Murmurs basics to clinical
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive content from Harrison's, Rosen's EM, Guyton, and other sources. Let me compile the complete, structured answer.
Heart Murmurs: Basics to Clinical
1. What Is a Murmur?
A heart murmur is an audible vibration caused by turbulent blood flow through the heart or great vessels. Turbulence arises from:
- High velocity flow across a normal or abnormal valve
- Forward flow across an obstructed orifice
- Backward (regurgitant) flow across an incompetent valve
- Shunting of blood through an abnormal communication
The intensity, duration, configuration, and timing are all determined by the magnitude, variability, and duration of the responsible pressure difference between two cardiac chambers or great arteries.
(Harrison's Principles of Internal Medicine 22E, p.1909)
2. Grading Murmur Intensity (Levine Scale 1-6)
| Grade | Description |
|---|---|
| 1/6 | Barely audible; requires concentration in a quiet room |
| 2/6 | Soft but clearly audible |
| 3/6 | Moderately loud; no thrill |
| 4/6 | Loud; thrill present |
| 5/6 | Very loud; audible with stethoscope barely on chest; thrill present |
| 6/6 | Audible with stethoscope off the chest; thrill present |
A thrill (palpable murmur) is present at grade 4 and above.
3. Heart Sounds: The Backdrop
Before understanding murmurs, you need the normal sounds firmly in mind.
S1 = Mitral + tricuspid valve closure (start of systole)
- Loud S1: early rheumatic MS, short PR interval, hyperkinetic states
- Soft S1: calcified/rigid MS leaflets, long PR interval, beta-blockers, LV dysfunction
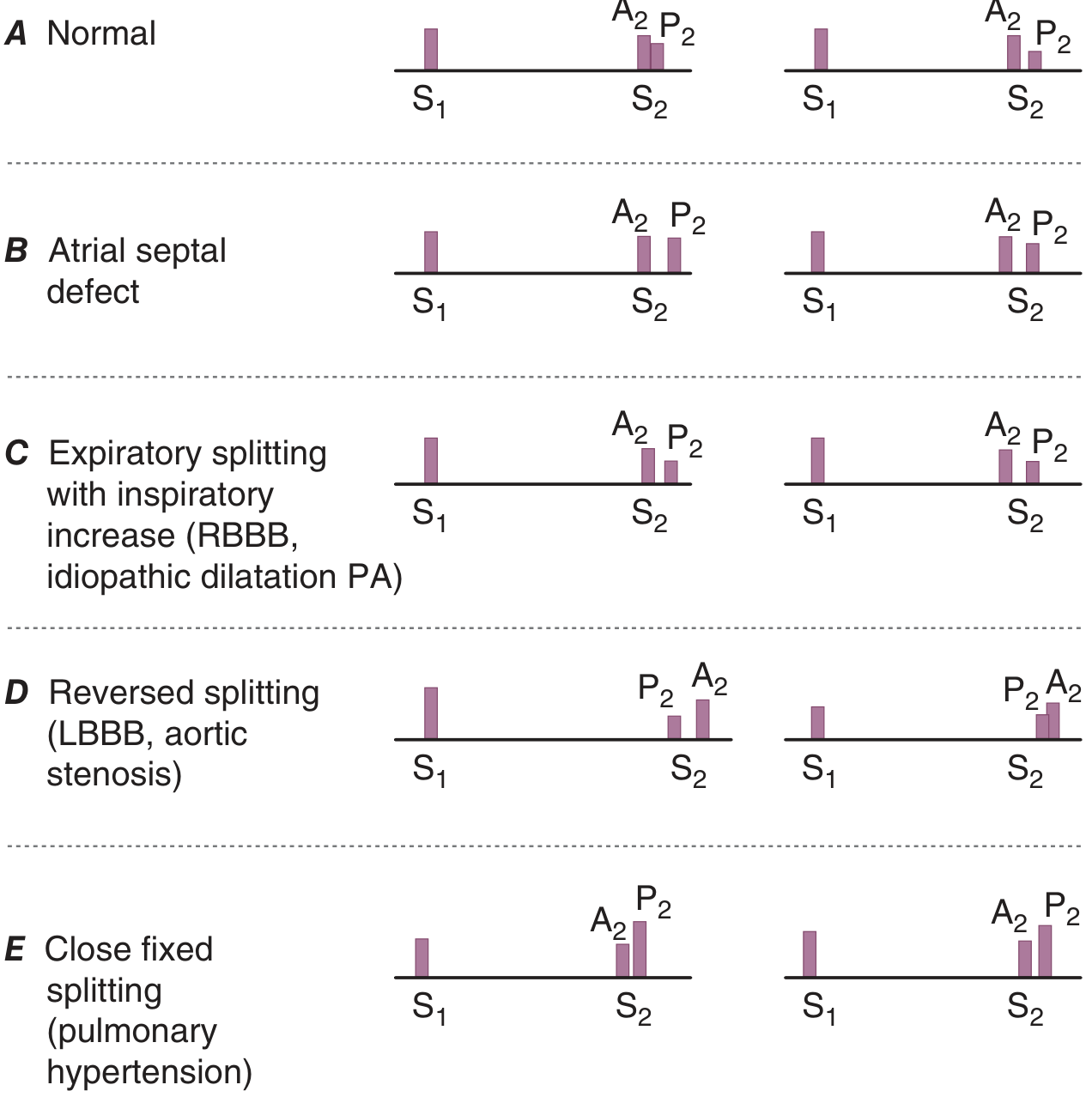
S2 = Aortic (A2) + pulmonic (P2) valve closure (end of systole)
- Normal splitting: A2-P2 interval widens with inspiration
- Fixed splitting = ASD (constant RA volume overload regardless of respiration)
- Wide splitting = RBBB (delayed P2)
- Reversed/paradoxical splitting = LBBB, RV pacing, severe AS, HOCM (P2 before A2; gap narrows with inspiration)
- Narrow/single S2 = Pulmonary arterial hypertension
S3 (ventricular gallop): Early diastolic - rapid filling phase. Normal in young; pathologic (heart failure) in older adults. Predicts cardiovascular mortality in chronic heart failure.
S4 (atrial gallop): Late diastolic - atrial filling phase. Seen in LV hypertrophy, ischemia. Absent in AF.
Opening snap (OS): High-pitched early diastolic sound in MS. The A2-OS interval is inversely proportional to severity (shorter interval = higher LA-LV gradient = more severe MS).
Ejection click: Early systolic, high-pitched. Seen with bicuspid aortic/pulmonic valve or root dilation.
Pericardial knock (PK): High-pitched, slightly later than OS; marks abrupt cessation of ventricular expansion in constrictive pericarditis.
(Harrison's Principles of Internal Medicine 22E, p.1908-1909)
4. Murmur Timing and Configuration
The pressure gradient between cardiac structures is the key driver:
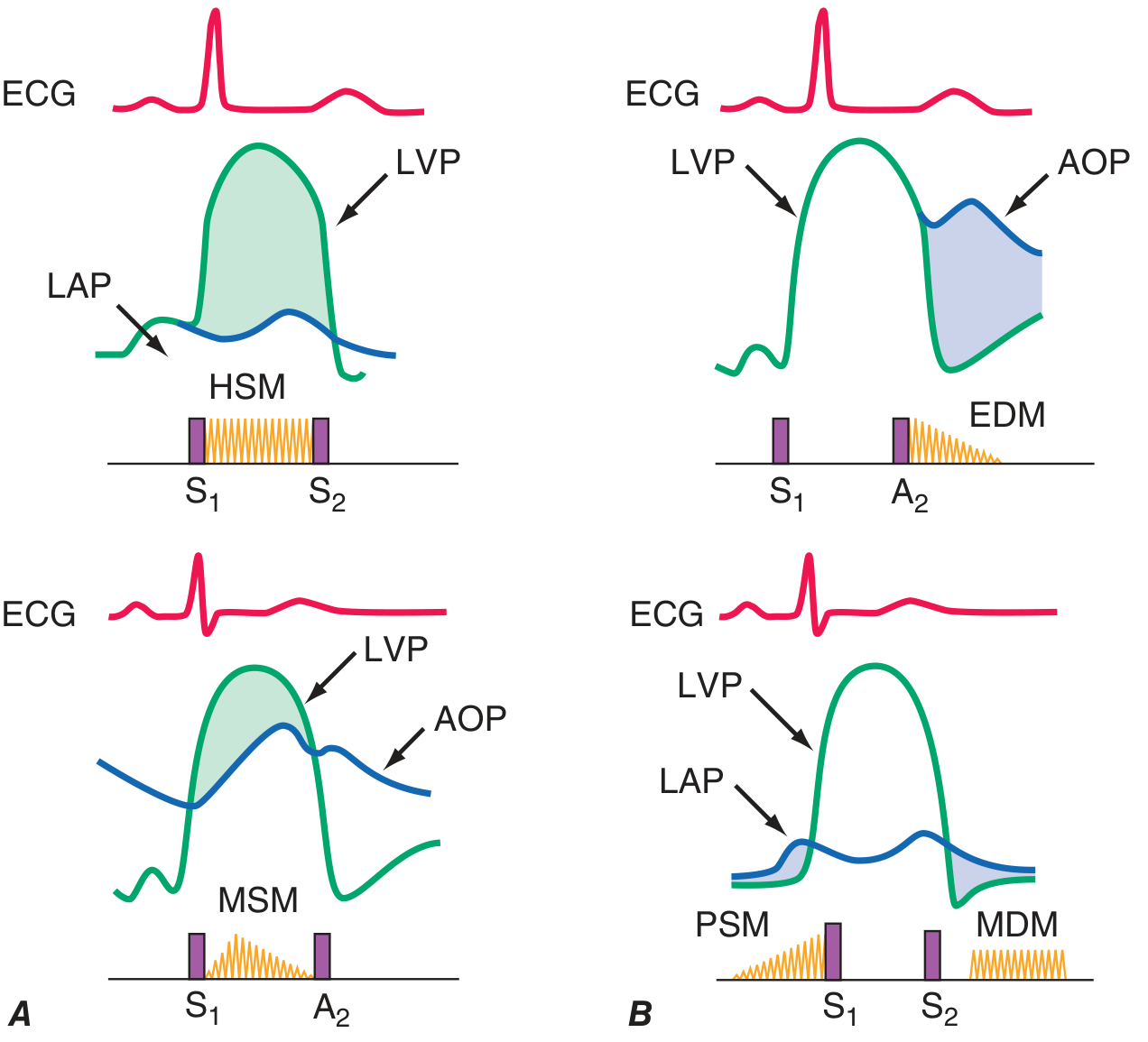
Systolic Murmurs
Early systolic - Begins at S1, decrescendo, ends before S2
- Acute severe MR (steep rise in LA pressure quickly equalizes LV-LA gradient)
- Acute TR with normal PA pressures
Mid-systolic (ejection) - Crescendo-decrescendo; begins after S1, ends before S2
- Aortic stenosis (AS) - most common cause in adults
- Pulmonic stenosis (PS)
- HOCM
- Aortic sclerosis
- High-flow states: fever, pregnancy, thyrotoxicosis, anemia, ASD with L-to-R shunt
Holosystolic (pansystolic) - Begins with S1, fills entire systole, ends at S2; implies a constant pressure gradient throughout systole
- Mitral regurgitation (MR) - chronic
- Tricuspid regurgitation (TR) - chronic
- Ventricular septal defect (VSD)
Late systolic - Begins mid-to-late systole, ends at S2
- Mitral valve prolapse (MVP) - preceded by a midsystolic click
Diastolic Murmurs
Early diastolic (decrescendo) - Begins at S2, decrescendo
- Aortic regurgitation (AR) - high-pitched, blowing, LSB
- Pulmonic regurgitation (PR) - Graham Steell murmur in pulmonary HTN
Mid-diastolic (rumble) - Low-pitched, after OS or S3
- Mitral stenosis (MS) - apical rumble with presystolic accentuation
- Tricuspid stenosis (TS) - LLSB, louder with inspiration
- Austin Flint murmur - mid-to-late diastolic rumble in severe AR (functional MS from AR jet impinging on MV leaflet); decreases with vasodilators
Presystolic - Late diastolic, just before S1; seen in MS with sinus rhythm (atrial kick)
Continuous Murmurs
Begin in systole, envelop S2, continue through diastole. Implies a pressure gradient present throughout the cardiac cycle.
- Patent ductus arteriosus (PDA) - classic "machinery murmur," 2nd-3rd left interspace
- Ruptured sinus of Valsalva aneurysm
- Coronary/great vessel arteriovenous fistula
- Cervical venous hum (benign) - supraclavicular, children/adolescents; obliterated by pressure
- Mammary soufflé (benign) - pregnancy; diastolic component obliterated by pressure
(Harrison's Principles of Internal Medicine 22E, p.1909-1910; Rosen's Emergency Medicine)
5. Auscultation Locations
| Area | Location | Key Murmurs |
|---|---|---|
| Aortic area | 2nd right interspace | AS (radiates to carotids) |
| Pulmonic area | 2nd left interspace | PS, ASD, innocent pulmonic flow |
| Tricuspid area | Lower left sternal border | VSD, TR, TS |
| Mitral area (apex) | 5th ICS, MCL | MR (radiates to axilla), MS |
Radiation clues:
- AS: apex to carotids (right)
- MR (posterior leaflet): anteriorly toward base (can mimic AS)
- MR (anterior leaflet): posteriorly to the axilla
- VSD: LLSB, radiates across chest
6. Bedside Maneuvers
This is where exam skill meets clinical medicine. Understanding maneuvers predicts the pathophysiology.
| Maneuver | Effect on Preload/Afterload | Key Effects |
|---|---|---|
| Valsalva (strain phase) | Decreases preload | HOCM louder, MVP click moves earlier; most others softer |
| Standing quickly | Decreases preload | HOCM louder, MVP click moves earlier |
| Squatting | Increases preload + afterload | HOCM softer, MVP click moves later |
| Passive leg raising | Increases preload | HOCM softer |
| Inspiration | Increases right heart filling | Right-sided murmurs louder (TR, PS, TS) - Carvallo's sign |
| Expiration | Increases left heart filling | Left-sided murmurs louder |
| Amyl nitrite | Vasodilator - decreases afterload | AS/HOCM louder; MR softer |
| Handgrip | Increases afterload | MR/AR/VSD louder; AS softer |
Key rule for HOCM vs other systolic murmurs: Any maneuver that decreases LV volume (less preload, more contractility) increases HOCM murmur. Any maneuver that increases LV volume decreases it.
(Harrison's Principles of Internal Medicine 22E, Table 246-1)
7. Innocent / Functional Murmurs
Not all murmurs are pathologic. Functional murmurs are always systolic, never diastolic.
| Murmur | Population | Character | Location |
|---|---|---|---|
| Still's murmur | Children 2-6 years | Low-pitched, musical/vibratory, grade 1-3 | LLSB to apex |
| Pulmonary flow murmur | Neonates, young adults | Soft systolic ejection | LUSB |
| Venous hum | Children | Continuous, low-pitched | Supraclavicular; obliterated by pressure |
| Physiologic/flow murmur | Pregnancy, fever, anemia, thyrotoxicosis | Midsystolic, soft | Variable |
Signs that a murmur is pathologic (not innocent):
- Diastolic timing
- Grade ≥ 3/6 systolic, holosystolic, or late systolic
- Associated with a thrill
- Abnormal heart sounds (clicks, gallops, rubs)
- Cyanosis, respiratory distress
- Abnormal ECG or chest X-ray
- Bounding or weak pulses
(Rosen's Emergency Medicine; Swanson's Family Medicine Review)
8. Key Valvular Lesions - Clinical Correlation
Aortic Stenosis (AS)
- Murmur: Midsystolic crescendo-decrescendo, best at 2nd RSB, radiates to carotids
- Severity markers: Parvus et tardus carotid pulse, late-peaking murmur (grade ≥3), soft A2, sustained LV apical impulse, S4
- S2: Reversed splitting (LBBB-like delay)
- Note: Elderly hypertensive patients and low-output states can mask severity (soft murmur despite severe AS)
Mitral Regurgitation (MR)
- Acute severe MR: Early systolic decrescendo (LA pressure rises sharply = gradient equalizes)
- Chronic MR: Holosystolic, blowing, best at apex
- Posterior leaflet: radiates to base (can mimic AS)
- Anterior leaflet: radiates to axilla/back
- Functional MR from annular dilation (DCM) also gives holosystolic apical murmur
Mitral Stenosis (MS)
- Murmur: Low-pitched mid-diastolic rumble at apex; presystolic accentuation (sinus rhythm only)
- Loud S1 + Opening Snap (OS) = classic triad
- A2-OS interval inversely proportional to MS severity
- S1 and OS soften with progressive leaflet calcification
Mitral Valve Prolapse (MVP)
- Midsystolic click followed by late systolic murmur
- With standing/Valsalva: click moves earlier (less LV volume)
- With squatting: click moves later (more LV volume)
Aortic Regurgitation (AR)
- Early diastolic decrescendo: High-pitched, blowing, best at 3rd LSB (Erb's point); patient leaning forward, breath held in expiration
- Austin Flint murmur: Mid-to-late diastolic rumble at apex (regurgitant jet causes functional MS)
- Wide pulse pressure, water-hammer pulse, Corrigan's sign
PDA - Machinery Murmur
- Continuous murmur: louder in systole, softer in diastole, waxes and wanes with heartbeat
- 2nd-3rd left interspace
(Harrison's Principles of Internal Medicine 22E; Guyton & Hall Medical Physiology)
9. Diagnostic Approach
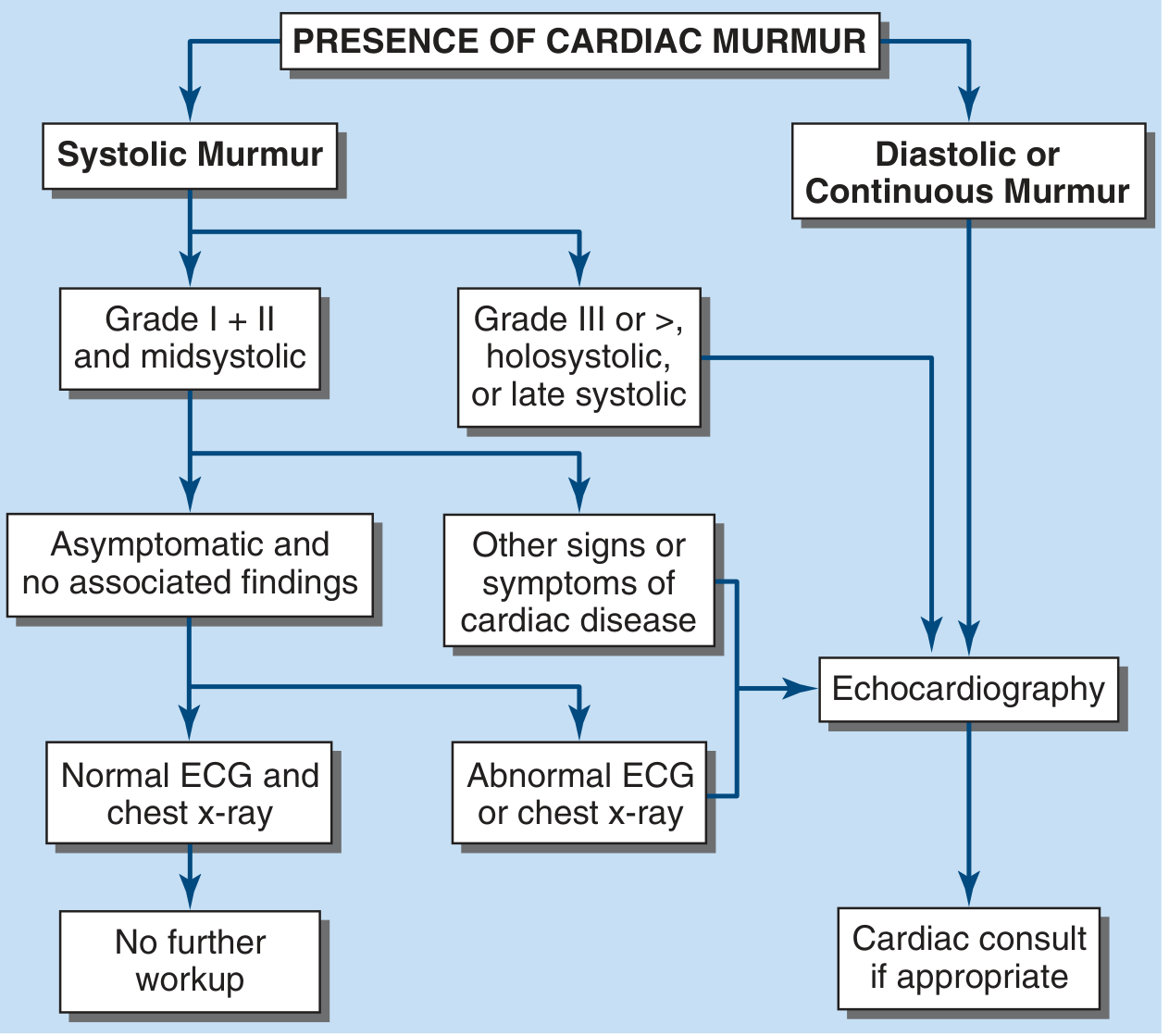
Key decision points:
- Soft midsystolic murmur (grade 1-2), asymptomatic child/young adult, normal ECG + CXR → no further workup needed
- Loud systolic murmur (grade ≥3), holosystolic, or late systolic → Echocardiography
- Any diastolic or continuous murmur → Echocardiography + cardiac consult
Two-dimensional and Doppler echocardiography remain the gold standard for characterizing valvular lesions, estimating gradients, and guiding management.
(Harrison's Principles of Internal Medicine 22E, p.1886)
10. Quick Reference Summary Table
| Condition | Timing | Shape | Quality | Location | Radiation | Special Features |
|---|---|---|---|---|---|---|
| AS | Midsystolic | Crescendo-decrescendo | Harsh | 2nd RSB | Carotids | Parvus et tardus, reversed S2 split |
| MR (chronic) | Holosystolic | Plateau | Blowing | Apex | Axilla | S3 common |
| MS | Mid-diastolic | Rumble + presystolic accentuation | Low | Apex | None | Loud S1, OS, A2-OS inversely ~severity |
| AR | Early diastolic | Decrescendo | High-pitched blowing | 3rd LSB | None | Wide pulse pressure, Austin Flint |
| PS | Midsystolic | Crescendo-decrescendo | Harsh | 2nd LSB | None | Ejection click, louder with inspiration |
| TR | Holosystolic | Plateau | Blowing | LLSB | None | Louder with inspiration (Carvallo's) |
| VSD | Holosystolic | Plateau | Harsh | LLSB | Across chest | Grade inversely ~ defect size |
| HOCM | Midsystolic | Crescendo-decrescendo | Harsh | LLSB/apex | None | Louder with Valsalva/standing |
| MVP | Late systolic | Crescendo | Blowing | Apex | Axilla | Preceded by midsystolic click |
| PDA | Continuous | Waxes/wanes | Machinery | 2nd-3rd LSB | None | Peaks at S2 |
| ASD | Midsystolic | Crescendo-decrescendo | Soft | 2nd LSB | None | Fixed S2 splitting, flow murmur |
(Harrison's Principles of Internal Medicine 22E; Rosen's Emergency Medicine; Guyton & Hall)
This is a shared conversation. Sign in to Orris to start your own chat.