What is dementia
Reading File
Finding Sources
Searching PubMed
"dementia" AND "review"
Reading File
Reading File
Finding Sources
Searching the Web
dementia overview definition types causes symptoms 2024
Finding Sources
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive textbook content. Let me compile the full answer.
Dementia
Definition
Dementia is a decline in memory or other cognitive abilities from a previously higher level of function, leading to impaired activities of daily living. It is not a single disease but a clinical syndrome - a collection of symptoms caused by underlying brain diseases. Although "dementia" can technically describe any cognitive decline (including from a single head injury), the term is most often used for gradually progressive deterioration over months to years. - Neuroanatomy through Clinical Cases 3rd Edition, p. 960
It must be distinguished from:
- Normal aging: mild slowing that does not interfere with daily function
- Mild Cognitive Impairment (MCI): cognitive deterioration beyond age-matched norms, but not yet affecting daily activities; MCI is a prodromal phase for some individuals who later develop dementia
- Delirium: acute onset, fluctuating attention - not dementia
- Pseudodementia: depression or psychiatric disorders mimicking dementia
Types of Dementia
Primary (Neurodegenerative) - no cure, progressive
| Type | Key Features |
|---|---|
| Alzheimer's disease | Most common (>50% of cases over age 65). Gradual onset, early episodic memory loss, amyloid plaques, neurofibrillary tangles |
| Vascular dementia | 2nd most common. Stepwise decline, early executive dysfunction, linked to strokes/vascular risk factors |
| Dementia with Lewy bodies | Early parkinsonism + visual hallucinations, fluctuating cognition |
| Frontotemporal dementia (FTD) | Behavioral and/or language disturbance; often younger onset |
| Parkinson's disease dementia | Motor symptoms precede cognitive decline |
| Huntington's disease | Subcortical dementia; movement disorder |
| Progressive supranuclear palsy | Subcortical dementia; gait/eye movement issues |
Secondary (Potentially Reversible) - up to ~10% of cases
- Chronic hypothyroidism
- Vitamin B12 or folate deficiency
- Normal pressure hydrocephalus (NPH)
- Chronic subdural hematoma
- Neurosyphilis
- Medications with CNS side effects
- Heavy metal toxicity
- Wernicke-Korsakoff syndrome (thiamine deficiency)
Mixed Dementia
Alzheimer's disease combined with vascular pathology is common, particularly in older adults.
Symptoms
Cognitive domains affected:
- Memory - both short-term and long-term, especially episodic (day-to-day events)
- Language - word-finding difficulty, aphasia
- Executive function - planning, judgment, abstract thinking
- Visuospatial ability - getting lost, difficulty with familiar tasks
- Attention and concentration
Behavioural and psychological symptoms:
- Personality changes, apathy, agitation
- Depression and anxiety
- Psychosis (hallucinations, delusions) - especially in Lewy body dementia
- Sleep disturbances
- Wandering
Functional decline: Impairment in interpersonal relationships, work, and social activities is a diagnostic requirement - ROSEN's Emergency Medicine
Causes and Pathophysiology
Most dementias arise from neurodegeneration - the progressive death of neurons:
- Alzheimer's disease: accumulation of beta-amyloid plaques (extracellular protein deposits) and neurofibrillary tangles (intracellular hyperphosphorylated tau protein). Changes begin in the medial temporal lobes (hippocampus, entorhinal cortex) - explaining why memory is affected first - then spread to association cortex. There is also loss of cholinergic neurons from the nucleus basalis.
- Vascular dementia: repeated strokes or chronic small vessel disease cutting off blood supply to brain regions.
- Lewy body dementia: abnormal accumulation of alpha-synuclein protein.
- Frontotemporal dementia: TDP-43 or tau protein accumulations in frontal/temporal lobes.
Diagnosis
A diagnosis combines:
- Clinical history - including functional assessment and collateral history from family
- Cognitive testing - Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Clinical Dementia Rating (CDR), Activities of Daily Living (ADL) scales
- Blood tests - thyroid function, B12/folate, syphilis serology, metabolic panel (to rule out reversible causes)
- Brain imaging - CT or MRI (to detect atrophy, vascular lesions, or structural causes); PET scanning for amyloid or metabolism
- Neuropsychological testing - to distinguish true dementia from pseudodementia due to depression
- Goldman-Cecil Medicine, p. 3803
Management
No cure exists for most primary dementias, but treatment focuses on:
-
Pharmacological (symptomatic):
- Cholinesterase inhibitors (donepezil, rivastigmine, galantamine) - for Alzheimer's and Lewy body dementia
- Memantine (NMDA receptor antagonist) - for moderate-to-severe Alzheimer's
- Medications for BPSD (behavioural/psychological symptoms)
- Newer disease-modifying agents (anti-amyloid antibodies, e.g., lecanemab) are emerging for early Alzheimer's
-
Non-pharmacological:
- Cognitive stimulation and rehabilitation (shown effective in recent meta-analysis, PMID 39485657)
- Physical exercise, structured routine, caregiver education
- Safety modifications at home
-
Palliative care (advanced stages):
- Goals-of-care conversations early, while the patient has capacity
- Comfort feeding (PEG tubes NOT recommended in advanced dementia - they do not reduce aspiration or improve survival)
- Hospice care improves symptom management and family satisfaction
- Bradley and Daroff's Neurology in Clinical Practice
Epidemiology
- Aging is the single greatest risk factor
- Over 50% of dementia in people aged 65+ is due to Alzheimer's disease
- Dementia can also occur in younger people (<65 years = "young-onset dementia")
- Estimated tens of millions affected globally; prevalence rises sharply with age
Key Takeaways
| Feature | Detail |
|---|---|
| Not one disease | A syndrome with many underlying causes |
| Most common cause | Alzheimer's disease |
| Reversible causes | ~10% - always screen for them |
| Hallmark of diagnosis | Cognitive decline + functional impairment |
| First area affected in Alzheimer's | Hippocampus - explaining early memory loss |
| Main drug classes | Cholinesterase inhibitors, memantine |
What is dementia
Finding Sources
Searching the Web
dementia definition types causes symptoms treatment 2025
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive textbook content and supporting images. Here is the full answer:
Dementia
Definition
Dementia is a decline in memory or other cognitive abilities from a previously higher level of function, leading to impaired activities of daily living. It is not a single disease - it is a clinical syndrome (an umbrella term) for a collection of symptoms caused by various underlying brain diseases. The term is most often applied when deterioration is gradually progressive over months to years, though it technically covers any lasting cognitive decline.
- Neuroanatomy through Clinical Cases 3rd Edition, p. 960
- Goldman-Cecil Medicine, Chapter 371
Key distinctions to make:
| Condition | How it differs from dementia |
|---|---|
| Normal aging | Mild slowing that does NOT interfere with daily activities |
| Mild Cognitive Impairment (MCI) | Decline beyond age norms but NO functional impairment; may or may not progress |
| Delirium | Acute onset, fluctuating attention - not chronic |
| Pseudodementia | Depression or psychiatric illness mimicking dementia - potentially reversible |
Types and Causes
Dementia is divided into primary (neurodegenerative, usually irreversible) and secondary (caused by other conditions, sometimes reversible):
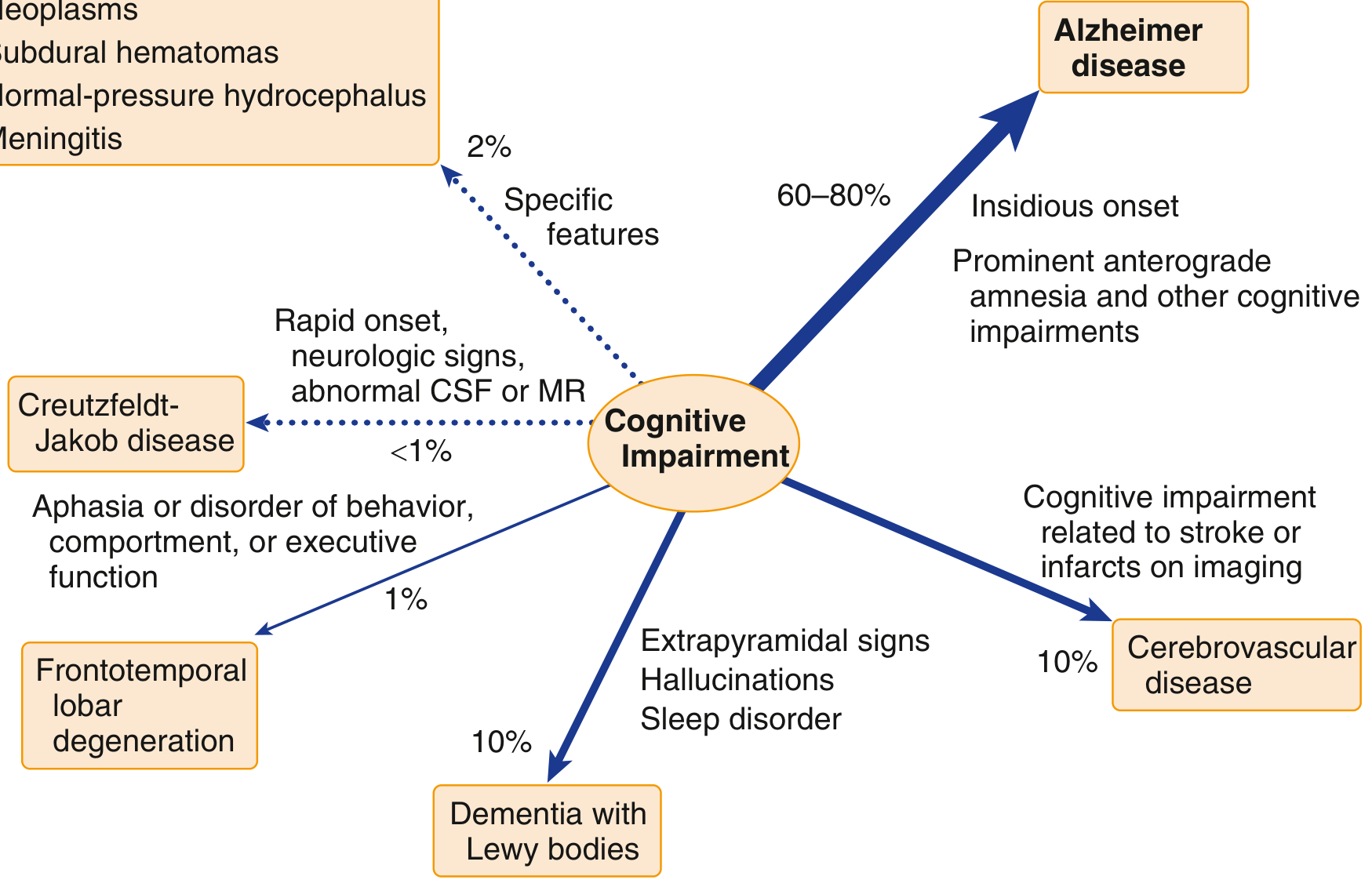
Differential diagnosis of cognitive impairment, showing approximate proportions:
Primary (Neurodegenerative) Dementias
| Type | Key Features |
|---|---|
| Alzheimer's disease | Most common (60-80% of cases). Insidious onset; early anterograde amnesia (episodic memory); amyloid plaques + neurofibrillary tangles |
| Vascular dementia | ~10%. Stepwise decline; early executive dysfunction; linked to strokes or small vessel disease |
| Dementia with Lewy bodies | ~10%. Extrapyramidal signs, visual hallucinations, sleep disorder, fluctuating cognition |
| Frontotemporal dementia (FTD) | ~1%. Aphasia or prominent behavioural/personality change; younger onset |
| Parkinson's disease dementia | Motor symptoms precede cognitive decline |
| Huntington's disease | Subcortical dementia; movement disorder |
Secondary (Potentially Reversible) Causes - found in ~10% of evaluations
- Normal-pressure hydrocephalus (NPH)
- Hypothyroidism / hyperthyroidism
- Vitamin B12 or folate deficiency
- Thiamine deficiency (Wernicke-Korsakoff syndrome)
- Chronic subdural hematoma
- Neurosyphilis, HIV, CNS infections
- Heavy metal toxicity
- Autoimmune encephalitis
- Medications with CNS side effects
Symptoms
Core cognitive domains affected:
- Memory - both short-term and long-term; episodic memory is hit first in Alzheimer's
- Language - word-finding difficulty, aphasia
- Executive function - planning, judgment, abstract thinking
- Visuospatial ability - getting lost, difficulty with familiar tasks
- Attention and concentration
Behavioural and psychological symptoms (BPSD):
- Apathy, personality changes, agitation
- Depression and anxiety
- Psychosis (hallucinations, delusions) - especially in Lewy body dementia
- Sleep disturbances
- Wandering
Functional impairment (interference with interpersonal relationships, work, and social activities) is a diagnostic requirement.
Pathophysiology (Alzheimer's Disease - the main example)
In Alzheimer's disease, pathological changes start in the medial temporal lobes (hippocampus and entorhinal cortex) - which explains why memory is the first symptom - then spread to association cortices of the frontal, parietal, and temporal lobes.
Two hallmark lesions:
- Amyloid (neuritic) plaques - extracellular deposits of beta-amyloid protein, derived from abnormal cleavage of amyloid precursor protein (APP). Beta-amyloid begins accumulating up to 20 years before symptoms appear.
- Neurofibrillary tangles - intracellular accumulations of hyperphosphorylated tau protein. The spread of tangles closely mirrors the clinical progression of disease.
There is also significant loss of cholinergic neurons arising from the nucleus basalis, septum, and diagonal band - this forms the basis for drug treatment.
MRI in Alzheimer's disease - normal brain (left) vs. 11 years later with dementia (right), showing dramatic hippocampal atrophy:
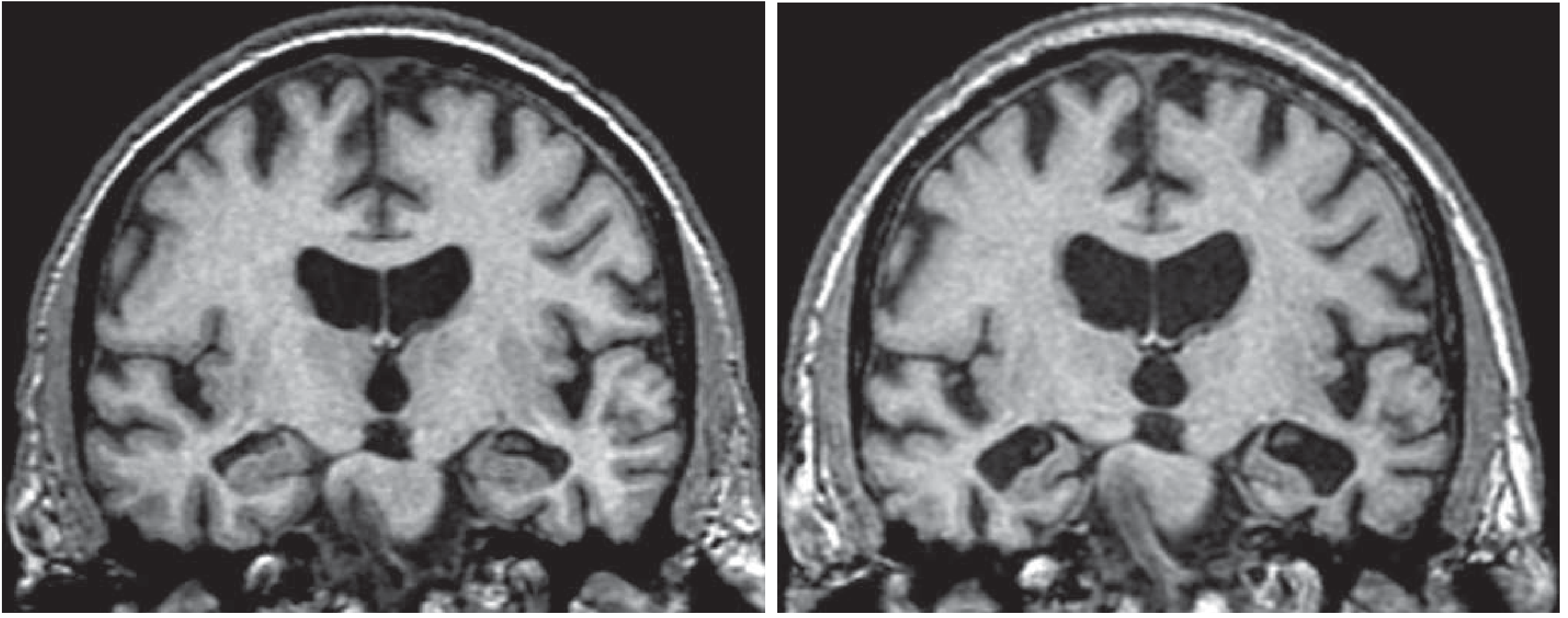
Goldman-Cecil Medicine, Fig. 371-3
Diagnosis
- Clinical history - detailed collateral history from family; assess activities of daily living, medication review, family history
- Cognitive testing - Mini-Mental State Exam (MMSE), Montreal Cognitive Assessment (MoCA), Clinical Dementia Rating (CDR), Activities of Daily Living (ADL) scale
- Blood tests - thyroid function, B12/folate, metabolic panel, syphilis serology (to exclude reversible causes)
- Brain MRI - detect atrophy, vascular lesions, structural causes; hippocampal atrophy is characteristic of Alzheimer's
- Advanced imaging (selected cases) - FDG-PET (regional hypometabolism), amyloid-PET, CSF biomarkers (Aβ42, phospho-tau)
- Lumbar puncture - if rapid progression, young onset, or atypical features
Management
Pharmacological
| Drug class | Drugs | Indication |
|---|---|---|
| Cholinesterase inhibitors | Donepezil, rivastigmine, galantamine | Mild-to-moderate Alzheimer's; also Lewy body dementia |
| NMDA antagonist | Memantine | Moderate-to-severe Alzheimer's |
| Disease-modifying (emerging) | Lecanemab, donanemab (anti-amyloid antibodies) | Early Alzheimer's - approved recently for slowing progression |
Cholinesterase inhibitors and memantine produce modest improvements in caregiver ratings of functioning; cognitive improvement is seen mainly with cholinesterase inhibitors. - Harrison's Principles of Internal Medicine 22e
Non-pharmacological
- Cognitive stimulation, cognitive training, and cognitive rehabilitation
- Physical exercise and structured daily routines
- Caregiver education and support
- Environmental safety modifications (preventing falls, wandering)
Palliative / Advanced Stages
- Goals-of-care conversations early, while the patient retains capacity
- Advance care planning for feeding, hospitalisation, and end-of-life wishes
- PEG tubes are NOT recommended in advanced dementia - no proven benefit for aspiration, wound healing, or survival; hand/comfort feeding is preferred
- Hospice care improves symptom management and family satisfaction
Epidemiology & Risk Factors
- Aging is the single greatest risk factor - prevalence of Alzheimer's doubles every 5 years after age 65
- Estimated 6.7 million older adults have Alzheimer's in the US; projected ~14 million by 2060 (CDC)
- Young-onset dementia = onset before age 65
- Other risk factors: family history, low educational attainment (less cognitive reserve), midlife vascular risk factors (hypertension, diabetes, high LDL), head injury
Summary
| Feature | Key Point |
|---|---|
| What it is | A syndrome, not a single disease |
| Most common cause | Alzheimer's disease (60-80%) |
| Reversible causes | ~10% - always screen for them |
| Diagnostic requirement | Cognitive decline + functional impairment |
| First brain region in Alzheimer's | Hippocampus - explains early memory loss |
| Pathological hallmarks | Amyloid plaques + neurofibrillary tangles (tau) |
| Drug treatment | Cholinesterase inhibitors + memantine (symptomatic only) |
For a visual overview of the major types, stages, and treatments:
This is a shared conversation. Sign in to Orris to start your own chat.