Differential diagnosis of acute intestinal infections and infectious dirrhea
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have rich, comprehensive material from multiple authoritative sources. Let me compile the full response.
Differential Diagnosis of Acute Intestinal Infections and Infectious Diarrhea
Classification Framework
The first step in the differential is understanding the mechanistic classification of diarrhea. Infectious diarrhea sits under the inflammatory umbrella but branches into noninvasive and invasive categories:
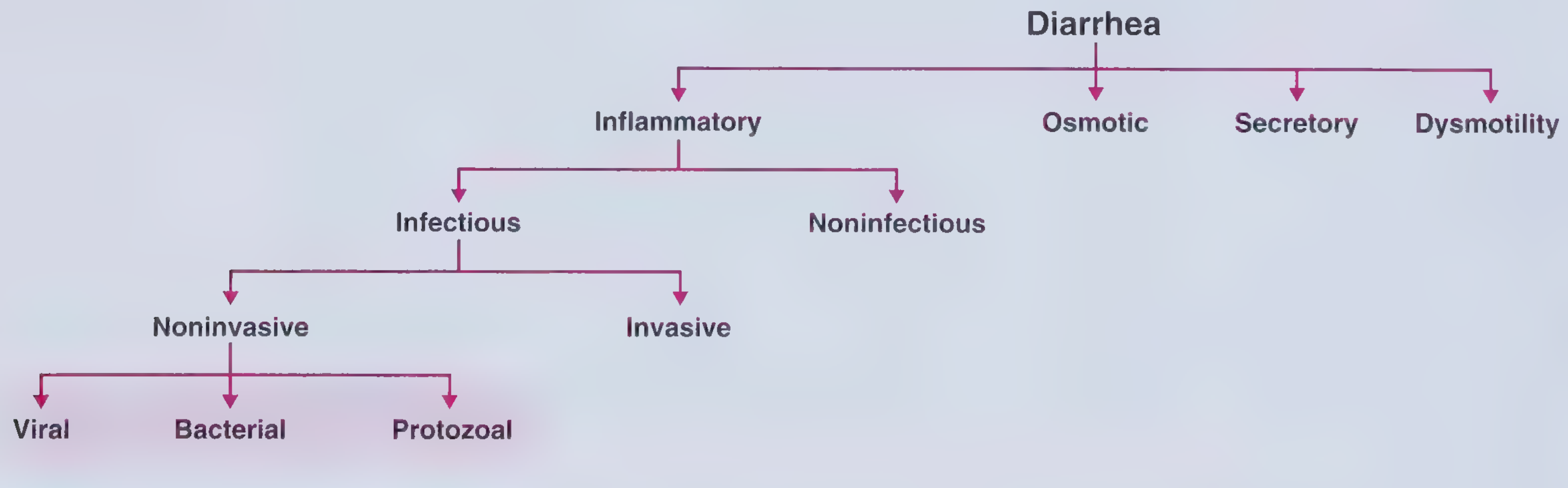
(Frameworks for Internal Medicine)
Step 1: Is This Infectious or Noninfectious?
Before differentiating among infectious causes, rule out noninfectious etiologies that mimic infectious diarrhea:
| Category | Examples |
|---|---|
| Osmotic diarrhea | Lactose intolerance, sorbitol/fructose ingestion, antacids, laxatives |
| Medications | Metformin, antibiotics, colchicine, digoxin, SSRIs |
| Inflammatory bowel disease | Ulcerative colitis, Crohn's disease |
| Microscopic colitis | Collagenous or lymphocytic colitis (chronic watery diarrhea, older women, associated with NSAIDs/PPIs) |
| Ischemic colitis | Sudden onset bloody diarrhea in elderly or vascular disease patients |
| Malabsorption | Celiac disease, exocrine pancreatic insufficiency |
| Functional | IBS (no nocturnal symptoms, no weight loss, no blood) |
| Endocrine | Hyperthyroidism, VIPoma, carcinoid |
Key distinguishing features of infectious vs. noninfectious diarrhea:
- Infectious: acute onset, epidemiological exposure, fever, fecal leukocytes/lactoferrin/calprotectin
- Noninfectious IBD: longer duration (weeks-months), no pathogenic organism isolated, nocturnal symptoms, extraintestinal manifestations (uveitis, arthritis, skin lesions)
- IBS: no rectal bleeding, no nocturnal symptoms, no incontinence, no weight loss
"An important distinction between acute bacterial infections and ulcerative colitis is that the diarrhea in infectious diseases tends to be limited to a period of days to a few weeks, whereas the diarrhea of ulcerative colitis is typically of longer duration." - Yamada's Textbook of Gastroenterology, 7th ed.
Step 2: Classify Infectious Diarrhea - Noninvasive vs. Invasive
| Feature | Noninvasive (Secretory/Toxigenic) | Invasive (Dysenteric/Inflammatory) |
|---|---|---|
| Stool | Watery, large volume, no blood | Bloody/mucoid, small volume, frequent |
| Fever | Absent or low-grade | Often high-grade |
| Tenesmus | Absent | Common |
| Fecal leukocytes | Absent | Present (PMNs) |
| Location of disease | Small intestine (proximal) | Large intestine (distal/colon) |
| Mechanism | Enterotoxin-mediated, osmotic | Mucosal invasion, cytotoxin |
| Abdominal pain | Periumbilical cramps | Lower quadrant, colicky |
(Frameworks for Internal Medicine)
Step 3: Differential Among Specific Infectious Causes
Diagnostic Approach Algorithm
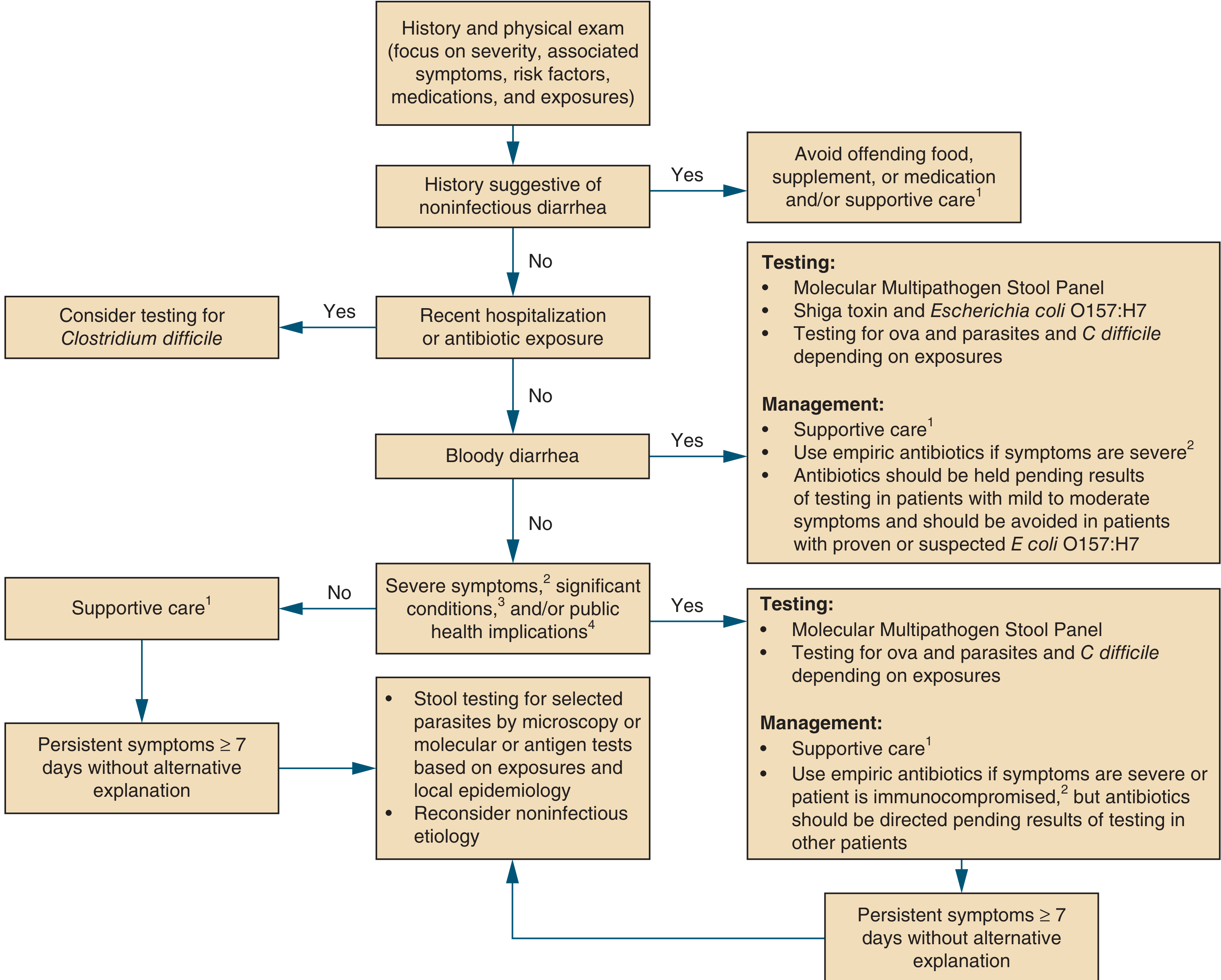
(Symptom to Diagnosis: An Evidence Based Guide, 4th ed., Figure 13-1)
A. Viral Gastroenteritis
The most common cause of acute infectious diarrhea overall. Diagnosis is usually clinical; ELISA and PCR assays are available for confirmation.
| Virus | Epidemiology | Incubation | Duration | Key Features |
|---|---|---|---|---|
| Norovirus | Most common in adults/older children; cruise ships, nursing homes, schools; year-round but peaks in cold weather | 12-48 h | 1-2 days | Vomiting prominent, myalgias, headache, watery diarrhea; highly contagious (low inoculum, fecal-oral + aerosolization); ~50% of all gastroenteritis outbreaks in the US |
| Rotavirus | Leading cause in unvaccinated young children; also adults; winter peak in temperate climates | 1-3 days | 5-7 days (longer in immunocompromised) | Fever, vomiting, voluminous watery diarrhea; ~50% of exposed children and ~33% of household adults infected |
| Enteric Adenovirus (types 40, 41) | Infants/young children; most adults asymptomatic | 8-10 days | 5-12 days | Prolonged watery diarrhea; does NOT cause nasopharyngitis/keratoconjunctivitis (unlike conventional adenovirus) |
| Astrovirus | Infants, young children; outbreaks in military recruits, nursing homes | 1-2 days | 2-5 days | Milder than rotavirus; watery diarrhea prominent |
(Frameworks for Internal Medicine; Harrison's Principles of Internal Medicine, 22nd ed.)
B. Noninvasive Bacterial / Toxigenic Diarrhea
Preformed toxin or enterotoxin-mediated; typically no fever, no fecal leukocytes, rapid onset after food ingestion.
| Organism | Incubation | Duration | Source | Key Features |
|---|---|---|---|---|
| Staphylococcus aureus | 1-6 h | 6-12 h | Mayonnaise, potato salad, food handlers | Preformed heat-stable toxin; sudden onset vomiting > diarrhea; self-limited; no fever |
| Bacillus cereus | 1-6 h (emetic); 6-12 h (diarrheal) | 1-2 days | Fried rice, reheated foods | Two syndromes: emetic (vomiting, like S. aureus) and diarrheal (watery stools) |
| Clostridium perfringens | 6-24 h | ~1 day | Steam-table meat, poultry, gravy | Watery diarrhea without vomiting; large foodborne outbreaks; in-vivo toxin production |
| Vibrio cholerae | 1-2 days | 6-8 days | Raw shellfish, contaminated water (travel to Asia) | "Rice-water" diarrhea, profound secretory diarrhea, rapid dehydration; cholera toxin raises cAMP |
| ETEC (Enterotoxigenic E. coli) | 1-3 days | 1-7 days | Contaminated water/food | Most common cause of traveler's diarrhea; watery, non-bloody |
| Clostridioides difficile | 5-14 days (post-antibiotic) | Variable | Person-to-person, surfaces | Antibiotic or PPI exposure; colitis, fever, pseudomembranes; toxic megacolon risk; high mortality in elderly/immunocompromised |
(Rosen's Emergency Medicine; Symptom to Diagnosis, 4th ed.)
C. Invasive (Dysenteric) Bacterial Diarrhea
Mucosal invasion of the colon; bloody/mucoid stool, fever, fecal leukocytes, tenesmus.
| Organism | Incubation | Duration | Source | Key Features |
|---|---|---|---|---|
| Shigella spp. | 1-2 days | 2-7 days | Water, person-to-person | Classic dysentery; low inoculum; fever, tenesmus, hematochezia; high incidence in men who have sex with men; toxigenic component (Shiga toxin in S. dysenteriae); complications: HUS, seizures, toxic megacolon |
| Salmonella (nontyphoidal) | 12-24 h | 2-7 days | Eggs, poultry, unpasteurized milk, reptiles | Watery diarrhea with fever; self-limited; more severe in sickle cell, immunocompromised; bacteremia risk |
| Salmonella typhi (typhoid fever) | 12-24 h | Weeks | Food, person-to-person (travel) | Stepwise fever, headache, constipation then diarrhea, splenomegaly, rose spots, altered mental status; systemic illness |
| Campylobacter jejuni | 2-5 days | 5-14 days | Undercooked poultry, untreated water, pets | Most common bacterial pathogen in stool cultures; watery then bloody diarrhea, fever, crampy pain; post-infectious Guillain-Barre, reactive arthritis |
| Yersinia enterocolitica | 12-48 h | 5-14 days | Pork, water, milk, cats, dogs, pigs | Acute diarrhea; right lower quadrant pain mimicking appendicitis (mesenteric lymphadenitis); common with travel to Asia |
| STEC / E. coli O157:H7 | 3-8 days | 5-10 days | Undercooked beef, raw milk, produce | Bloody diarrhea without fever (characteristic); Shiga toxin; high risk of HUS and TTP; antibiotics CONTRAINDICATED |
| Vibrio parahaemolyticus | 8-24 h | 5-14 days | Raw/undercooked seafood, shellfish | Watery diarrhea, sometimes dysenteric; associated with seafood consumption |
(Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Symptom to Diagnosis, 4th ed.)
D. Parasitic / Protozoal Infections
Consider in prolonged (>7-14 days), travel-related, or immunocompromised presentations.
| Organism | Duration | Source | Key Features |
|---|---|---|---|
| Giardia lamblia | Weeks-months | Untreated freshwater, person-to-person | Chronic, non-bloody watery diarrhea, bloating, flatulence, weight loss, steatorrhea; NO rectal bleeding |
| Entamoeba histolytica | Variable | Contaminated food/water (travel to endemic areas) | Bloody diarrhea resembling UC/Crohn's; ulcers scattered in cecum/ascending colon, covered with yellow exudate containing organisms; can cause amoebic liver abscess |
| Cryptosporidium spp. | Self-limited (immunocompetent); prolonged (HIV/AIDS) | Water, petting zoos, farm animals | Watery diarrhea; profuse and life-threatening in immunocompromised; chlorine-resistant |
| Cyclospora cayetanensis | Weeks | Contaminated produce (fresh berries, herbs) | Watery diarrhea, fatigue, weight loss; prolonged if untreated |
| Balantidium coli | Variable | Exposure to pigs | Rare; dysenteric illness |
E. Special Situations
Clostridioides difficile colitis - always consider in any patient with recent antibiotic use or hospitalization. The diagnosis is made by PCR or toxin assay, not culture alone.
Immunocompromised host (HIV/AIDS, transplant): Expand the differential to include CMV colitis (watery or bloody diarrhea, mucosal ulcerations on endoscopy), Mycobacterium avium complex (MAI), Microsporidium, and Isospora belli. Blood cultures are important; viral culture and histological examination of biopsies are required. (Yamada's Gastroenterology, 7th ed.)
Sexually transmitted proctitis: In patients with anal-receptive intercourse, consider Neisseria gonorrhoeae, Chlamydia trachomatis (lymphogranuloma venereum), herpes simplex virus, and Treponema pallidum - these cause proctitis that may resemble UC on endoscopy.
Traveler's diarrhea: Most common cause is ETEC. Other agents include norovirus, Campylobacter, Shigella, Salmonella, and Cryptosporidium. Regional differences in epidemiology are critical in history-taking.
Step 4: Exposure-Based Differential
The exposure history is essential for prioritizing the differential (Symptom to Diagnosis, 4th ed.):
| Exposure | Most Likely Pathogens |
|---|---|
| Unpasteurized dairy | Salmonella, Campylobacter, Yersinia, S. aureus, Cryptosporidium, Listeria, STEC |
| Raw/undercooked poultry | Campylobacter, Salmonella, STEC, C. perfringens, S. aureus |
| Raw shellfish | Vibrio spp., norovirus, hepatitis A |
| Fried/reheated rice | B. cereus |
| Recent antibiotics/hospitalization | C. difficile |
| Untreated freshwater | Campylobacter, Cryptosporidium, Giardia, Shigella, Salmonella |
| International travel | ETEC, Salmonella typhi, Cryptosporidium, Giardia, norovirus, Cyclospora |
| Farm/petting zoo | STEC, Cryptosporidium, Campylobacter |
| Reptiles, poultry | Nontyphoidal Salmonella |
Step 5: Laboratory Approach to Distinguish Causes
| Finding | Suggests |
|---|---|
| Fecal PMNs / lactoferrin / calprotectin | Invasive bacterial colitis, IBD |
| No fecal leukocytes | Viral, ETEC, C. perfringens, S. aureus, Giardia |
| Bloody stool, no fever | STEC O157:H7 (do NOT use antibiotics) |
| Bloody stool with fever | Shigella, Campylobacter, Salmonella, amebiasis |
| Leukocytosis with left shift | Invasive bacterial (Shigella, Salmonella); not typically viral |
| Lymphocytosis or normal WBC/differential | Viral gastroenteritis (Sleisenger and Fordtran's GI and Liver Disease) |
| Stool culture | Salmonella, Shigella, Campylobacter, Yersinia, Vibrio |
| PCR multiplex stool panel | Broadest coverage; preferred for severe/hospitalized patients |
| C. difficile toxin PCR | Post-antibiotic diarrhea |
| O&P (ova and parasites) | Persistent diarrhea >7 days, travel, immunocompromise |
Summary: Key Distinguishing Patterns
| Pattern | Leading Diagnosis |
|---|---|
| Vomiting-dominant, 1-2 days, no fever, group setting | Norovirus, S. aureus (very rapid onset) |
| Watery diarrhea <7 days, low-grade fever, no blood | Viral (rotavirus, norovirus), ETEC |
| Bloody diarrhea + high fever + fecal PMNs | Shigella, Campylobacter, Salmonella |
| Bloody diarrhea + NO fever + HUS | STEC O157:H7 |
| Watery diarrhea + post-antibiotic | C. difficile |
| Prolonged watery diarrhea + bloating + NO blood | Giardia |
| Bloody diarrhea + chronic course + no pathogen | Ulcerative colitis, Crohn's |
| Right lower quadrant pain mimicking appendicitis | Yersinia enterocolitica |
| Profound "rice-water" dehydrating diarrhea | Vibrio cholerae |
| Diarrhea in immunocompromised | CMV, Cryptosporidium, MAC, Microsporidium |
Sources:
- Symptom to Diagnosis: An Evidence Based Guide, 4th ed. (McGraw Hill)
- Frameworks for Internal Medicine (Wolters Kluwer)
- Harrison's Principles of Internal Medicine, 22nd ed. (McGraw Hill)
- Tintinalli's Emergency Medicine, 9th ed. (McGraw Hill)
- Rosen's Emergency Medicine, 9th ed. (Elsevier)
- Yamada's Textbook of Gastroenterology, 7th ed. (Wiley)
- Sleisenger and Fordtran's GI and Liver Disease (Elsevier)
This is a shared conversation. Sign in to Orris to start your own chat.