Rhegmatogenous retinal detachment for 15 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive 15-mark answer. Let me compile it.
Rhegmatogenous Retinal Detachment (RRD)
Definition
Rhegmatogenous retinal detachment (from Greek rhegma = rent/break) is a separation of the neurosensory retina from the retinal pigment epithelium (RPE) through a full-thickness break in the retina, allowing liquefied vitreous to accumulate in the subretinal space.
Epidemiology & Pathogenesis
- Incidence: ~1 in 10,000 per year; bilateral involvement in ~10% of cases
- Pathogenetic triad: retinal break + vitreous liquefaction (syneresis) + vitreoretinal traction
- RD almost never occurs if vitreous is not at least partially liquefied and traction is absent
- >40% of RDs occur in myopic eyes — high myopia causes vitreous degeneration, PVD, and lattice/snailtrack degeneration more commonly
- Highly myopic eyes also face risk from round holes in chorioretinal atrophy and macular holes
- Vitreous loss at cataract surgery and Nd:YAG laser capsulotomy also increase risk
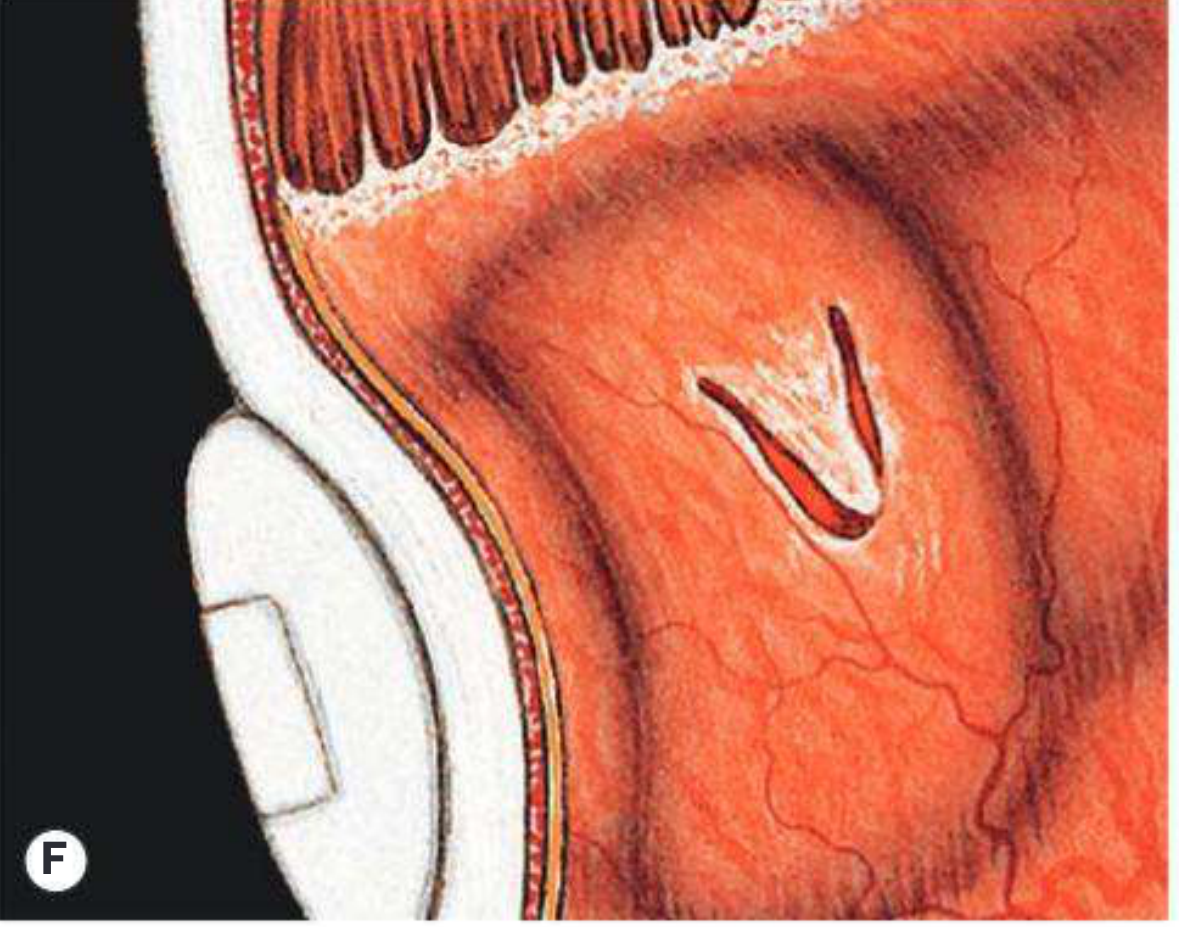
Types of Retinal Breaks
| Type | Mechanism | Features |
|---|---|---|
| U-tear / horseshoe tear | Dynamic vitreoretinal traction during PVD | Flap remains attached anteriorly; most common cause of RRD |
| Round/oval hole | Atrophic degeneration (no traction) | Common in lattice degeneration, young myopes |
| Dialysis | Avulsion at ora serrata | Post-traumatic; slow-spreading inferior RD |
| Giant tear | >90° circumferential break | Severe PVD; high risk of PVR |
Risk Factors
- High myopia
- Previous cataract surgery / aphakia / pseudophakia
- Lattice degeneration, snailtrack degeneration
- Blunt ocular trauma
- Fellow eye RD (contralateral RD risk ~10%)
- Family history
Distribution of Breaks
- ~60% superotemporal quadrant
- ~15% superonasal
- ~15% inferotemporal
- ~10% inferonasal
- ~50% of eyes with RD have more than one break, often within 90° of each other
Modified Lincoff's Rules (SRF Spread)
SRF spread is governed by gravity, anatomical limits (ora serrata, optic nerve), and the location of the primary break.
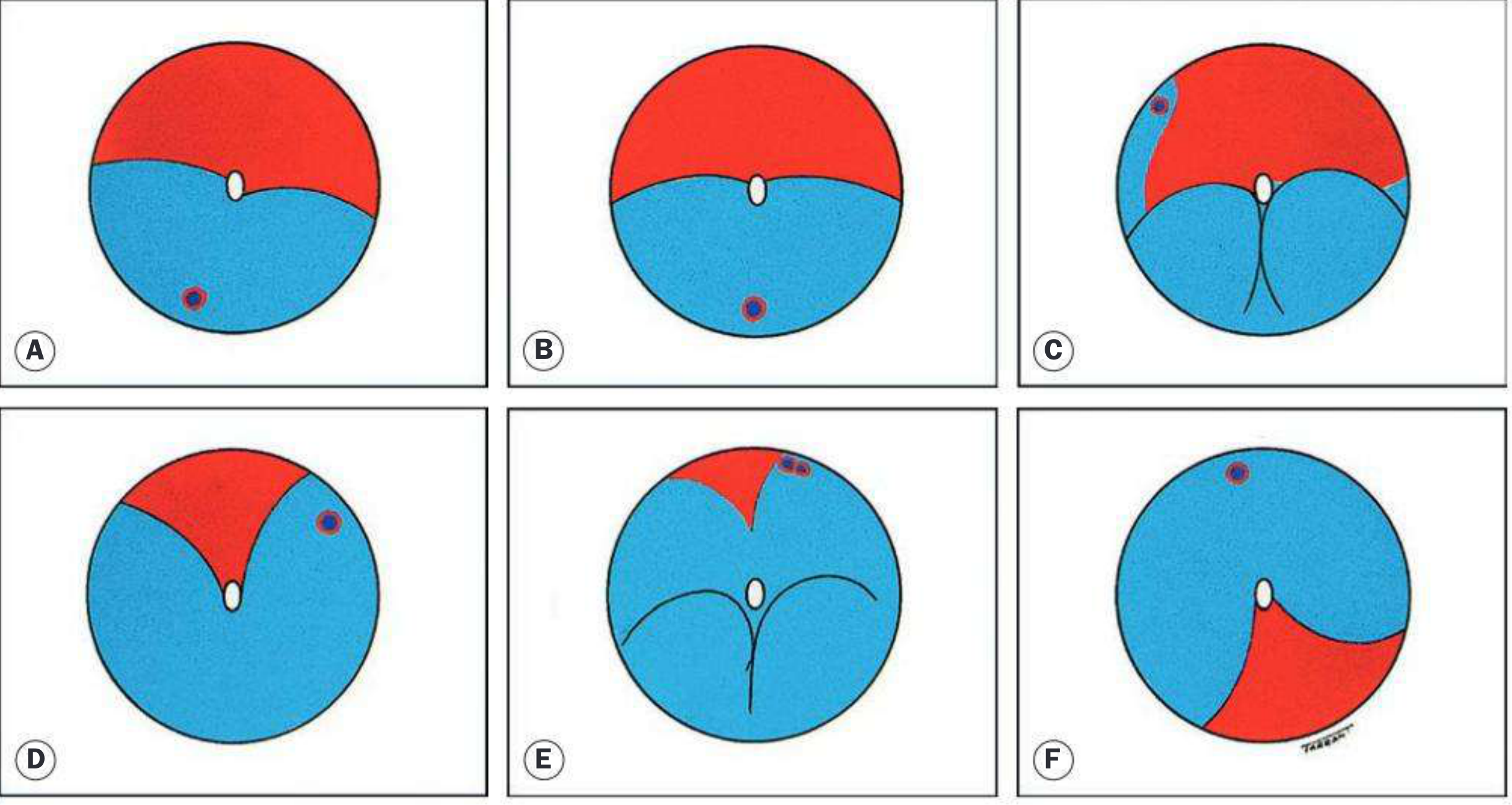
Key rules:
- Superior break → SRF spreads inferiorly on same side first, then superiorly opposite
- Inferior RD slightly higher on temporal side → break on that side inferiorly
- Break at 6 o'clock → equal fluid levels inferiorly
- Bullous inferior RD → primary break usually above horizontal meridian
- Subtotal RD with superior wedge of attached retina → break at periphery nearest its highest border
Symptoms
Classic premonitory symptoms occur in ~60% of patients with acute PVD:
- Photopsia (flashing lights) — due to vitreoretinal traction (location of photopsia does NOT predict break site)
- Floaters — due to PVD, vitreous condensation, or tobacco dust
- Curtain/shadow — relative peripheral visual field defect; appears in the quadrant opposite to the primary break
- Loss of central vision — if fovea involved by SRF, or by large bullous RD
- A lower field defect is appreciated more quickly than an upper defect
The quadrant of the field defect first appearing is opposite to the primary break location.
Signs
General
- Relative afferent pupillary defect (RAPD/Marcus Gunn pupil) — in extensive RD
- Low IOP (~5 mmHg lower than fellow eye) — characteristic
- Very low IOP + associated choroidal detachment
- Raised IOP → Schwartz-Matsuo syndrome (RRD + apparent uveitis, often dialysis from blunt trauma; displaced photoreceptor outer segments clog trabecular meshwork — resolves after RD repair)
- 'Tobacco dust' (Shafer's sign) — pigment cells in anterior vitreous; highly specific for RRD
- Mild iritis — common; may mask underlying RD
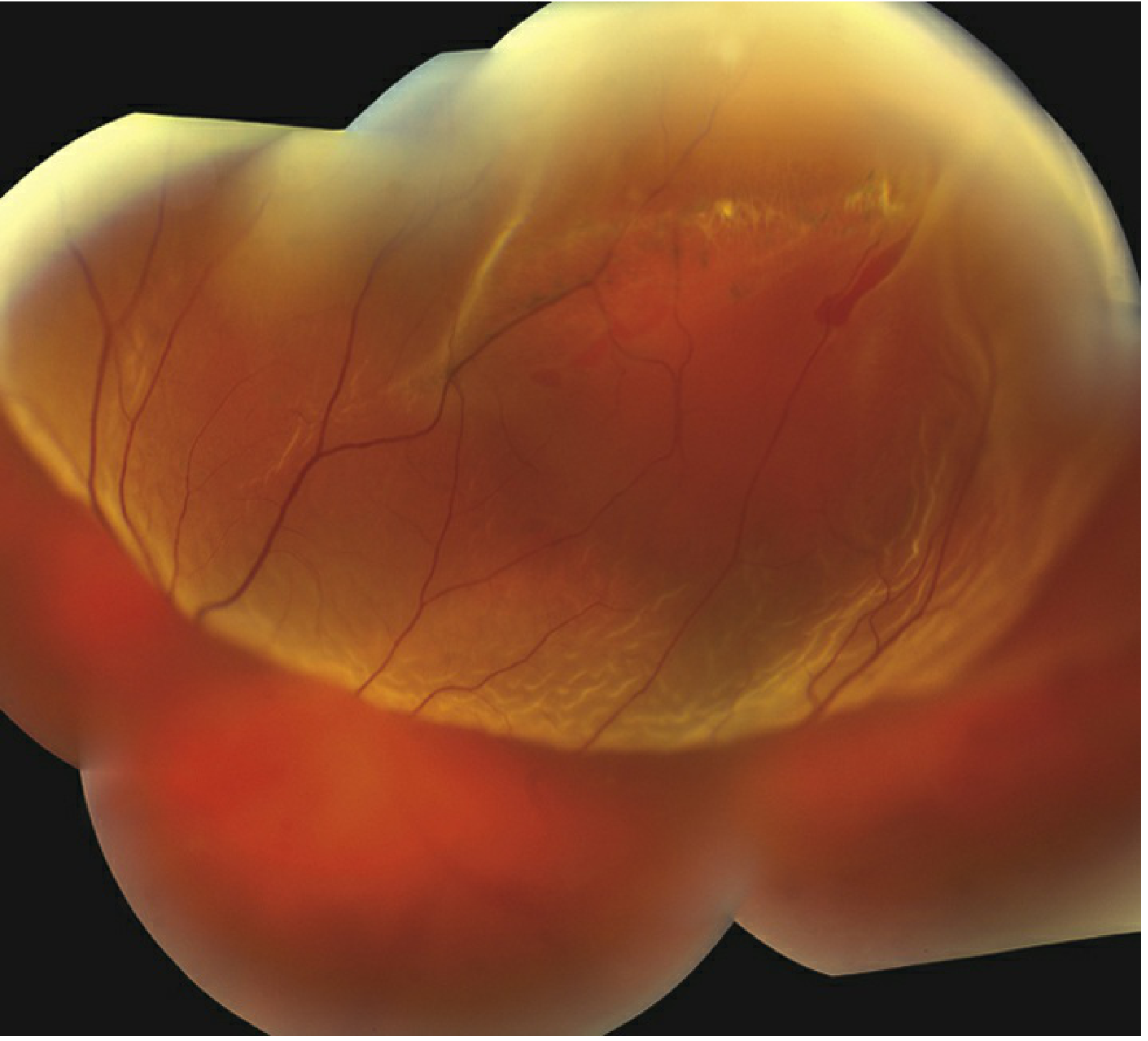
Fundus — Fresh RD
- Convex elevation of retina with slightly opaque, corrugated appearance (retinal oedema)
- Loss of underlying choroidal pattern
- Retinal blood vessels appear darker than in flat retina
- SRF extends to ora serrata
- B-scan US: good mobility of retina and vitreous
Fundus — Longstanding RD
- Retinal thinning (atrophy)
- Intraretinal cysts — develop after ~1 year; resolve after reattachment
- Subretinal demarcation lines ('high-water marks' or 'tide marks') — RPE cell proliferation at junction of flat/detached retina; develop after ~3 months
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Retinoschisis | Smooth, dome-shaped, translucent; absolute field defect; normal choroidal vessels visible; no SRF shift |
| Choroidal detachment | Brown, smooth, immobile; extends anterior to ora serrata; limited posteriorly by vortex veins |
| Exudative RD | No break; SRF shifts with gravity; smooth convex surface |
| Tractional RD | Concave surface; no free SRF; no primary break (proliferative membranes) |
Complications
Proliferative Vitreoretinopathy (PVR)
- Main cause of surgical failure
- Epiretinal and subretinal membrane formation → tangential traction → fixed star-fold retinal folds
- Graded A (vitreous cells), B (retinal wrinkling), C (fixed folds)
- Usually follows surgery for RRD or penetrating injury
Workup
- Slit-lamp examination — assess anterior vitreous (tobacco dust), lens status, PVD
- Indirect ophthalmoscopy with scleral depression — entire periphery of both eyes; locate all breaks
- B-scan ultrasonography — when media opacities prevent fundal view (dense VH, dense cataract)
- OCT — identifies tractional membranes; distinguishes tractional component; assesses macular status
Treatment
Urgency
- Macula-on RD → emergency surgery (same day / next day) — visual prognosis significantly better
- Macula-off RD → urgent but not emergency; outcomes do not worsen if repaired within 7–10 days
- Macula-off chronic RD → repair within 1 week if possible
- Urgent surgery also needed for: superior or large break, high myopia (rapid SRF spread), vitreous haemorrhage with B-scan-confirmed RD
- Pre-operatively: minimise activity, bed-rest with break in the most dependent position
Surgical Options
1. Pneumatic Retinopexy
- Outpatient procedure
- Intravitreal gas bubble (SF₆ or C₃F₈) + cryotherapy/laser to seal break
- Advantages: minimally invasive, quick, office-based
- Limitations: success rates lower than scleral buckling
- Indication: uncomplicated RD with small break or breaks <2 clock hours in the upper two-thirds of peripheral retina
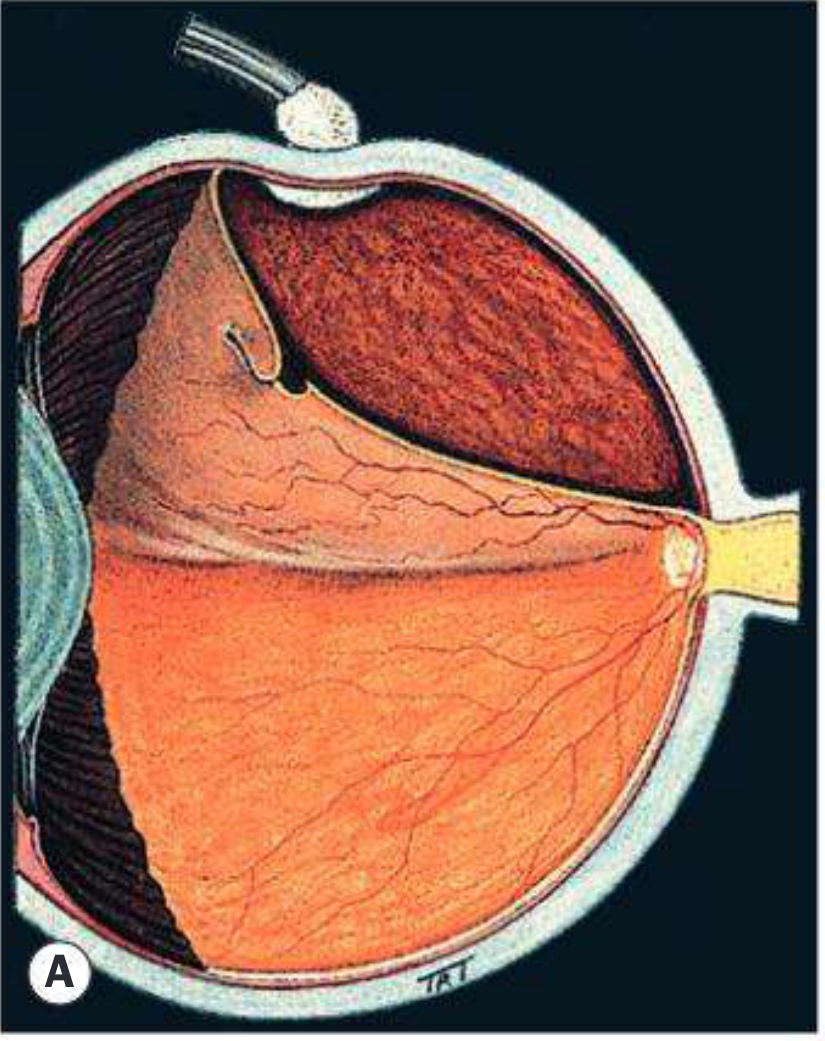
2. Scleral Buckling (Conventional/External)
- Silicone explant sutured onto sclera → inward indentation closes break by opposing RPE to neurosensory retina + reduces vitreoretinal traction
- Explant configurations: radial, segmental, circumferential, or encircling (360° band)
- Technique: peritomy → localize breaks → cryotherapy → suture explant → check buckle-break relation; drain SRF if needed
- Always indicated for post-traumatic dialysis
3. Pars Plana Vitrectomy (PPV)
- Increasingly preferred; >80% of primary RD surgery in the USA uses PPV
- Indicated when:
- Breaks cannot be visualized (VH, dense media opacity, posterior capsule opacification)
- Breaks unlikely to be closed by buckle (giant tears, large posterior breaks, PVR)
- Endotamponade with gas (SF₆, C₃F₈) or silicone oil maintains retinal apposition
Prognosis
- Anatomical success rate >90% with modern surgery
- Visual outcome depends on macular status pre-operatively
- Macula-on: good visual prognosis
- Macula-off: visual recovery incomplete; better if repaired within 72 hours to 7–10 days
Follow-Up
Post-surgery review: 1 day → 1 week → 1 month → 2–3 months → every 6–12 months. All patients require examination of the fellow eye for predisposing lesions.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed., pp. 695–702; The Wills Eye Manual, 8th Ed., pp. 764–771
Principles of sclera buckling surgery and complications
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the content needed. Let me compile the comprehensive answer from the textbook material already retrieved (block5, lines 174–290+).
The key content I extracted covers:
- Principles (lines 174–232): definition, purpose, explants, configurations, technique, SRF drainage, adjuncts
- Surgical failure (lines 233–273): causes of failure with illustrations
- Complications (lines 242–290+): full list
Principles of Scleral Buckling Surgery & Complications
Definition & Rationale
Scleral buckling (SB) — also called conventional or external retinal detachment surgery — is a procedure in which a material (explant) is sutured onto the outer scleral surface to create an inward indentation (buckle) of the globe wall.
Two fundamental aims:
- Close retinal breaks by apposing the RPE to the detached neurosensory retina, eliminating the pathway for liquefied vitreous to enter the subretinal space
- Reduce dynamic vitreoretinal traction at sites of local vitreoretinal adhesion — preventing reopening of breaks
Scleral buckling must always be used for retinal detachment secondary to post-traumatic dialysis — Kanski's Clinical Ophthalmology, p. 701
The Explant
- Made from soft or hard silicone (sponge or solid)
- The entire break should be surrounded by ~2 mm of buckle
- The buckle must also cover the vitreous base anterior to the tear — to prevent subsequent reopening and anterior SRF leakage
- Break dimensions are estimated by comparing with the optic disc diameter
Buckle Configurations
| Configuration | Use |
|---|---|
| Radial (perpendicular to limbus) | Single U-tear; prevents fish-mouthing; used with radial explant (plomb) |
| Segmental (circumferential segment) | Small cluster of breaks in one quadrant |
| Circumferential (broad arc) | Multiple breaks in one or two quadrants |
| Encircling (360° band) | Multiple breaks in ≥2 quadrants, PVR, aphakic/pseudophakic RD, undetected breaks |
Surgical Technique (Step-by-Step)
Step 1 — Anaesthesia
Peribulbar or general anaesthesia.
Step 2 — Peritomy (Conjunctival Incision)
360° or limited peritomy to expose the sclera and allow access to all four quadrants. The rectus muscles are identified and, if needed, slung with sutures for globe control.
Step 3 — Localization of Breaks
The break is localized with indirect ophthalmoscopy and the sclera is marked with a diathermy pen under BIO guidance. Accurate localization is the most critical step.
Step 4 — Cryotherapy (Retinopexy)
Applied around the retinal break under BIO visualization — ice ball visible through retina confirms adequate application. Creates a chorioretinal adhesion that seals the break after retinal reattachment.
Step 5 — Suturing the Explant
- Mattress sutures placed in partial-thickness sclera
- Explant of appropriate dimensions oriented correctly (radial/circumferential) and sutured to sclera
- Position checked to confirm the buckle is correctly placed relative to the break
Step 6 — Drainage of Subretinal Fluid (SRF)
Optional but important decision:
| Drain SRF | Do Not Drain SRF |
|---|---|
| Very high IOP after buckle | Fresh, mobile RD |
| Longstanding RD with thick SRF | Young patient with mobile SRF |
| Inferior RD | Low operative risk acceptable |
| Suspected subretinal membranes |
Drainage technique: A sclerotomy is made over the area of deepest SRF; the choroid is perforated carefully. Risks include: choroidal haemorrhage, retinal incarceration, subretinal haemorrhage, and inadvertent perforation of the retina.
Step 7 — Intraocular Pressure Management
After drainage or a tight buckle, IOP may rise. Options:
- Anterior chamber paracentesis
- Intravitreal gas injection (also aids break closure)
Step 8 — Final Check
BIO used to confirm: (a) break is on the buckle, (b) retinal vascularity is preserved (patent central retinal artery), (c) IOP not critically raised.
Step 9 — Wound Closure
Conjunctiva re-approximated with absorbable sutures. Subconjunctival antibiotic and steroid injected.
Adjunctive Procedures
- Laser photocoagulation (photocoagulation retinopexy): Post-operatively when retina is flat; creates permanent chorioretinal adhesion
- Intravitreal gas (SF₆ or C₃F₈): Adjunct tamponade; patient positioned to keep gas against break
- Encircling band: Used when breaks are multiple, in multiple quadrants, or when PVR is present — reduces vitreoretinal traction globally
Causes of Surgical Failure
The common causes of failure (retina remains detached or re-detaches) are:
| Cause | Explanation |
|---|---|
| Break not on the buckle | Incorrect localization or buckle displacement |
| Undersized explant | Break extends beyond margins of buckle |
| New / missed breaks | Secondary breaks not identified pre-op |
| Fish-mouthing of U-tear | Radial folds at the edges of a U-tear keep it open — requires radial explant or gas tamponade |
| PVR | Epiretinal/subretinal membranes contract → fixed star-folds → re-detachment |
| Buckle slippage or extrusion | Explant migrates or erodes through conjunctiva |
Complications of Scleral Buckling
Intraoperative
| Complication | Notes |
|---|---|
| Choroidal haemorrhage | During SRF drainage; ranges from minor to expulsive |
| Retinal perforation | Needle or drainage site penetrates retina |
| Subretinal haemorrhage | From drainage; may spread under retina |
| Retinal incarceration | Retina drawn into drainage site |
| Vitreous loss | May occur if globe perforated |
Early Postoperative
| Complication | Notes |
|---|---|
| Raised IOP | From tight buckle, forward rotation of lens-iris diaphragm, or choroidal detachment; may require paracentesis |
| Choroidal detachment | From hypotony post-drainage; usually resolves spontaneously |
| Anterior segment ischaemia | From ischaemia of the anterior segment if >2 rectus muscles are disinserted; presents with corneal oedema, cells, flare, dilated episcleral vessels |
| Ocular motility disturbance / diplopia | Muscle scarring or displacement |
| Conjunctival wound dehiscence | Especially with 360° peritomy |
Late Postoperative
| Complication | Notes |
|---|---|
| Buckle extrusion / exposure | Explant erodes through conjunctiva; risk increased by infection, thin conjunctiva |
| Buckle infection | Requires explant removal in most cases |
| Induced refractive change | Encircling band increases axial length → myopic shift; may cause anisometropia |
| Strabismus / diplopia | Extraocular muscle restriction by explant; common with large or encircling buckles |
| Cataract | More common with encircling procedures + drainage |
| Epiretinal membrane (macular pucker) | Proliferative response on retinal surface post-repair |
| PVR (proliferative vitreoretinopathy) | Main late cause of failure; epiretinal membranes → star folds → re-detachment |
| Fish-mouthing | Radial folds at U-tear edges preventing closure |
| Macular pucker | Epiretinal membrane causing metamorphopsia |
| Retinal re-detachment | From new/missed breaks, PVR, or buckle failure |
| Subretinal fluid persistence | Chronic SRF may persist for months even with anatomical success |
Outcomes
- Anatomical success rate: ~85–90% with a single procedure
- Visual outcome depends on pre-operative macular status
- Encircling buckles carry a higher rate of myopic shift and motility disturbance than segmental buckles
- Success rate is lower if PVR is present pre-operatively
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed., pp. 700–704
This is a shared conversation. Sign in to Orris to start your own chat.