Do heart have m3 receptors
Reading File
Searching PubMed
M3 muscarinic receptor heart cardiac
Finding Sources
Searching PubMed
muscarinic receptor subtypes cardiac M2 M3
Reading File
Reading File
Here is a thorough answer based on authoritative textbooks:
Do the Heart Have M3 Receptors?
Yes, the heart does have M3 muscarinic receptors, but their distribution and importance differ from the dominant M2 subtype.
Muscarinic Receptor Distribution in the Heart
| Receptor | Location in Heart | Role |
|---|---|---|
| M2 | Predominant subtype - SA node, AV node, atrial myocardium, ventricles | Main mediator of vagal/parasympathetic cardiac effects |
| M3 | Coronary circulation (endothelium & smooth muscle); also some non-M2 sites in the myocardium | Coronary vasodilation; minor cardiomyocyte effects |
M2 Receptors - The Dominant Cardiac Subtype
M2 receptors are the predominant muscarinic subtype in the mammalian heart. When activated by acetylcholine (released by vagal nerve endings):
- Decrease heart rate (negative chronotropy) - slowing SA node pacemaker activity
- Slow AV conduction (negative dromotropy)
- Directly decrease atrial contractile force
- Exert inhibitory modulation of ventricular contractile force
Mechanism: M2 couples to the Gi/o protein (pertussis toxin-sensitive), which:
- Inhibits adenylyl cyclase (reducing cAMP)
- Increases K+ conductance (via GIRK channels) → hyperpolarization
- Modulates Ca2+ channels and If (funny current)
M3 Receptors in the Heart - Where and Why
M3 receptors have been specifically identified in the coronary circulation. Additionally, "non-M2 receptors" have been reported to exist in the heart more broadly (Miller's Anesthesia).
M3 receptor locations:
- Coronary vascular endothelium - stimulation causes release of nitric oxide (NO) → vasodilation
- Coronary vascular smooth muscle - direct relaxation
- Lung, bladder, exocrine glands, smooth muscle are the classic peripheral sites (Lippincott Pharmacology)
Mechanism of M3 signaling (wherever it acts):
- Couples to Gq/11 protein
- Activates phospholipase C
- Generates IP3 (raises intracellular Ca2+) and DAG (activates PKC)
Clinical Relevance
- Anticholinergic drugs (e.g., atropine, glycopyrrolate) block both M2 and M3 receptors. At the heart, M2 blockade is the clinically relevant effect (causing tachycardia).
- Selective M3 antagonists (e.g., darifenacin, used in overactive bladder) are designed to spare M2-mediated cardiac effects. However, since M3 receptors are present in the coronary circulation, they can affect coronary tone.
- The reference to "loss of vagally mediated bradycardia in mice lacking M2 or M3 muscarinic receptors" (from Goodman & Gilman's bibliography) suggests M3 may contribute to vagal bradycardia in some contexts as well.
Summary
The heart has both M2 and M3 muscarinic receptors. M2 is the dominant, clinically important subtype responsible for all classic parasympathetic cardiac effects (bradycardia, reduced AV conduction). M3 receptors are found mainly in the coronary circulation where they mediate vasodilation via NO, and there is some evidence of non-M2 (including M3) receptors in the myocardium itself.
- Miller's Anesthesia (10th ed.), Neural Regulation of Cardiac Function
- Lippincott Illustrated Reviews: Pharmacology, Muscarinic Receptors section
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Effect of parasympathetic
Asking for Preferences
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Here is a complete, textbook-based breakdown of parasympathetic effects:
Effects of Parasympathetic Stimulation ("Rest and Digest")
The parasympathetic nervous system uses acetylcholine (ACh) as its neurotransmitter at both pre- and postganglionic synapses, acting on muscarinic receptors at target organs.
Organ-by-Organ Effects
| Organ/System | Parasympathetic Effect |
|---|---|
| Eye | Pupillary constriction (miosis) via sphincter pupillae; increased lens curvature (accommodation for near vision) via ciliary muscle |
| Salivary Glands | Increased secretion - copious, watery saliva |
| Heart | Slowing of heart rate (bradycardia); decreased AV conduction; decreased atrial contractility |
| Lungs | Bronchoconstriction; increased bronchial secretions |
| GI Tract | Increased secretions; increased motility (peristalsis); relaxation of sphincters |
| Pancreas | Increased secretion (both exocrine and endocrine) |
| Male Sex Organs | Erection (point - parasympathetic = "P" for point) |
| Bladder | Detrusor contraction (micturition); internal urethral sphincter relaxation |
| Skin | No significant effect |
| Blood Vessels | Vasodilation in select beds (e.g., coronary via M3 on endothelium → NO release) |
Effects on the Heart - In Detail
The parasympathetic supply to the heart is via the vagus nerve (CN X). Postganglionic fibers act mainly at the SA node and AV node, with some supply to the atria and coronary arteries.
1. Negative Chronotropy (decreased heart rate)
- ACh acts on M2 receptors at the SA node
- Activates Gi → inhibits adenylyl cyclase (↓cAMP) + increases K+ conductance (GIRK channels) → hyperpolarization
- Slows diastolic depolarization → decreases firing rate
- Result: heart rate falls below 60 bpm (bradycardia)
- Extreme vagal stimulation can even stop the heart temporarily (e.g., carotid sinus syndrome causing syncope)
2. Negative Dromotropy (slowed AV conduction)
- ACh slows conduction through the AV node
- Increases PR interval on ECG
- Extreme stimulation can cause complete heart block
3. Negative Inotropy (decreased contractility)
- Direct decrease in atrial contractile force
- Indirect inhibitory modulation of ventricular contractility
4. Coronary Artery Constriction (direct effect)
- Postganglionic fibers extend into coronary arteries
- Direct effect is mild vasoconstriction
- However, M3 receptor stimulation on endothelium releases NO causing vasodilation (as discussed in the previous response)
Mechanism of Action - M2 Receptor Signaling
ACh → M2 receptor → Gi/o protein →
├── Inhibits adenylyl cyclase → ↓cAMP → ↓PKA → ↓Ca²⁺ influx
├── Opens GIRK (K⁺) channels → hyperpolarization
└── Modulates If (funny current) → slows pacemaker
Important Clinical Points
- Atropine (muscarinic antagonist) blocks all these effects - used to treat bradycardia and heart block
- Vagal tone at rest: the heart is under dominant parasympathetic influence at rest. Loss of vagal tone (e.g., cardiac vagotomy) increases resting heart rate from ~70 to ~160 bpm
- Vasovagal syncope: sudden, excessive vagal discharge causing profound bradycardia + vasodilation → loss of consciousness
- Carotid sinus massage: increases vagal tone deliberately - used to break certain supraventricular tachycardias
Sources:
- THIEME Atlas of General Anatomy & Musculoskeletal System, Sympathetic/Parasympathetic Synopsis table
- Histology: A Text and Atlas (Pawlina), Systemic Regulation of Heart Function
- Guyton & Hall Textbook of Medical Physiology, Bradycardia & Vagal Stimulation sections
- Lippincott Illustrated Reviews: Pharmacology, Muscarinic Receptors
What is the function of ciliary muscle
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Excellent - the textbooks give a thorough picture. Here is the complete answer:
Functions of the Ciliary Muscle
The ciliary muscle is smooth muscle forming the bulk of the ciliary body, located just posterior to the iris. It has three major functions:
1. Accommodation (Primary Function)
Accommodation = the ability to increase the refractive power of the eye to focus on near objects by changing the shape of the lens.
Mechanism:
| State | Ciliary Muscle | Zonular Fibers (Suspensory Ligaments) | Lens Shape | Vision |
|---|---|---|---|---|
| Near vision | Contracts (sphincter-like) | Relax (tension released) | Becomes more convex (rounder) | Near focus |
| Far/distant vision | Relaxes | Taut/tense | Becomes flatter | Far focus |
When the ciliary muscle contracts, it moves inward and forward, releasing tension on the zonular fibers attached to the lens. The elastic lens then bulges into a more convex shape, increasing its refractive power for near vision. When the muscle relaxes, zonular fibers pull the lens flat for distance vision.
- Innervation: Parasympathetic fibers via CN III (oculomotor nerve), relayed through the ciliary ganglion
- Receptor: M3 muscarinic receptors on ciliary smooth muscle
- Drugs that mimic this: pilocarpine, physostigmine
- Drugs that block this: atropine, cyclopentolate → cause cycloplegia (paralysis of accommodation)
Presbyopia: Accommodation progressively fails after age 40 and is nearly gone by age 60, because the lens hardens and loses elasticity - not because the muscle fails.
2. Aqueous Humor Drainage - Reduces Intraocular Pressure
Ciliary muscle contraction puts tension on the trabecular meshwork, opening its pores and facilitating outflow of aqueous humor into the canal of Schlemm. This reduces intraocular pressure.
- This is the mechanism by which pilocarpine (a muscarinic agonist) lowers IOP in open-angle glaucoma
- Atropine has the opposite effect - blocks ciliary contraction, impairs drainage, can raise IOP (dangerous in glaucoma patients)
3. Aqueous Humor Production (Ciliary Body - Epithelium)
While this is a function of the ciliary body epithelium (not the muscle itself), it is closely related:
- Beta-adrenoceptors on ciliary epithelium stimulate aqueous humor secretion
- Beta-blockers (e.g., timolol eye drops) reduce secretion and lower IOP - another treatment for glaucoma
Innervation Summary
Parasympathetic (CN III → ciliary ganglion → short ciliary nerves)
→ M3 receptors on ciliary muscle
→ Contraction → accommodation + ↓IOP (trabecular meshwork opening)
Sympathetic
→ β receptors on ciliary epithelium
→ Aqueous humor secretion
Clinical Relevance
| Condition/Drug | Effect on Ciliary Muscle |
|---|---|
| Atropine (cycloplegic) | Blocks M3 → paralyzes accommodation (cycloplegia); used for refraction in children, uveitis |
| Pilocarpine | Stimulates M3 → contracts ciliary muscle → lowers IOP; treats glaucoma |
| Organophosphate poisoning | Excess ACh → sustained ciliary contraction (cyclospasm) → fixed near vision |
| Presbyopia | Lens hardens with age → accommodation lost despite normal muscle |
| CN III palsy | Loss of parasympathetic input → accommodation fails + pupil dilates + ptosis + eye turns "down and out" |
Sources:
- Katzung's Basic & Clinical Pharmacology (16th ed.), Pharmacology of the Eye
- K.J. Lee's Essential Otolaryngology, The Globe
- Gray's Anatomy for Students, Cranial Nerves (CN III innervation table)
Does activation of parasympathetic causes passing stools
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Yes - parasympathetic activation is a key driver of defecation. Here is the full explanation straight from Guyton & Hall:
Parasympathetic Activation and Defecation
The Two Defecation Reflexes
Defecation is controlled by two coordinated reflexes - one intrinsic, one parasympathetic:
Reflex 1: Intrinsic Myenteric Defecation Reflex (weak on its own)
- Feces distend the rectal wall
- Afferent signals spread through the myenteric (Auerbach's) plexus
- Triggers peristaltic waves in the descending colon, sigmoid, and rectum
- Relaxes the internal anal sphincter via inhibitory myenteric signals
- By itself this reflex is relatively weak and cannot effectively cause defecation
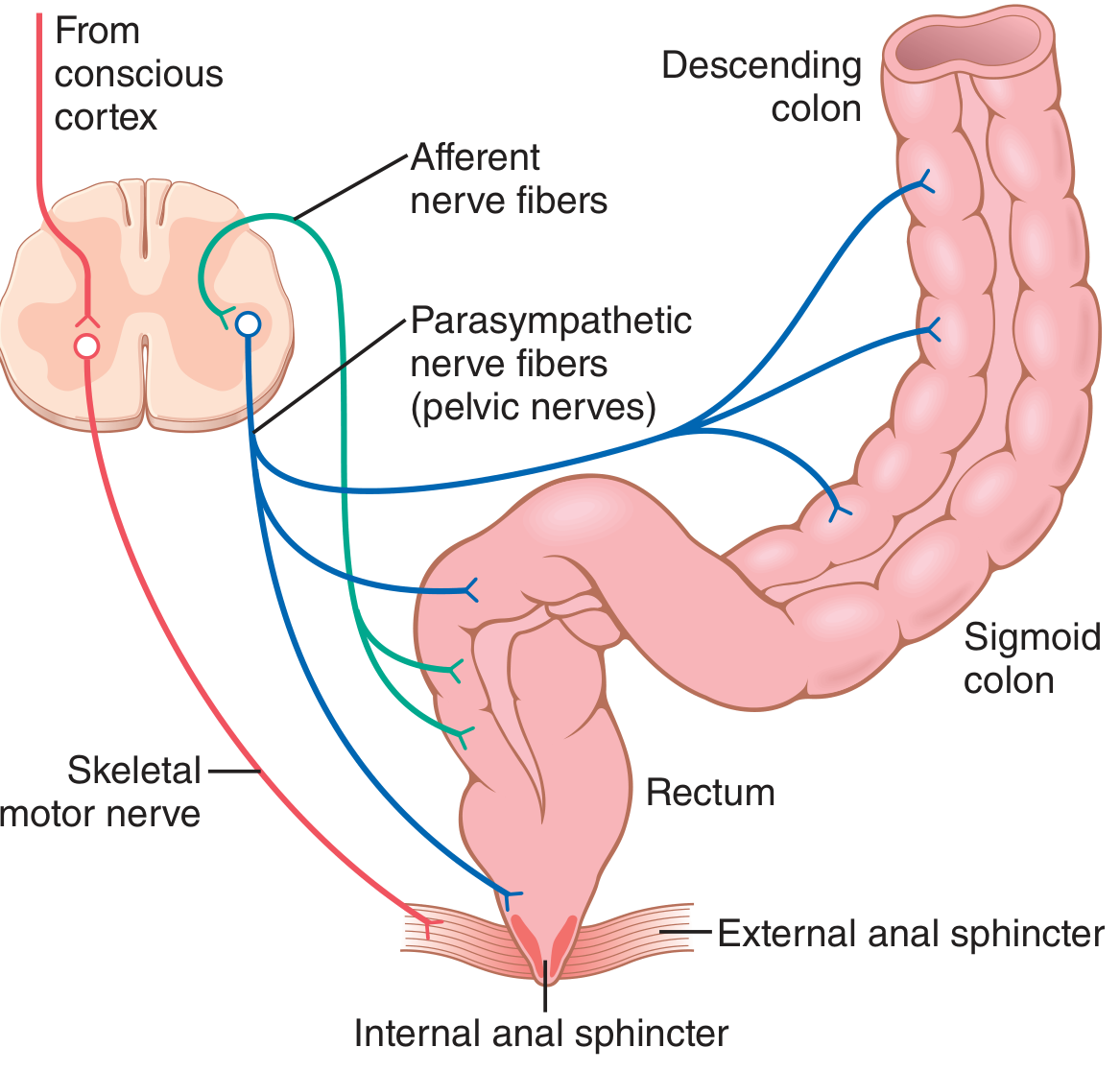
Reflex 2: Parasympathetic Defecation Reflex (the powerful amplifier)
- Rectal distension signals travel afferently to the sacral spinal cord (S2-S4)
- A reflex signal returns via parasympathetic fibers in the pelvic nerves to the descending colon, sigmoid, rectum, and anus
- These parasympathetic signals:
- Greatly intensify peristaltic waves
- Relax the internal anal sphincter
- Convert the weak intrinsic reflex into a powerful, effective defecation reflex
What Happens Step-by-Step
1. Mass movement pushes feces into rectum
↓
2. Rectal wall distension → urge to defecate
↓
3. Afferent signals → sacral spinal cord (S2-S4)
↓
4. Parasympathetic efferents via pelvic nerves
↓
5. Intensified peristalsis in descending colon, sigmoid, rectum
+ Relaxation of INTERNAL anal sphincter (smooth muscle, involuntary)
↓
6. Additional signals cause:
- Deep breath (diaphragm moves down)
- Glottis closure (Valsalva)
- Abdominal muscle contraction (↑intra-abdominal pressure)
- Pelvic floor relaxation
↓
7. If EXTERNAL anal sphincter (voluntary, somatic/pudendal nerve) is
consciously relaxed → DEFECATION occurs
The Two Sphincters - Key Distinction
| Sphincter | Type | Control | Parasympathetic Effect |
|---|---|---|---|
| Internal anal sphincter | Smooth muscle (involuntary) | Autonomic | Relaxed by parasympathetic → allows defecation |
| External anal sphincter | Skeletal muscle (voluntary) | Somatic (pudendal nerve, S2-S4) | Not directly controlled by parasympathetic - requires conscious voluntary relaxation |
Defecation requires both: parasympathetic relaxation of the internal sphincter AND voluntary relaxation of the external sphincter. This is why defecation can be consciously postponed even when the urge is strong.
Gastrocolic Reflex - Why You Feel the Urge After Eating
After a meal, stomach and duodenal distension triggers the gastrocolic reflex - transmitted via the autonomic nervous system - which initiates mass movements in the colon. This is why the urge to defecate commonly occurs after meals (especially breakfast). This reflex is abolished when extrinsic autonomic nerves to the colon are removed.
Clinical Relevance
| Condition | Mechanism |
|---|---|
| Spinal cord injury above sacral level | Lose voluntary control of external sphincter → automatic reflex emptying (reflex bowel) |
| Sacral cord injury (S2-S4) | Lose the parasympathetic defecation reflex → severe constipation, atonic bowel |
| Hirschsprung's disease | Absence of myenteric plexus in colon segment → no peristalsis, massive constipation |
| Anticholinergic drugs (atropine) | Block muscarinic receptors → decreased GI motility → constipation |
| Cholinomimetics (neostigmine, bethanechol) | Increase parasympathetic activity → increased motility → diarrhea/defecation |
| Habitual suppression of defecation urge | Weakens natural reflexes over time → chronic constipation |
In summary: Yes, parasympathetic activation is essential for defecation. The sacral parasympathetics (pelvic nerves, S2-S4) powerfully amplify the intrinsic myenteric reflex, intensify peristalsis, and relax the internal anal sphincter. The final step - relaxing the external sphincter - requires voluntary somatic control.
- Guyton & Hall Textbook of Medical Physiology, Chapter 64 - Defecation
This is a shared conversation. Sign in to Orris to start your own chat.