemia (number of parasitized RBCs per 1000 RBCs)
Thick Blood Smear
- NOT fixed before staining (RBCs lyse during staining)
- Concentrates parasites 40-100x compared to a thin smear - much higher sensitivity for detecting low-density infections
- Parasites and WBCs are counted together; parasitemia is then calculated
- A minimum of 200 WBCs must be counted under oil immersion before calling a smear negative
- 100-200 fields must be examined before declaring a thick smear negative
Prognostic indicators on smear:
- >10^5 parasites/μL = increased risk of death
- >20% of parasites with visible pigment = poor prognosis in severe malaria
- Phagocytosed malarial pigment in >5% of neutrophils = recent schizogony, poor prognosis
2. Rapid Diagnostic Tests (RDTs)
RDTs detect malaria parasite antigens in a finger-prick blood sample using antibody-based stick or card tests. They are the main method in endemic areas when reliable microscopy is not available.
Antigens detected:
| Antigen | Specificity |
|---|---|
| PfHRP2 (Histidine-Rich Protein 2) | P. falciparum-specific |
| Plasmodium LDH (pLDH) | Pan-malaria or species-specific |
| Aldolase | Pan-malaria |
Types:
- Monovalent RDT - detects only P. falciparum
- Bivalent RDT - carries a second antibody (pan-malaria or P. vivax-specific), distinguishing falciparum from non-falciparum malaria
Important caveats:
- PfHRP2-based RDTs can remain positive for several weeks after treatment (helpful in severe malaria after drug clearance, but misleading in high-transmission areas)
- RDTs cannot quantify parasitemia - a key limitation
- PfHRP2/3 gene deletions in some P. falciparum strains (especially in the Horn of Africa) cause false-negative results with PfHRP2-based RDTs - a growing problem
3. Molecular Diagnosis - PCR
- More sensitive than both microscopy and RDTs
- Accurately defines malaria species, including mixed infections
- Detects submicroscopic parasitemia
- Used in reference centers for confirmation, species typing, drug resistance genotyping, and epidemiological studies
- NOT used for primary diagnosis in endemic settings due to cost, infrastructure needs, and time required
4. Fluorescence Microscopy (Acridine Orange Staining)
- Staining parasites with the fluorescent dye acridine orange allows rapid diagnosis in patients with low-level parasitemia
- Limitation: does not allow speciation - cannot identify which Plasmodium species is present
- Used in field settings where it is faster than conventional Giemsa microscopy
5. Serology (Antibody Tests)
- Detects antibodies against malaria rather than the parasite itself
- Not useful for diagnosing acute infection (antibodies appear late and persist long after infection)
- Used mainly for epidemiological surveys and blood donor screening
- Has no role in clinical diagnosis of acute malaria
Summary Table
| Test | Sensitivity | Speciation | Quantifies Parasitemia | Best Use |
|---|---|---|---|---|
| Thick blood smear | High | No | Yes | Initial detection |
| Thin blood smear | Moderate | Yes | Yes | Species ID + parasitemia |
| RDT (PfHRP2) | High for Pf | Partial | No | Rapid field diagnosis |
| PCR | Highest | Yes | Yes | Reference labs, confirmation |
| Acridine orange | High | No | No | Low-resource rapid screening |
| Serology | - | No | No | Epidemiology only |
Clinical Approach (per WHO/National Guidelines)
- Where microscopy result is available within 24 hours: Treat based on species identified on smear (P. falciparum vs P. vivax)
- Where microscopy is unavailable and monovalent RDT is used: Treat based on RDT result; if positive, presume P. falciparum
- Where bivalent RDT is used: Distinguishes falciparum from vivax, guides appropriate drug choice (ACT vs chloroquine + primaquine)
Any positive test - whether RDT or microscopy - warrants prompt treatment. Delay in diagnosis and treatment is a leading cause of death in malaria patients.
Sources: Harrison's Principles of Internal Medicine 22E (2025), Park's Textbook of Preventive and Social Medicine, CDC Malaria Diagnostic Testing
What's are the standard test for diagnosis of maleria
I already covered this in detail in my previous response! Here's a quick recap of the standard malaria diagnostic tests:
Standard Tests for Malaria Diagnosis
1. Blood Smear Microscopy (Gold Standard)
- Thick smear - higher sensitivity, concentrates parasites 40-100x, used for detection
- Thin smear - used for species identification and parasitemia quantification
- Stained with Giemsa stain (preferred), or Wright's/Leishman's/Field's stain
- Must examine 100-200 fields before calling a smear negative
2. Rapid Diagnostic Tests (RDTs)
- Detect parasite antigens (PfHRP2, pLDH, aldolase) from a finger-prick sample
- Monovalent - detects P. falciparum only
- Bivalent - distinguishes P. falciparum from P. vivax
- Cannot quantify parasitemia; PfHRP2 tests may miss strains with gene deletions
3. PCR (Molecular Diagnosis)
- Most sensitive and specific
- Identifies all species and mixed infections
- Used in reference labs only - not for routine field diagnosis
4. Acridine Orange Fluorescence Microscopy
- Rapid, good for low-density parasitemia
- Cannot speciate the parasite
5. Serology (Antibody Tests)
- Detects past infection, not active disease
- Used for epidemiology and blood bank screening only - no role in acute diagnosis
Key rule: Malaria is never a clinical diagnosis alone - always confirm with a lab test. Scroll up to see the full detailed breakdown with images and treatment flow charts.
Diagnostic test for anemia
Finding Sources
Searching the Web
standard diagnostic tests anemia workup CBC iron studies 2024
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from Harrison's and other authoritative sources. Here is the full, detailed answer:
Diagnostic Tests for Anemia
Anemia is defined as hemoglobin below normal for a given population. The WHO thresholds are: <13 g/dL in men, <12 g/dL in non-pregnant women, <11 g/dL in pregnant women.
The diagnostic approach follows a structured, stepwise process.
Step 1: Complete Blood Count (CBC) - First-Line Test
The CBC is the foundation of anemia diagnosis. Key parameters:
Red Cell Indices (Table 66-1, Harrison's 22E)
| Index | Formula | Normal Range | Use |
|---|---|---|---|
| Hemoglobin (Hgb) | Direct measure | M: 13.5-17.5 g/dL; F: 12-16 g/dL | Confirms anemia |
| Hematocrit (Hct) | RBC × MCV / 10 | M: 41-53%; F: 36-46% | Confirms anemia |
| MCV | Hct / RBC count × 10 | 85-95 fL | Classifies anemia by cell size |
| MCH | Hgb / RBC count × 10 | 28.5-32.3 pg | Varies with MCV |
| MCHC | Hgb / Hct × 100 | 33.8-34.2 g/dL | Limited additional value |
| RDW | Range of cell sizes | 11.5-14.5% | Elevated = anisocytosis (varied cell sizes) |
| Platelet count | Direct count | 150,000-400,000/μL | Pancytopenia check |
MCV-Based Classification (Most Practical Approach)
| Type | MCV | Common Causes |
|---|---|---|
| Microcytic | < 80 fL | Iron deficiency, thalassemia, anemia of chronic disease, sideroblastic anemia |
| Normocytic | 80-100 fL | Acute blood loss, hemolytic anemia, anemia of chronic disease, aplastic anemia, renal disease |
| Macrocytic | > 100 fL | B12/folate deficiency, hypothyroidism, liver disease, drugs (hydroxyurea, methotrexate) |
Step 2: Peripheral Blood Smear - Mandatory for All Anemias
Directly visualizing red cell morphology is one of the most informative steps in anemia workup.
| Morphology Found | Pathophysiology | Disease Associations |
|---|---|---|
| Microcytes / Hypochromia | Hemoglobin deficiency | Iron deficiency, thalassemia, sideroblastic anemia |
| Macro-ovalocytes | Nuclear-cytoplasmic dyssynchrony | B12/folate deficiency |
| Spherocytes | Loss of red cell membrane | Hereditary spherocytosis, autoimmune hemolytic anemia |
| Schistocytes | RBC fragmentation | TTP, HUS, DIC, mechanical heart valve hemolysis |
| Sickle cells | Hemoglobin polymerization | Sickle cell disease |
| Target cells | Redundant red cell membrane | Thalassemia, liver disease, hemoglobinopathies |
| Teardrop cells | Marrow infiltration/fibrosis | Myelofibrosis |
| Basophilic stippling | Pathologic precipitation of polyribosomes | Thalassemia, lead poisoning |
| Echinocytes / Burr cells | Multiple small projections | Uremia, liver disease |
| Howell-Jolly bodies | Nuclear remnants | Asplenia, post-splenectomy |
| Polychromasia | Premature reticulocyte release | Hemolytic anemia, EPO stimulation |
| Elliptocytes / Pencil cells | Elongated RBCs | Iron deficiency, hereditary elliptocytosis |
| Nucleated RBCs | Marrow stress, asplenia | Massive hemorrhage, hemolysis, marrow fibrosis |
Step 3: Reticulocyte Count - Assesses Bone Marrow Response
Reticulocytes are young RBCs containing residual mRNA, present for ~24 hours after marrow release.
- Corrected reticulocyte count = Measured % × (Patient Hct / 45)
- Absolute reticulocyte count (preferred): directly measures reticulocytes per volume - no correction needed
| Reticulocyte Count | Interpretation |
|---|---|
| High (>100,000/μL) | Hyperproductive marrow - blood loss or hemolysis |
| Low/Normal in anemia | Hypoproductive - marrow failure, nutritional deficiency, renal disease |
Step 4: Iron Studies - For Microcytic or Suspected Iron-Deficiency Anemia
| Test | Normal | Iron Deficiency | Anemia of Chronic Disease |
|---|---|---|---|
| Serum Iron | 60-170 μg/dL | ↓ Low | ↓ Low |
| Serum Ferritin | 15-300 ng/mL | ↓ Low (<15) - most specific | Normal / ↑ High |
| TIBC (Total Iron Binding Capacity) | 250-370 μg/dL | ↑ High | ↓ Low / Normal |
| Transferrin saturation | 20-50% | ↓ Low (<15%) | ↓ Low |
| Soluble Transferrin Receptor (sTfR) | 8.7-28.1 nmol/L | ↑ Elevated | Normal |
| sTfR/Ferritin ratio | - | ↑ High | Normal |
Serum ferritin is the single best test for iron deficiency: a ferritin <15 ng/mL virtually confirms iron deficiency (high specificity); ferritin >100 ng/mL has a very low likelihood ratio for iron deficiency (LR- ~0.08). - Symptom to Diagnosis, 4th Ed.
Step 5: Additional Targeted Tests (Based on Suspected Cause)
For Macrocytic / Megaloblastic Anemia
- Serum Vitamin B12 - <200 pg/mL suggests deficiency
- Serum folate / RBC folate - RBC folate is more reliable
- Methylmalonic acid (MMA) and Homocysteine - elevated in B12 deficiency; only homocysteine elevated in folate deficiency
- Anti-intrinsic factor antibodies - for pernicious anemia
- Anti-parietal cell antibodies - for pernicious anemia
For Hemolytic Anemia
- LDH - elevated (released from lysed RBCs)
- Indirect bilirubin - elevated (from heme breakdown)
- Haptoglobin - decreased (consumed by free hemoglobin)
- Direct Coombs Test (DAT) - positive in autoimmune hemolytic anemia
- Urine hemoglobin / hemosiderinuria - intravascular hemolysis
For Suspected Hemoglobinopathy / Thalassemia
- Hemoglobin electrophoresis - identifies abnormal Hgb variants (HbS, HbC, HbH)
- HPLC (High-Performance Liquid Chromatography) - gold standard for Hgb typing
- Genetic/molecular testing - for alpha-thalassemia gene deletions
For Aplastic Anemia / Bone Marrow Failure
- Bone marrow aspiration + biopsy - mandatory
- Normal M:E ratio = 2.5:1
- Performed from the posterior iliac spine
- Biopsy must be done BEFORE aspiration to avoid artifact
- Indications include: circulating blasts, severe pancytopenia, reticulocytes <0.1%, unexplained severe anemia, evidence of marrow infiltration
For Renal Anemia
- Serum creatinine / eGFR - chronic kidney disease suppresses EPO
- Serum EPO level - inappropriately low in renal anemia
Diagnostic Algorithm Summary
ANEMIA CONFIRMED (low Hgb on CBC)
|
Peripheral Blood Smear + Reticulocyte Count
|
_____|__________________________________________
| | |
MICROCYTIC NORMOCYTIC MACROCYTIC
(MCV <80) (MCV 80-100) (MCV >100)
| | |
Iron studies Reticulocyte count B12, folate, MMA
Ferritin High → Hemolysis/ Homocysteine
TIBC blood loss Thyroid function
Hgb electro- Low → Marrow failure/ Liver enzymes
phoresis CKD/chronic disease Bone marrow biopsy
Sources: Harrison's Principles of Internal Medicine 22E (2025), Washington Manual of Medical Therapeutics, Goldman-Cecil Medicine, Symptom to Diagnosis 4th Ed., Robbins Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.