Enumerate Therapeutic uses & Side-effects of the following a) Fluoxetine (5 t Clomiphene citrate Interferon 2 =I0 Mark) avlet I9Metronidazole C. Sreptomycin
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have enough detailed information from all five drugs. Let me compile the comprehensive answer:
Therapeutic Uses and Side Effects of Five Drugs
a) Fluoxetine
Class: Selective Serotonin Reuptake Inhibitor (SSRI)
Mechanism: Potent, selective inhibitor of the serotonin transporter (SERT), blocking reuptake of 5-HT. Has minimal affinity for muscarinic (ACh), alpha-1 adrenergic (α1), and histamine (H1) receptors.
Therapeutic Uses
| Indication | Notes |
|---|---|
| Major Depressive Disorder (MDD) | First-line SSRI; effective in adults and adolescents |
| Obsessive-Compulsive Disorder (OCD) | FDA-approved |
| Bulimia Nervosa (BN) | 60 mg/day shown effective in multiple RCTs; reduces binge/purge episodes |
| Panic Disorder | Approved indication |
| Premenstrual Dysphoric Disorder (PMDD) | Approved as Sarafem |
| Bipolar Depression | Used in combination (e.g., with olanzapine - "Symbyax") |
| Binge Eating Disorder (BED) | Off-label use |
| Anxiety Disorders | Generalised anxiety, social phobia |
Side Effects
| System | Effects |
|---|---|
| GI | Nausea, diarrhea, dry mouth, anorexia (most common early effects) |
| CNS/Neurological | Headache, insomnia, nervousness, tremor, dizziness |
| Sexual | Decreased libido, anorgasmia, ejaculatory delay (common and dose-dependent) |
| Cardiovascular | QTc prolongation (mild), hypertension |
| Metabolic | Weight loss initially; weight gain with long-term use |
| Serious | Serotonin syndrome (with MAOIs or serotonergic drugs), suicidality risk in adolescents (black box warning), hyponatremia (SIADH), bleeding risk (inhibits platelet serotonin) |
| Discontinuation | Long half-life (48-72 h parent; 180 h for active metabolite norfluoxetine) means less discontinuation syndrome vs other SSRIs |
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
b) Clomiphene Citrate
Class: Selective Estrogen Receptor Modulator (SERM) - triphenylethylene derivative
Mechanism: Acts as an estrogen antagonist at the hypothalamus - blocks estrogen negative feedback - increases GnRH pulsatility - raises FSH/LH - induces ovulation. The two isomers: enclomiphene (trans) = potent antagonist; zuclomiphene (cis) = weak agonist.
Therapeutic Uses
| Indication | Notes |
|---|---|
| Ovulation Induction | Primary use - anovulatory infertility (PCOS, hypothalamic-pituitary dysfunction, dysfunctional uterine bleeding) |
| Polycystic Ovary Syndrome (PCOS) | First-line agent for ovulation induction (though letrozole now preferred by many guidelines) |
| Amenorrhoea with anovulation | Induction of ovulatory cycles |
| Male hypogonadism / oligospermia | Off-label use - increases testosterone production |
| Luteal phase defect | Augments LH surge and progesterone production |
Side Effects
| Category | Effects |
|---|---|
| Vasomotor | Hot flushes/flashes (most common) |
| Ovarian | Ovarian enlargement, ovarian hyperstimulation syndrome (OHSS) - though milder than with gonadotropins |
| Visual | Blurred vision, scotomas, photophobia (indication to STOP treatment promptly) |
| Multiple Pregnancy | ~8% rate, majority twins |
| Anti-estrogenic effects | Cervical mucus thickening (reduces sperm penetration), thin endometrium |
| GI | Nausea, bloating, abdominal discomfort |
| Mood | Mood swings, depression, irritability |
| Rare | Alopecia |
- Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th Ed.
- Berek & Novak's Gynecology
c) Interferons
Classes: IFN-α (alfa), IFN-β (beta), IFN-γ (gamma)
Mechanism: Bind cell-surface receptors → induce host cell enzymes that inhibit viral RNA translation → degradation of viral mRNA and tRNA. Also have immunomodulatory and antiproliferative effects.
Therapeutic Uses
| Interferon Type | Approved Indications |
|---|---|
| IFN-α (Peginterferon alfa-2a/2b) | Chronic Hepatitis B (preferred agent), Chronic Hepatitis C (in combination, though largely superseded by DAAs), Hairy cell leukaemia, Chronic myelogenous leukaemia (CML), Kaposi sarcoma, Condylomata acuminata (genital warts - HPV) |
| IFN-β (beta-1a, beta-1b) | Relapsing-remitting Multiple Sclerosis (reduces relapse rate) |
| IFN-γ | Chronic Granulomatous Disease (CGD) - reduces infection frequency |
Side Effects
| System | Effects |
|---|---|
| Flu-like symptoms | Fever, chills, myalgias, arthralgias, fatigue (very common, especially early in therapy) |
| GI | Nausea, vomiting, diarrhea, anorexia |
| Haematological | Bone marrow suppression: neutropaenia, thrombocytopaenia, anaemia (principal dose-limiting toxicity) |
| Neurological/Psychiatric | Fatigue, somnolence, behavioural disturbances, depression (common and potentially severe) |
| Endocrine | Autoimmune thyroiditis, hypothyroidism/hyperthyroidism |
| Cardiovascular | Rarely - cardiomyopathy, heart failure |
| Metabolic | Severe weight loss |
| Injection site | Local reactions (induration, erythema) |
- Lippincott Illustrated Reviews: Pharmacology
- Goodman & Gilman's Pharmacological Basis of Therapeutics
d) Metronidazole
Class: 5-Nitroimidazole
Mechanism: Prodrug - requires reductive activation of its nitro group by anaerobic/microaerophilic organisms. The activated nitro radical anion causes radical-mediated DNA strand breaks → cell death. Active only in low-oxygen environments.
Therapeutic Uses
| Category | Specific Uses |
|---|---|
| Protozoal infections | Trichomoniasis (2 g single oral dose), Amoebiasis (intestinal + amoebic liver abscess - drug of choice), Giardiasis |
| Anaerobic bacterial infections | Bacteroides fragilis, Clostridium spp., anaerobic gram-negative bacilli - intra-abdominal sepsis, pelvic inflammatory disease |
| Clostridium difficile (CDI) | Historically first-line for mild CDI (now superseded by vancomycin in severe disease) |
| H. pylori eradication | Component of triple/quadruple therapy (e.g., PPI + amoxicillin + metronidazole ± bismuth) |
| Surgical prophylaxis | Pre-operative bowel preparation |
| Bacterial vaginosis | Oral or topical |
| Dental infections | Anaerobic oral flora |
Side Effects
| System | Effects |
|---|---|
| GI | Nausea, vomiting, metallic taste (very characteristic), dry mouth, anorexia, abdominal cramps |
| CNS | Headache, dizziness, vertigo, rarely encephalopathy, convulsions, ataxia, incoordination |
| Peripheral nervous system | Peripheral neuropathy, paraesthesia, numbness (with prolonged use - warrants discontinuation) |
| Urinary | Dysuria, cystitis, darkening of urine |
| Skin | Urticaria, flushing, pruritus; rare Stevens-Johnson syndrome |
| Disulfiram-like reaction | Flushing, vomiting, headache if alcohol is consumed during or within 3 days of therapy |
| Drug interactions | Potentiates warfarin (prolongs PT), interacts with disulfiram (psychosis), may precipitate lithium toxicity, CNS toxicity in CNS disease |
| Pregnancy | Avoid in 1st trimester |
- Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th Ed.
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
e) Streptomycin
Class: Aminoglycoside antibiotic (first aminoglycoside - isolated from Streptomyces griseus)
Mechanism: Binds irreversibly to the 30S ribosomal subunit (P12 protein) → misreading of mRNA → faulty protein synthesis → bactericidal. Active against extracellular, rapidly dividing bacilli.
Therapeutic Uses
| Category | Specific Uses |
|---|---|
| Tuberculosis (TB) | Second-line agent; used in drug-resistant TB (MDR-TB) or when first-line agents cannot be used. Effective against rapidly multiplying extracellular bacilli; ineffective against persisters. Given IM/IV, 15 mg/kg/day (max 1 g/day), always in combination. |
| Plague | (Yersinia pestis) - drug of choice, 1 g twice daily IM + oral tetracycline |
| Tularemia | (Francisella tularensis) - drug of choice, 1-2 g/day IM for 10-14 days |
| Brucellosis | In combination with doxycycline |
| Endocarditis | Penicillin + streptomycin for enterococcal endocarditis; streptomycin used for gentamicin-resistant enterococcal strains |
| Viridans streptococcal endocarditis | 2-week penicillin + streptomycin regimen |
Side Effects
| System | Effects |
|---|---|
| Vestibulotoxicity | The most serious toxicity - vertigo, nystagmus, loss of balance (targets vestibular apparatus preferentially over auditory); frequency proportional to patient age and blood levels |
| Ototoxicity | Auditory damage (deafness) - less common than vestibular damage with streptomycin; kanamycin and neomycin more cochleotoxic |
| Nephrotoxicity | Tubular damage - less common with streptomycin than gentamicin/tobramycin |
| Neuromuscular blockade | Rare - inhibits acetylcholine release and blocks nicotinic receptors; risk at high doses |
| Hypersensitivity | Fever, skin rashes, urticaria - more frequent with prolonged courses (e.g., TB treatment) |
| Injection site | Pain at IM injection site |
| Foetal risk | Ototoxicity reported in neonates of mothers treated with streptomycin during pregnancy (causes fetal harm) |
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
- Park's Textbook of Preventive and Social Medicine
Quick Summary Table
| Drug | Main Use(s) | Key/Characteristic Side Effect |
|---|---|---|
| Fluoxetine | Depression, OCD, Bulimia, Panic disorder | Sexual dysfunction, serotonin syndrome, long t½ |
| Clomiphene citrate | Anovulatory infertility, PCOS | Hot flushes, visual disturbances, multiple pregnancy |
| Interferon | Hepatitis B/C, CML, MS, CGD | Flu-like symptoms, depression, bone marrow suppression |
| Metronidazole | Trichomoniasis, Amebiasis, Anaerobic infections | Metallic taste, peripheral neuropathy, disulfiram-like reaction with alcohol |
| Streptomycin | TB (2nd line), Plague, Tularemia, Endocarditis | Vestibulotoxicity (vertigo/ataxia), ototoxicity, nephrotoxicity |
Mechanism of action, uses & side-effects ofValproic acid.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data. Here is the full answer:
Valproic Acid (Valproate / Sodium Valproate)
Chemical nature: n-Dipropylacetic acid - a short-chain branched fatty acid. The active form at body pH is the valproate ion. Formulations include valproic acid capsules/syrup, sodium valproate, and divalproex sodium (a coordination complex of equal parts valproic acid + sodium valproate).
I. Mechanism of Action
Valproic acid has broad-spectrum antiseizure activity and its exact mechanism is not fully established. It acts via at least three complementary pathways:
1. Blockade of Voltage-Sensitive Sodium Channels (VSSCs)
- Inhibits sustained repetitive neuronal firing by prolonging recovery of voltage-activated Na⁺ channels from their inactivated state
- Reduces excessive sodium influx → reduces excitatory (glutamatergic) neurotransmission
- This action parallels those of phenytoin and carbamazepine
2. Enhancement of GABAergic Inhibition
- Stimulates glutamic acid decarboxylase (GAD) - the enzyme that synthesizes GABA
- Inhibits GABA-transaminase (GABA-T) - the main GABA-degrading enzyme
- Inhibits succinic semialdehyde dehydrogenase - another enzyme in GABA catabolism
- Net result: ↑ GABA levels in the brain → enhanced inhibitory neurotransmission
3. Reduction of T-Type Calcium Currents
- Produces a small reduction of T-type Ca²⁺ currents in thalamic neurons (similar to ethosuximide)
- This action is thought to explain its efficacy against absence seizures (which depend on thalamo-cortical oscillatory circuits driven by T-type Ca²⁺)
4. Inhibition of Histone Deacetylase (HDAC)
- Valproate is a potent HDAC inhibitor → modulates gene expression via epigenetic mechanisms
- This may underlie some of its neuroprotective, mood-stabilizing, and anticancer properties
Summary Diagram (Stahl's Psychopharmacology):
"Valproic acid may work by interfering with voltage-sensitive sodium channels, enhancing the inhibitory actions of GABA, and regulating downstream signal transduction cascades."
II. Therapeutic Uses
A. Epilepsy (First-line broad-spectrum antiseizure drug)
| Seizure Type | Notes |
|---|---|
| Generalized tonic-clonic seizures | First-line; highly effective |
| Absence seizures | First-line (preferred over ethosuximide when patient also has tonic-clonic seizures) |
| Myoclonic seizures | Drug of choice for juvenile myoclonic epilepsy (JME) |
| Atonic seizures | Used in Lennox-Gastaut syndrome |
| Focal (partial) seizures | Effective, though carbamazepine/phenytoin may be superior for complex focal seizures |
| Status epilepticus | IV formulation available for acute management |
B. Bipolar Disorder (Mood Stabilizer)
- Acute mania: First-line agent; IV infusion can rapidly stabilize agitated behavior; comparable efficacy to lithium for mixed mania and rapid cycling
- Maintenance: Reduces frequency of manic and depressive episodes
- Bipolar depression: Less evidence but used
C. Migraine Prophylaxis
- Approved for prevention of migraine headaches; reduces frequency and severity
- Not used for acute treatment
D. Other (Off-label / Emerging)
- Neuropathic pain
- Schizoaffective disorder (adjunct)
- Post-traumatic stress disorder (PTSD)
- HDAC inhibition has prompted investigation in some cancers (e.g., cutaneous T-cell lymphoma)
III. Side Effects
A. Dose-Related (Common)
| System | Side Effect |
|---|---|
| GI | Nausea, vomiting, abdominal pain, heartburn, diarrhea (most common; mitigated by taking with food or using enteric-coated formulation) |
| CNS | Fine tremor (at higher levels), sedation, dizziness, ataxia |
| Metabolic | Weight gain, increased appetite |
| Hair | Transient hair loss (alopecia); hair may regrow curlier |
| Haematological | Thrombocytopaenia (idiosyncratic), platelet dysfunction |
| Ammonia | Hyperammonaemia → lethargy, encephalopathy (especially with urea cycle disorders - contraindicated in these patients) |
B. Idiosyncratic (Serious / Rare)
| Effect | Details |
|---|---|
| Hepatotoxicity | Most serious; potentially fatal hepatic failure. Risk greatest in children <2 years and those on polypharmacy. Most fatalities within first 4 months of therapy. Monitor LFTs. |
| Pancreatitis | Rare but life-threatening; can occur at any time in treatment |
| Thrombocytopaenia | Idiosyncratic; monitor platelet count |
C. Teratogenicity (Major Concern)
Valproate is highly teratogenic - it is the most teratogenic of all antiepileptic drugs.
| Risk | Detail |
|---|---|
| Neural tube defects | 1-2% risk (spina bifida, anencephaly) - first trimester exposure |
| Cardiovascular malformations | Atrial/ventricular septal defects |
| Orofacial clefts | Cleft lip/palate |
| Digital/limb anomalies | |
| Cognitive impairment | Children exposed in utero have lower IQ scores; learning disabilities |
| Fetal valproate syndrome | Distinctive facial features + developmental delay |
Avoid in women of childbearing age wherever possible. Folic acid supplementation is essential if used.
D. Drug Interactions
| Interaction | Effect |
|---|---|
| Phenobarbital | Valproate inhibits phenobarbital metabolism → ↑ phenobarbital levels → stupor/coma |
| Phenytoin | Displaces phenytoin from plasma proteins → ↑ free phenytoin → toxicity |
| Lamotrigine | Valproate dramatically reduces lamotrigine clearance (2-3× prolonged t½) → lamotrigine toxicity; require halving of lamotrigine dose |
| Carbamazepine | ↑ carbamazepine epoxide (toxic metabolite) levels |
| Warfarin | Displacement from protein binding → ↑ anticoagulant effect |
Quick Reference Summary
| Property | Detail |
|---|---|
| Class | Short-chain branched fatty acid / Broad-spectrum AED + Mood stabilizer |
| MOA | Na⁺ channel blockade + ↑ GABA (GAD activation + GABA-T inhibition) + ↓ T-type Ca²⁺ + HDAC inhibition |
| Main uses | All seizure types, Bipolar mania/prophylaxis, Migraine prophylaxis |
| Characteristic side effects | GI distress, tremor, weight gain, alopecia |
| Serious toxicity | Fatal hepatotoxicity (esp. <2 yr), pancreatitis, teratogenicity |
| Contraindications | Urea cycle disorders, hepatic disease, pregnancy (relative) |
| Therapeutic range | 50-100 mcg/mL (up to 150 mcg/mL in some cases) |
- Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th Ed.
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
- Stahl's Essential Psychopharmacology, 5th Ed.
Glutamate
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - rich content retrieved. Now I have everything needed for a comprehensive answer.
Glutamate as a Neurotransmitter
1. Overview
Glutamate (glutamic acid) is the principal excitatory neurotransmitter in the CNS. Key facts:
- Mediates fast excitatory neurotransmission at ~80% of all brain synapses, particularly those innervating dendritic spines
- Brain concentration is 10 mM - the highest of all amino acids; ~20% of this constitutes the neurotransmitter pool
- Repolarization of membranes after glutamatergic depolarization accounts for up to 80% of the brain's total energy expenditure
- Virtually every neuron in the CNS is innervated by glutamatergic neurons
2. Synthesis
Glutamate cannot cross the blood-brain barrier - it must be synthesised de novo inside the CNS:
Primary pathway:
Glucose → TCA cycle → α-Ketoglutarate → (transamination) → Glutamate
The Glutamine Cycle (Glutamate-Glutamine Cycle):
This is the dominant recycling pathway, accounting for ~40% of brain glutamate turnover:
Presynaptic terminal Astrocyte (glia)
Glutamate → released into synapse
↓ taken up by EAAT1/EAAT2
Glutamate
↓ Glutamine synthetase (ATP-dependent, glia only)
Glutamine → released to neuron
↓ Phosphate-activated glutaminase (mitochondrial)
Glutamate ← recycled
- Astrocytes (not neurons) express the reuptake transporters EAAT1 and EAAT2 that clear glutamate from the synapse
- Glutamine synthetase is expressed only in glia - neurons lack it
- This astrocyte-neuron metabolic cooperation is called the glutamate-glutamine shuttle
Storage: The neurotransmitter pool (~20%) is packaged into vesicles by the vesicular glutamate transporter (vGluT)
3. Glutamatergic Pathways in the Brain
| Pathway | Details |
|---|---|
| Primary sensory afferents | Retinal ganglion cells, cochlear cells, trigeminal nerve, spinal afferents - all glutamatergic |
| Thalamocortical projections | Distribute sensory information to cortex via glutamate |
| Corticolimbic pyramidal neurons | Major source of intrinsic, associational, and efferent cortical projections |
| Hippocampal circuit (memory) | Perforant path → Granule cells (dentate gyrus) → CA3 pyramidal cells → CA1 pyramidal cells (4 sequential glutamatergic synapses) |
| Climbing fibres | Cerebellar cortex - glutamatergic |
| Corticospinal tract | Glutamatergic |
4. Glutamate Receptors
Glutamate acts on two broad families of receptors:
A. Ionotropic Glutamate Receptors (iGluRs) — Fast Transmission
These are ligand-gated ion channels (tetramers). Three subtypes:
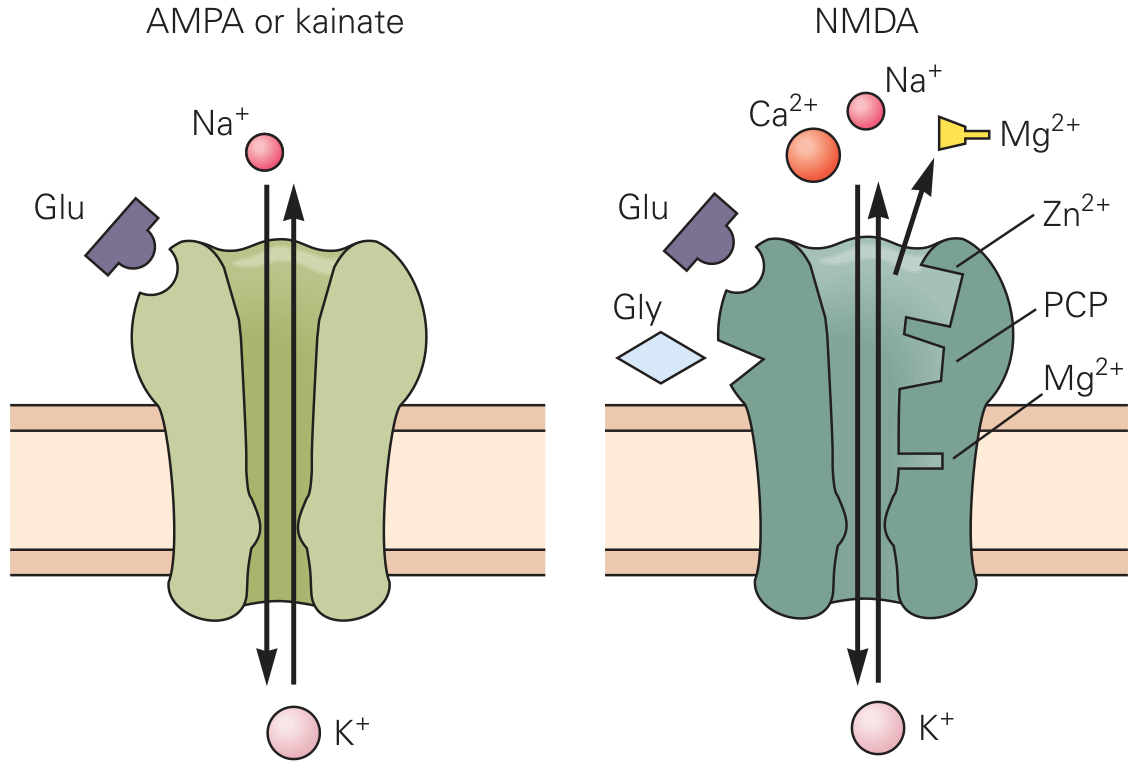
1) AMPA Receptors
| Property | Detail |
|---|---|
| Agonist | α-Amino-3-hydroxy-5-methylisoxazole-4-propionic acid (AMPA) |
| Subunits | GluR1–GluR4 (4 subunits); tetramers |
| Ion permeability | Na⁺ and K⁺ primarily; GluR2 subunit restricts Ca²⁺ entry (via Q/R editing: Arg at position 607 of GluR2 blocks Ca²⁺) |
| Function | Mediate the fast EPSP (excitatory postsynaptic potential); primary mediators of fast excitatory transmission |
| Antagonist | CNQX (6-cyano-7-nitroquinoxaline-2,3-dione) |
| LTP/LTD | Trafficking of AMPA receptors into/out of the postsynaptic membrane underlies long-term potentiation (LTP) and long-term depression (LTD) |
2) Kainate Receptors
| Property | Detail |
|---|---|
| Subunits | GluR5–GluR7, KA1, KA2 (5 subunits) |
| Ion permeability | Na⁺ and K⁺ |
| Location | Presynaptically on glutamatergic terminals (auto-receptors) |
| Function | Reduce glutamatergic neurotransmission when activated (negative feedback); role less defined than AMPA |
| Antagonist | CNQX |
3) NMDA Receptors (Most complex and clinically important)
| Property | Detail |
|---|---|
| Agonist | N-Methyl-D-aspartate (NMDA) |
| Subunits | NR1 (channel-forming) + NR2A-D (glutamate-binding); 7 genes |
| Ion permeability | Ca²⁺, Na⁺, K⁺ - highly Ca²⁺ permeable |
| Antagonist | APV (2-amino-5-phosphonovaleric acid); MK-801; Phencyclidine (PCP); Ketamine; Mg²⁺ (voltage-dependent) |
Unique features of the NMDA receptor - it is a "coincidence detector":
Three conditions must be met simultaneously for the channel to open:
- Glutamate binds to the NR2 subunit
- Glycine or D-serine binds to the glycine modulatory site (GMS) on NR1 (co-agonist; mandatory)
- Membrane depolarisation sufficient to expel the Mg²⁺ block from within the channel (provided by prior AMPA activation)
This triple requirement makes NMDA receptors act as molecular coincidence detectors - they only activate when both presynaptic and postsynaptic neurons are simultaneously active. This is the cellular basis of Hebbian learning ("neurons that fire together, wire together").
D-Serine is the dominant co-agonist in the forebrain - synthesised in the postsynaptic spine and released as an autocrine signal to prime NMDA receptors.
B. Metabotropic Glutamate Receptors (mGluRs) — Modulatory
| Property | Detail |
|---|---|
| Type | G protein-coupled receptors (GPCRs) |
| Groups | Group I (mGluR1, 5) - postsynaptic, Gq-coupled → ↑IP₃/DAG → ↑Ca²⁺; Group II (mGluR2, 3) - presynaptic auto-receptors, Gi-coupled → ↓cAMP; Group III (mGluR4, 6, 7, 8) - presynaptic, Gi-coupled → ↓cAMP |
| Function | Primarily modulate (fine-tune) glutamatergic and GABAergic transmission; do not mediate fast EPSPs |
| Agonist | ACPD (trans-1-amino-1,3-cyclopentanedicarboxylic acid) |
5. Synaptic Transmission Sequence
1. Action potential arrives at presynaptic terminal
2. Voltage-gated Ca²⁺ channels open → Ca²⁺ influx
3. Glutamate-containing vesicles fuse with membrane → glutamate released into cleft
4. Glutamate binds AMPA receptors → rapid Na⁺ influx → EPSP (fast depolarisation)
5. If depolarisation sufficient → Mg²⁺ expelled from NMDA channel
6. Glutamate + D-serine bind NMDA receptor → Ca²⁺ influx (slower, sustained)
7. Ca²⁺ activates kinases (CaMKII, PKC) → LTP, gene expression, synaptic plasticity
8. Glutamate cleared by astrocytic EAAT1/EAAT2 → converted to glutamine → recycled
6. Role in Synaptic Plasticity
| Process | Mechanism |
|---|---|
| Long-Term Potentiation (LTP) | ↑ AMPA receptors inserted into postsynaptic membrane (via PSD-95 scaffold expansion) + NMDA-dependent Ca²⁺ signalling → CaMKII activation |
| Long-Term Depression (LTD) | ↓ AMPA receptors removed from postsynaptic membrane (PSD-95 scaffold shrinks) |
| Memory formation | LTP at hippocampal synapses (CA3→CA1 Schaffer collaterals) is the leading cellular model of learning and memory |
AMPA receptor trafficking is continuous: half the synaptic AMPA receptors are replaced every ~15 minutes. LTP/LTD disrupt this equilibrium to strengthen or weaken synapses.
7. Clinical Relevance
| Condition | Glutamate's Role |
|---|---|
| Excitotoxicity | Excess glutamate (stroke, trauma, hypoxia) → sustained NMDA activation → massive Ca²⁺ influx → mitochondrial dysfunction, free radical generation, neuronal death |
| Epilepsy | Excessive glutamatergic excitation; AMPA receptor autoantibodies (anti-GluA3) can cause seizures; NMDA antagonists have antiseizure properties |
| Schizophrenia | NMDA receptor hypofunction hypothesis: NMDA blockade (by PCP/ketamine) mimics positive and negative symptoms of schizophrenia; GWAS data link glutamate pathway genes to schizophrenia risk |
| Alzheimer's Disease | Tonic NMDA activation by low-level glutamate leak → synaptic noise → memantine (NMDA antagonist) used therapeutically |
| Depression | Ketamine (NMDA antagonist) produces rapid antidepressant effects; glutamate dysregulation implicated in MDD |
| Bipolar disorder | Glutamatergic hyperactivity; valproate and lithium modulate NMDA/glutamate signalling |
| ALS / Stroke | Motor neuron loss and ischaemic neuronal death involve excitotoxic glutamate mechanisms |
8. Summary Diagram of Receptor Types
| Receptor | Type | Ions | Speed | Key Feature |
|---|---|---|---|---|
| AMPA | iGluR | Na⁺, K⁺ | Fast | Mediates EPSP |
| Kainate | iGluR | Na⁺, K⁺ | Fast | Presynaptic auto-receptor |
| NMDA | iGluR | Ca²⁺, Na⁺, K⁺ | Slower | Needs Glu + Gly/D-Ser + depolarisation; coincidence detector; LTP/learning |
| mGluR (Gp I) | mGluR (Gq) | — | Slow | Postsynaptic; ↑Ca²⁺ via IP₃ |
| mGluR (Gp II/III) | mGluR (Gi) | — | Slow | Presynaptic; ↓glutamate release (auto-inhibition) |
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- Eric Kandel's Principles of Neural Science, 6th Ed.
- Neuroscience: Exploring the Brain, 5th Ed.
- Stahl's Essential Psychopharmacology, 5th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.