Explain diabetes
Reading File
Finding Sources
Searching PubMed
"diabetes mellitus"[MeSH Terms] AND "review"[pt]
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
I now have all the material needed for a comprehensive answer. Let me compose it.
Diabetes Mellitus
Diabetes mellitus (DM) is a group of metabolic diseases characterized by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both. It is one of the most common chronic diseases worldwide and a leading cause of cardiovascular disease, blindness, renal failure, and lower-limb amputation.
1. Normal Glucose Physiology (Baseline)
The plasma glucose is normally maintained between 60-150 mg/dL despite wide variations after meals and exercise. Glucose comes from three sources: dietary absorption, glycogenolysis, and gluconeogenesis. Insulin - secreted by pancreatic beta cells - is the key anabolic hormone that suppresses hepatic glucose production and promotes glucose uptake in muscle and fat. Counterregulatory hormones (glucagon, epinephrine, cortisol, growth hormone) oppose insulin and raise blood glucose when needed. - Rosen's Emergency Medicine, p. 2534
2. Classification
The ADA recognizes four major types. - Rosen's Emergency Medicine, p. 2535
| Type | Core Defect | Key Features |
|---|---|---|
| Type 1 DM | Autoimmune beta-cell destruction | Absolute insulin deficiency; ketosis-prone; autoantibodies present (85-90%) |
| Type 2 DM | Insulin resistance + relative insulin deficiency | Usually asymptomatic initially; associated with obesity; rare ketosis |
| Gestational DM | Similar to type 2 pathogenesis | Onset during pregnancy; screened at 24-28 weeks with 75-g OGTT |
| Secondary / Other | Beta-cell damage from external cause | Chronic pancreatitis, cystic fibrosis, drugs (steroids, antipsychotics) |
| Prediabetes | Early insulin resistance | FPG 110-125 mg/dL or HbA1c 5.7-6.4%; 1-5% progress to DM per year |
3. Pathophysiology
Type 1 DM
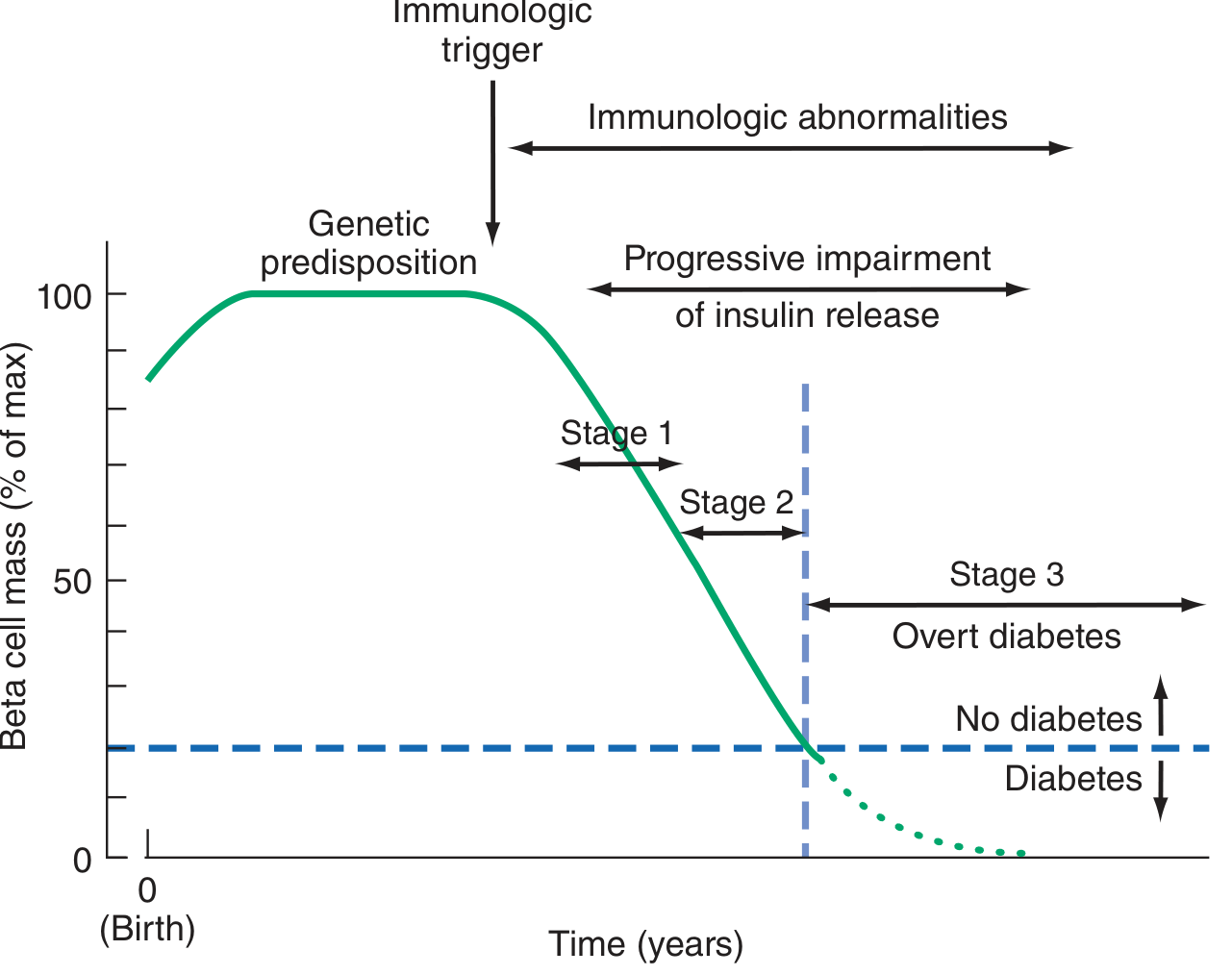
Type 1 DM results from the interaction of genetic, environmental, and immunologic factors leading to immune-mediated destruction of beta cells. Most patients have autoantibodies (islet cell antibodies, anti-GAD, anti-insulin, anti-IA-2). The disease is staged:
- Stage 1: Two or more autoantibodies present; normoglycemia
- Stage 2: Autoimmunity + dysglycemia
- Stage 3: Frank hyperglycemia meeting diagnostic criteria
A "honeymoon phase" may occur in the first 1-2 years after diagnosis when residual beta cells produce some insulin. Over time, insulin secretion disappears entirely. - Harrison's Principles of Internal Medicine 22e, p. 3243
Type 2 DM
Type 2 DM develops through a two-hit process:
- Insulin resistance - peripheral tissues (muscle, fat, liver) respond poorly to insulin. Increased insulin demand is compensated for years by beta-cell hypersecretion.
- Beta-cell failure - over time, beta cells become dysfunctional. First-phase insulin release is selectively impaired. Eventually, fasting hyperglycemia develops.
Obesity (especially abdominal) is the primary driver of insulin resistance. Mechanisms include defects in muscle glycogen synthesis, ectopic lipid accumulation in the pancreas and liver, and chronic low-grade inflammation. - Guyton & Hall Textbook of Medical Physiology
4. Diagnosis
| Test | Diagnostic Threshold |
|---|---|
| HbA1c | ≥ 6.5% (preferred confirmatory test) |
| Fasting plasma glucose | ≥ 126 mg/dL |
| 2-hour OGTT (75 g glucose) | ≥ 200 mg/dL |
| Random glucose + symptoms | ≥ 200 mg/dL |
- Rosen's Emergency Medicine, p. 2535
5. Clinical Features
Type 1: Acute onset, often dramatic - polyuria, polydipsia, weight loss, fatigue. Up to 25-50% of children present with diabetic ketoacidosis (DKA). - Harrison's, p. 3243
Type 2: Often asymptomatic for years. Many are diagnosed incidentally on routine bloodwork. Patients frequently have hypertriglyceridemia, hypertension, and central obesity (metabolic syndrome).
6. Long-Term Complications
Persistent hyperglycemia (glucotoxicity) causes damage through several mechanisms:
-
Advanced glycation end-products (AGEs) - form from glucose reacting with proteins; bind to RAGE receptors; trigger cytokine release (TGF-beta, VEGF), ROS generation, and procoagulant states
-
Protein kinase C activation - promotes VEGF-driven neovascularization (retinopathy) and TGF-beta-driven fibrosis (nephropathy)
-
Polyol pathway - aldose reductase converts excess glucose to sorbitol, depleting NADPH; damages nerves and lens
-
Robbins & Kumar Basic Pathology, p. 749
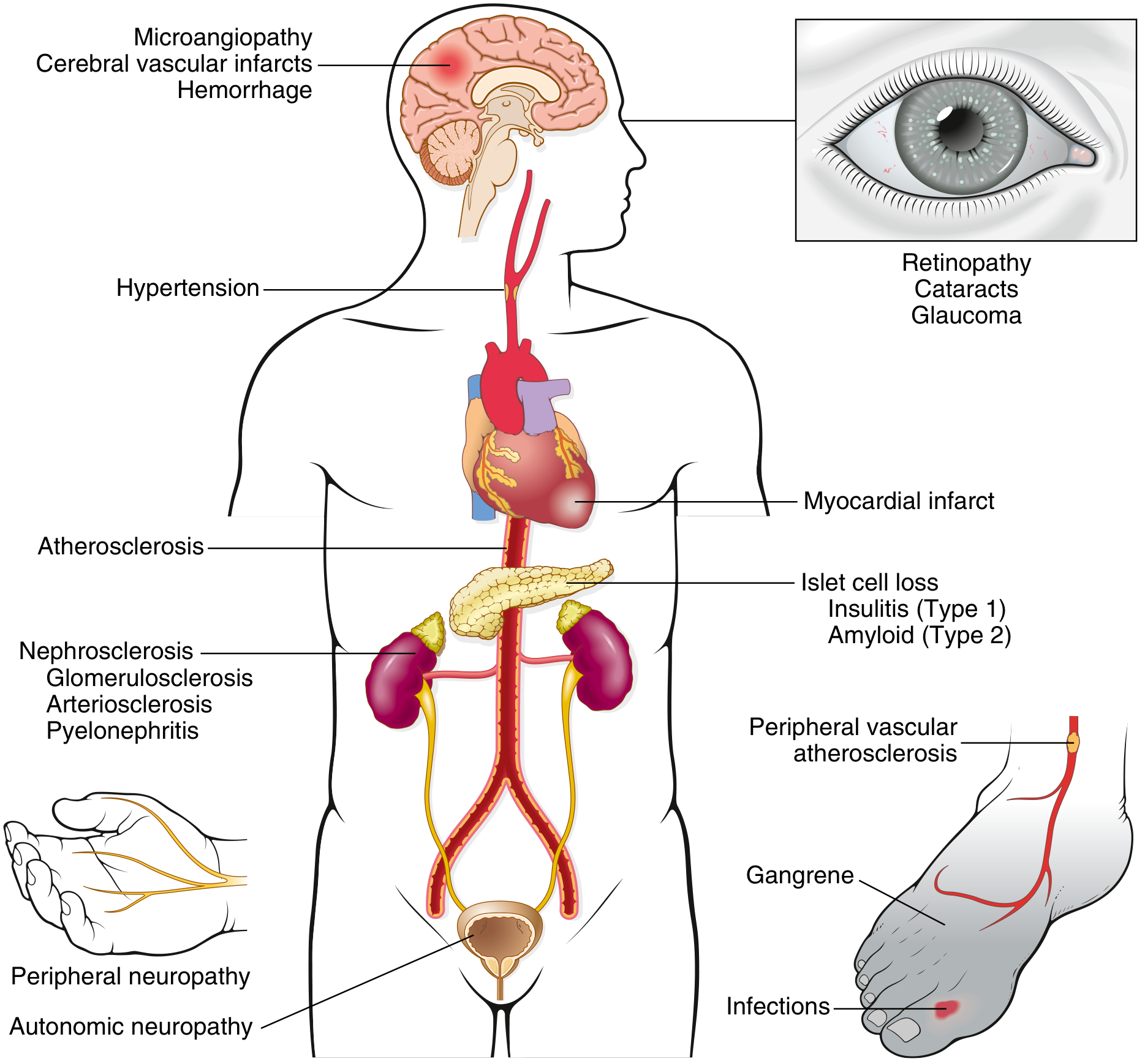
Microvascular Complications
- Diabetic retinopathy - proliferative scarring of the retina; leading cause of adult-onset blindness
- Diabetic nephropathy - glomerulosclerosis; leads to chronic kidney disease; associated with ~15-year reduction in life expectancy
- Diabetic neuropathy - distal symmetric polyneuropathy (burning/numbness in feet); autonomic neuropathy (gastroparesis, orthostatic hypotension, bladder dysfunction)
Macrovascular Complications
- Accelerated atherosclerosis of coronary, cerebral, and peripheral arteries
- 2-4x increased risk of MI and stroke
- Peripheral arterial disease - can progress to gangrene and amputation
7. Management
Type 1 DM
Insulin therapy is mandatory - the patient cannot survive without it. Regimens typically use basal insulin (long-acting) combined with bolus insulin (rapid-acting) at meals.
Type 2 DM
Treatment is stepwise - Guyton & Hall; Harrison's:
- Lifestyle modifications - caloric restriction, physical activity, weight loss (first-line for all patients)
- Metformin - suppresses hepatic glucose output; first-line drug; weight-neutral
- Sulfonylureas - stimulate pancreatic insulin release
- Thiazolidinediones (TZDs) - increase peripheral insulin sensitivity (PPAR-gamma agonists)
- GLP-1 receptor agonists (e.g., semaglutide, liraglutide) - enhance glucose-dependent insulin secretion + cause significant weight loss; also have cardiovascular benefits
- GIP/GLP-1 dual agonists (e.g., tirzepatide) - even greater reductions in weight and blood glucose
- SGLT2 inhibitors (e.g., empagliflozin) - block renal glucose reabsorption; have cardiorenal protective effects
- DPP-4 inhibitors - prolong endogenous incretin activity; modest glucose-lowering
- Insulin - required in later stages when beta-cell function is severely depleted
Monitoring & Targets
- Annual eye exams (retinopathy screening)
- Annual foot examination - assess pedal pulses, sensation (monofilament, vibration), reflexes
- Annual urine albumin-to-creatinine ratio (nephropathy)
- HbA1c target typically < 7% for most adults
- Blood pressure and lipid control are equally important - Harrison's, p. 3247
8. Special Situations
- Classification difficulty: Adults with new-onset type 1 DM are often misdiagnosed as type 2. Young age (<35), non-obese BMI, DKA, or personal/family history of autoimmunity should prompt testing for islet cell autoantibodies.
- Gestational DM: Screened at 24-28 weeks; resolves postpartum in most cases but increases lifetime risk of type 2 DM.
- Monogenic diabetes (MODY): Rare; consider in childhood/early adulthood onset with autosomal inheritance pattern and no autoimmune markers.
Recent Evidence Note
A 2025 meta-analysis of GLP-1 receptor agonists (99,599 patients, JACC) confirmed significant cardiovascular benefits in diabetic patients. A separate 2025 review in JAMA Ophthalmology flagged potential ocular adverse events with semaglutide (worsening diabetic retinopathy in some patients) - an important consideration when initiating GLP-1 therapy in patients with pre-existing retinopathy.
Sources: Harrison's Principles of Internal Medicine 22e | Rosen's Emergency Medicine | Robbins & Kumar Basic Pathology | Guyton & Hall Textbook of Medical Physiology | Basic Medical Biochemistry (Lieberman) | Katzung's Basic & Clinical Pharmacology
Explain hydroureteronephrosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hydronephrosis" AND "obstructive uropathy"
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the content and images needed for a thorough, illustrated explanation. Let me compile the answer.
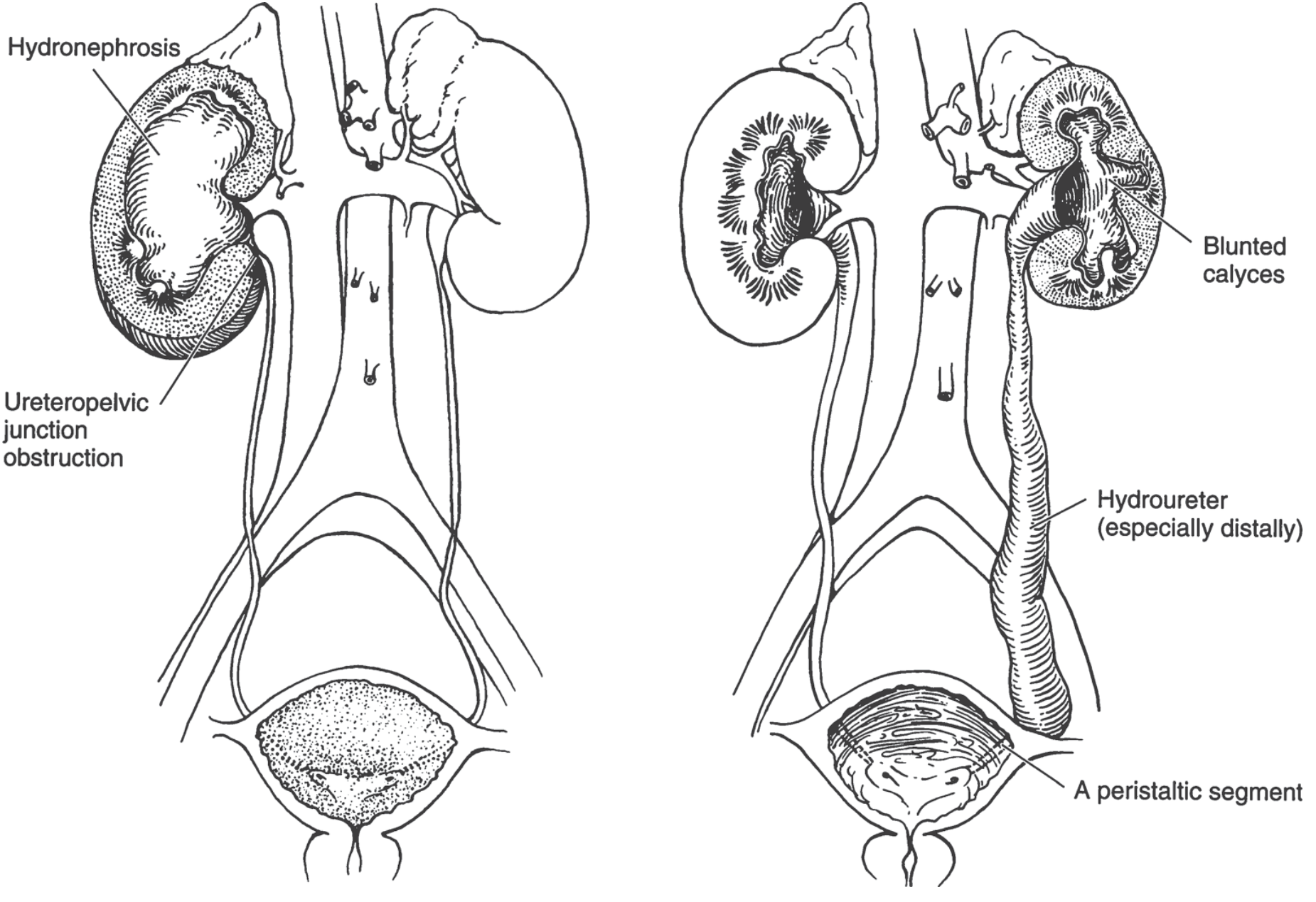
Hydroureteronephrosis
Hydroureteronephrosis is the simultaneous dilation of the renal collecting system (renal pelvis and calyces - "hydronephrosis") and the ureter ("hydroureter") due to obstruction to the outflow of urine anywhere from the kidney down to the bladder outlet. When only the kidney collecting system is distended without ureteral involvement, it is called hydronephrosis alone - as a rule, the combination implies an obstruction at or below the ureterovesical junction (UVJ), while isolated hydronephrosis implies an obstruction above, at the ureteropelvic junction (UPJ).
1. Anatomy of Obstruction - Where It Occurs
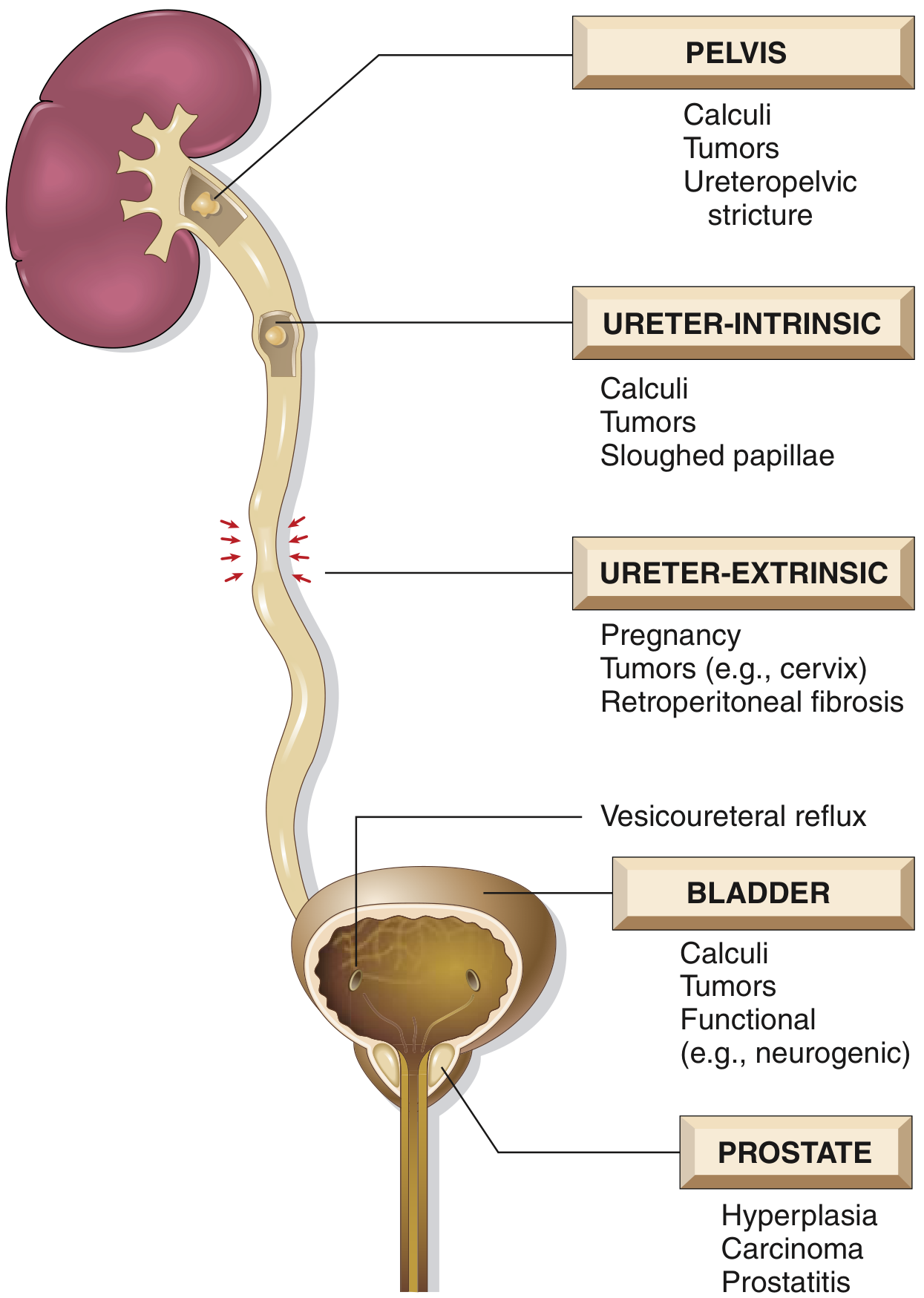
Key principle: Bilateral hydroureteronephrosis occurs only when the obstruction is below the level of the ureters (bladder or urethra). If blockage is at or above the ureters, the lesion is unilateral. - Robbins & Kumar Basic Pathology
2. Causes
Congenital (Intrinsic)
- UPJ obstruction - most common congenital ureteral abnormality; more common in boys (5:2 ratio) and on the left side; caused by abnormal smooth muscle investment, ureteral kinking, or aberrant lower pole renal artery compression
- UVJ obstruction (megaureter) - aperistaltic or narrowed segment at the ureterovesical junction
- Ureterocele - cystic dilation of the distal ureter within the bladder, often associated with ureteral duplication; nearly always causes significant hydroureteronephrosis
- Posterior urethral valves - male infants; obstructs below the bladder, causes bilateral hydroureteronephrosis
- Smith & Tanagho's General Urology; Campbell-Walsh-Wein Urology
Acquired - Intrinsic
| Site | Cause |
|---|---|
| Renal pelvis / UPJ | Calculi, transitional cell carcinoma, stricture |
| Ureter | Calculi (most common cause of acute unilateral obstruction), urothelial tumors, sloughed papillae |
| Bladder | Bladder calculi, bladder carcinoma, neurogenic bladder |
| Urethra/prostate | BPH (most common cause of bilateral obstruction in older men), prostate carcinoma, urethral stricture |
Acquired - Extrinsic Compression
- Malignancy - approximately 70% of tumors causing ureteral obstruction are genitourinary (cervical cancer most common, then bladder and prostate); breast, GI carcinoma, and lymphoma make up most of the rest - Comprehensive Clinical Nephrology 7e
- Retroperitoneal fibrosis - mediates bilateral ureteral encasement
- Pregnancy - two mechanisms: (1) mechanical compression of the ureters at the pelvic brim by the gravid uterus (right side > left due to dextrorotation), and (2) progesterone-mediated smooth muscle relaxation; begins at ~20 weeks gestation - NKF Primer on Kidney Diseases
- Lymphocele / pelvic hematoma - post-surgery or transplant
- Enlarged pelvic lymph nodes
3. Pathophysiology
Once obstruction occurs, the following sequence unfolds: - Robbins & Kumar Basic Pathology; Campbell-Walsh-Wein
- Continued glomerular filtration despite the obstruction causes progressive dilation of the renal pelvis, calyces, and ureter proximal to the blockage
- Rising intrapelvic pressure is transmitted back through the collecting ducts, compressing the renal vasculature - this causes arterial insufficiency and venous stasis
- Tubular dysfunction first - the papillae, most vulnerable to pressure, are damaged earliest; the primary functional loss is tubular concentrating ability (tubular function is impaired before GFR falls)
- Interstitial inflammation and fibrosis follows, mediated by:
- TGF-β1 - key profibrotic cytokine
- Angiotensin II (upregulated rapidly post-obstruction) - causes vasoconstriction, stimulates TGF-β1 and TNF-α, drives interstitial fibrosis; ACE inhibitors/ARBs can partially attenuate this
- IL-18 - triggers tubular epithelial-to-mesenchymal transition (EMT) and fibroblast proliferation
- Thromboxane A2 (TXA2) and prostaglandins - alter renal hemodynamics
- GFR falls later as pressure-mediated ischemia propagates and fibrosis replaces functional nephrons
- Sudden complete obstruction causes early GFR compromise before significant dilation develops; with partial/intermittent obstruction, massive dilation can develop with relatively preserved function initially
- Campbell-Walsh-Wein Urology; Brenner & Rector's The Kidney
4. Morphology (Gross and Microscopic)
Gross pathology:
- With subtotal or intermittent obstruction, the kidney may reach lengths of 20 cm
- The organ becomes largely a thin-walled, fluid-filled sac - the greatly distended pelvicalyceal system
- Renal parenchyma is compressed and atrophied; papillae are obliterated; pyramids are flattened
- The ureter proximal to the obstruction is dilated and tortuous (hydroureter)

Microscopic pathology:
- Early: tubular dilation and atrophy
- Late: loss of glomeruli, replacement of renal parenchyma by fibrous tissue
- Superimposed pyelonephritis is common
- Robbins & Kumar Basic Pathology, p. 528
5. Clinical Features
| Situation | Presentation |
|---|---|
| Unilateral hydroureteronephrosis | Often asymptomatic for long periods; may present as flank pain, hematuria, or palpable mass; discovered incidentally on imaging |
| Acute ureteral stone | Severe colicky flank pain radiating to groin, nausea, vomiting |
| Malignant ureteral obstruction | Rarely presents with colic; more often insidious decline in GFR, presenting to nephrologist |
| Bilateral obstruction | Anuria + renal failure (obstructive uropathy) |
| Incomplete bilateral obstruction | Paradoxically, polyuria (not oliguria) due to loss of tubular concentrating ability |
| Bladder outlet obstruction | Bladder distension, overflow incontinence, weak stream |
- Robbins; Comprehensive Clinical Nephrology 7e
6. Diagnosis
- Ultrasound - first-line imaging; sensitive for identifying hydronephrosis (dilated renal pelvis and calyces) and hydroureter; used in antenatal screening and emergency settings. Mild dilation may be physiological (e.g., early pregnancy)
- CT urography (non-contrast) - gold standard for ureteric calculi; identifies level and cause of obstruction
- MRI urography - useful in pregnancy (avoids radiation)
- Diuretic renography (MAG3 scan) - quantifies differential renal function and drainage kinetics; distinguishes obstructed from non-obstructed dilation
- Antegrade pyelography (percutaneous) - best for defining the exact level of obstruction, especially when retrograde approach fails; can be combined with percutaneous nephrostomy (PCN)
- Retrograde ureteropyelography - endoscopic; detailed assessment of the ureteral lumen
7. Management
General principle: relieve obstruction promptly to preserve renal function. Recovery depends on the duration and degree of obstruction.
Acute/Urgent Relief
- Bladder outlet obstruction - urethral or suprapubic catheter
- Upper tract obstruction - retrograde double-J (DJ) ureteral stent placement is preferred; percutaneous nephrostomy (PCN) is the fallback if retrograde approach fails or if the patient is septic (PCN avoids endoscopic manipulation that could worsen bacteremia)
- In bilateral obstruction, draining the kidney with better-preserved parenchyma on CT/ultrasound is sufficient initially
- DJ stents and PCN tubes need replacement every 3-6 months; complications include migration, obstruction, infection, and lower urinary tract symptoms (urgency, frequency in ~70% of patients with stents)
- Comprehensive Clinical Nephrology 7e
Definitive Treatment (by cause)
| Cause | Treatment |
|---|---|
| Ureteric calculus | Ureteroscopy + laser lithotripsy; shockwave lithotripsy |
| BPH | Alpha-blockers; TURP; laser prostatectomy |
| UPJ obstruction (congenital) | Pyeloplasty (Anderson-Hynes); laparoscopic preferred |
| Malignant external compression | Stenting (metallic self-expanding stent for malignant obstruction); tumor-directed therapy |
| Retroperitoneal fibrosis | Steroids; ureterolysis |
| Ureterocele | Transurethral incision; heminephrectomy + ureteral reimplantation if needed |
| Neurogenic bladder | Intermittent catheterization; anticholinergics; botulinum toxin |
Post-Obstructive Diuresis
After relief of prolonged bilateral obstruction, a post-obstructive diuresis occurs - a large volume of urine is produced due to:
- Retained solutes (osmotic diuresis)
- Downregulation of tubular transporters (NKCC2 reduction, decreased aquaporin-2 phosphorylation)
- Early phase is partly prostaglandin (COX-2) mediated; late phase is tubular transporter-dependent
- Patients require careful fluid and electrolyte monitoring to avoid dehydration and electrolyte imbalance
- Brenner & Rector's The Kidney; Campbell-Walsh-Wein
8. Special Situations
- Physiological hydroureteronephrosis of pregnancy: right side predominates; mild and normally resolves postpartum; pathological obstruction (e.g., stone) should be excluded if pain or fever is present
- Post-renal transplant obstruction: most common in the early post-operative period; causes include poor ureteral implantation, blood clots, ischemic stricture, lymphocele compression, or BPH in the recipient. Ultrasound shows hydronephrosis; managed with DJ stenting or PCN
- Antenatally detected hydronephrosis: most common indication for fetal urinary tract investigation; many cases resolve spontaneously; those that persist require postnatal workup with ultrasound and voiding cystourethrogram (VCUG) to exclude vesicoureteral reflux
Sources: Robbins & Kumar Basic Pathology | Smith & Tanagho's General Urology 19e | Campbell-Walsh-Wein Urology | Brenner & Rector's The Kidney | Comprehensive Clinical Nephrology 7e | NKF Primer on Kidney Diseases 8e
This is a shared conversation. Sign in to Orris to start your own chat.