What is the protocol of Fluid resuscitation in patient of acute pancreatitis 24 hr 48 hr 72 hr and thereafter
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute pancreatitis" AND "fluid resuscitation"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive, multi-source data. Let me compile the full answer.
Fluid Resuscitation Protocol in Acute Pancreatitis
Fluid resuscitation is the single most important initial treatment in acute pancreatitis. The goal is to replace massive third-space losses from the systemic inflammatory response, prevent pancreatic microvascular ischemia, and avoid end-organ damage - while not over-resuscitating, which carries its own serious risks.
Preferred Fluid
Lactated Ringer's (LR) solution is strongly preferred over normal saline (0.9% NaCl):
- LR has demonstrated lower C-reactive protein levels (anti-inflammatory effect)
- Large volumes of NS cause hyperchloremic metabolic acidosis, which activates trypsinogen, making acinar cells more prone to injury and worsening SIRS
- LR may provide direct anti-inflammatory benefits through its lactate buffering
- Colloids are not recommended over crystalloids; colloid use is only considered if hematocrit falls below 24% or albumin drops below 2 g/dL
(Rosen's Emergency Medicine; Current Surgical Therapy 14e, p.582)
The Time-Based Protocol
Resuscitation Targets (All Time Points)
Before diving into time phases, understand the end-points that guide fluid titration:
| Parameter | Target |
|---|---|
| Heart rate | < 120 beats/min |
| Mean arterial pressure (MAP) | 65-85 mmHg |
| Urine output | > 0.5-1 mL/kg/hour |
| Hematocrit | Falling (not rising) - target ~35-44% |
| BUN | Falling or stable |
| CVP (severe cases / ICU) | 8-12 mmHg |
| Mixed venous O₂ saturation (ICU) | ≥ 70% |
First 24 Hours - Aggressive Resuscitation Phase
This is the most critical window. Inadequate resuscitation in the first 24 hours is directly linked to increased:
- Pancreatic necrosis (from hypoperfusion)
- SIRS and organ failure
- ICU admission rates
- Need for invasive interventions
What to do:
- Initial bolus: 1-2 L of LR over 30-60 minutes (15-20 mL/kg bolus = approximately 1050-1400 mL in a 70 kg patient)
- Maintenance rate: 250-500 mL/hour (ACG recommendation) OR 5-10 mL/kg/hour (IAP/APA goal-directed recommendation)
- Total first-24-hour volume: typically 2500-4000 mL is required in most patients
- Patients with severe volume depletion, significant tachycardia, or hypotension may need more rapid infusion
- Monitoring: Hematocrit and BUN every 8-12 hours; vitals continuous or every 2-4 hours; strict urine output measurement (Foley catheter mandatory)
- A fall in hematocrit and BUN within the first 12-24 hours is strong evidence of adequate resuscitation
Note: Overly aggressive fluid therapy (historically up to 20 mL/kg/hour) has been shown to increase risk of fluid overload, acute lung injury, and abdominal compartment syndrome. A recent RCT showed that the traditional aggressive strategy increased fluid overload risk compared to a moderate-intensity strategy (10 mL/kg bolus then 1.5 mL/kg/hour) without improving outcomes.
(Harrison's Principles 22E, 2025; Current Surgical Therapy 14e)
24-48 Hours - Reassessment and Goal-Directed Phase
By this period, the degree of disease severity is becoming clearer (CRP peaks at 24-48 hours and is a reliable severity marker at this stage):
- Continue LR at a rate titrated to resuscitation targets
- Reduce rate if resuscitation goals are being met (HR < 120, MAP adequate, urine output > 0.5-1 mL/kg/hr) to avoid fluid overload
- Reassess every 6-8 hours with bedside clinical evaluation (vitals, O₂ saturation, physical exam)
- Monitor for volume overload signs: tachypnea, hypoxia, lower extremity edema, pleural effusion on CXR
- Rising BUN at this stage signals ongoing inadequate hydration AND is independently associated with higher in-hospital mortality
- Patients with persistent tachycardia, hypotension, or oliguria require escalation to ICU with invasive hemodynamic monitoring
- For severe acute pancreatitis: target CVP 8-12 mmHg, mixed venous O₂ saturation ≥ 70%
- Consider CT scan after 48-72 hours if not improving to assess for pancreatic necrosis
(Rosen's EM; Harrison's Principles 22E, 2025)
48-72 Hours - Transition Phase
- If patient is stabilizing (vitals normalized, urine output adequate, falling BUN/hematocrit), begin tapering IV fluid rate
- Introduce early enteral nutrition - do not wait for lipase normalization; current guidelines recommend oral feeding within 24-48 hours in mild-moderate cases when tolerated
- Continue monitoring for signs of fluid overload; diuresis may be appropriate once the initial hypovolemia has resolved
- If not improving: CT with IV contrast should be performed to assess for necrosis
- Persistent organ failure beyond 48 hours defines severe acute pancreatitis and warrants continued aggressive ICU-level management
Beyond 72 Hours - Maintenance and Weaning Phase
- Transition from IV fluids to enteral/oral intake as tolerated
- Mild-to-moderate disease: most patients should be tolerating oral liquids or a low-fat solid diet by this point
- Severe/necrotizing pancreatitis: continue hemodynamic monitoring; nasojejunal tube feeding is preferred over parenteral nutrition
- Parenteral nutrition (TPN) is reserved for patients who cannot tolerate oral or nasojejunal feeds within 5-7 days of admission
- Avoid prophylactic antibiotics unless infected necrosis is documented (positive FNA culture or clinical/radiographic deterioration)
- If fever, rising WBC, or hemodynamic deterioration occurs: consider infected pancreatic necrosis - obtain FNA culture, start carbapenems (better pancreatic penetration than cephalosporins or fluoroquinolones)
(Current Surgical Therapy 14e; Maingot's Abdominal Operations)
Summary Table
| Time Window | Fluid Rate | Key Actions | Monitoring |
|---|---|---|---|
| 0-24 h | Bolus 1-2 L, then 250-500 mL/h (or 5-10 mL/kg/h) | Aggressive resuscitation, NPO, analgesics | HCT + BUN every 8-12 h; strict I/O; Foley |
| 24-48 h | Titrate down to resuscitation targets | Reassess severity (CRP peaks); ICU if needed | Clinical eval every 6-8 h; CVP in severe cases |
| 48-72 h | Taper if stable; wean if tolerating PO | Start enteral feeding; CT scan if not improving | Watch for fluid overload; check for necrosis |
| > 72 h | IV fluids as needed; transition to oral/EN | TPN only if EN fails; treat complications | Ongoing hemodynamic and organ function monitoring |
Management Algorithm (Maingot's)
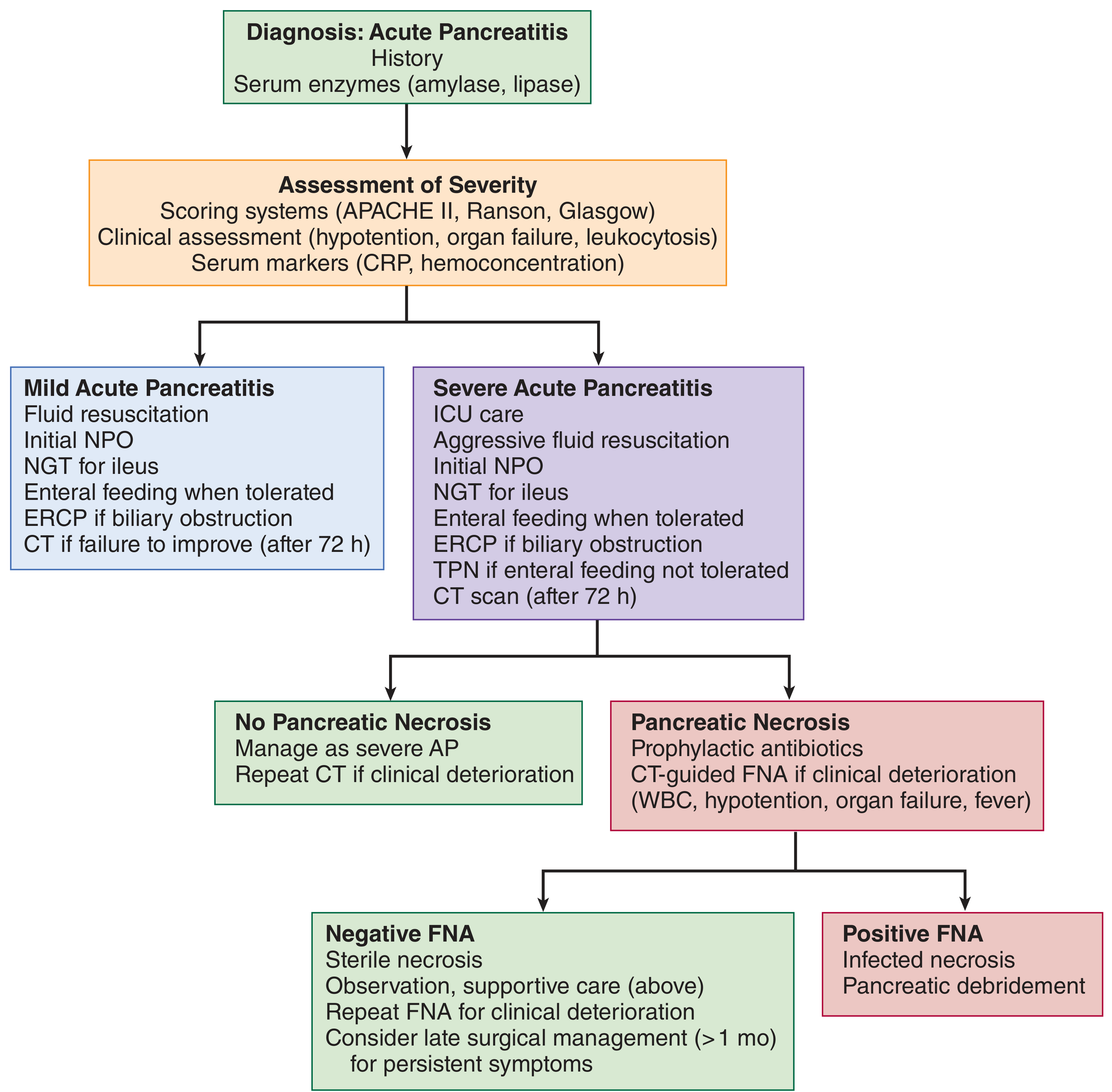
Fig 54-6 from Maingot's Abdominal Operations - Management algorithm for acute pancreatitis
Recent Evidence Update (2023-2025)
Recent meta-analyses support several key points:
- LR vs. NS: Multiple 2024-2025 meta-analyses confirm LR reduces progression to moderate-to-severe acute pancreatitis compared to NS (PMID: 40085761)
- A 2023 systematic review confirmed that early, goal-directed resuscitation within the first 24-48 hours improves outcomes, but that the optimal volume strategy remains an area of active research (PMID: 37689561)
- The WATERFALL RCT (referenced in Harrison's 22E, 2025) showed that moderate-intensity hydration (10 mL/kg bolus + 1.5 mL/kg/hr) was non-inferior to aggressive hydration but with significantly less fluid overload - this has shifted recent guidelines toward goal-directed rather than blanket aggressive protocols
Key clinical takeaway: Fluid resuscitation in acute pancreatitis is not a "set rate and forget" protocol. It requires reassessment every 6-8 hours using clinical parameters, BUN, hematocrit, and urine output. The risk of under-resuscitation (necrosis, organ failure) and over-resuscitation (ARDS, abdominal compartment syndrome) are both real and must be balanced through goal-directed therapy.
This is a shared conversation. Sign in to Orris to start your own chat.