Classification and clinical features of cl and cp
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Cleft Lip (CL) and Cleft Palate (CP) - Classification and Clinical Features
Cleft lip and/or palate (CL/P) is the most common congenital orofacial abnormality, occurring in approximately 1:600 live births. They may occur in isolation or as part of over 300 recognized syndromes.
Incidence Distribution
| Type | Frequency |
|---|---|
| Cleft lip alone | ~15% |
| Cleft lip + palate | ~45% |
| Isolated cleft palate | ~40% |
- Cleft lip ± palate is more common in males
- Isolated cleft palate is more common in females
Classification
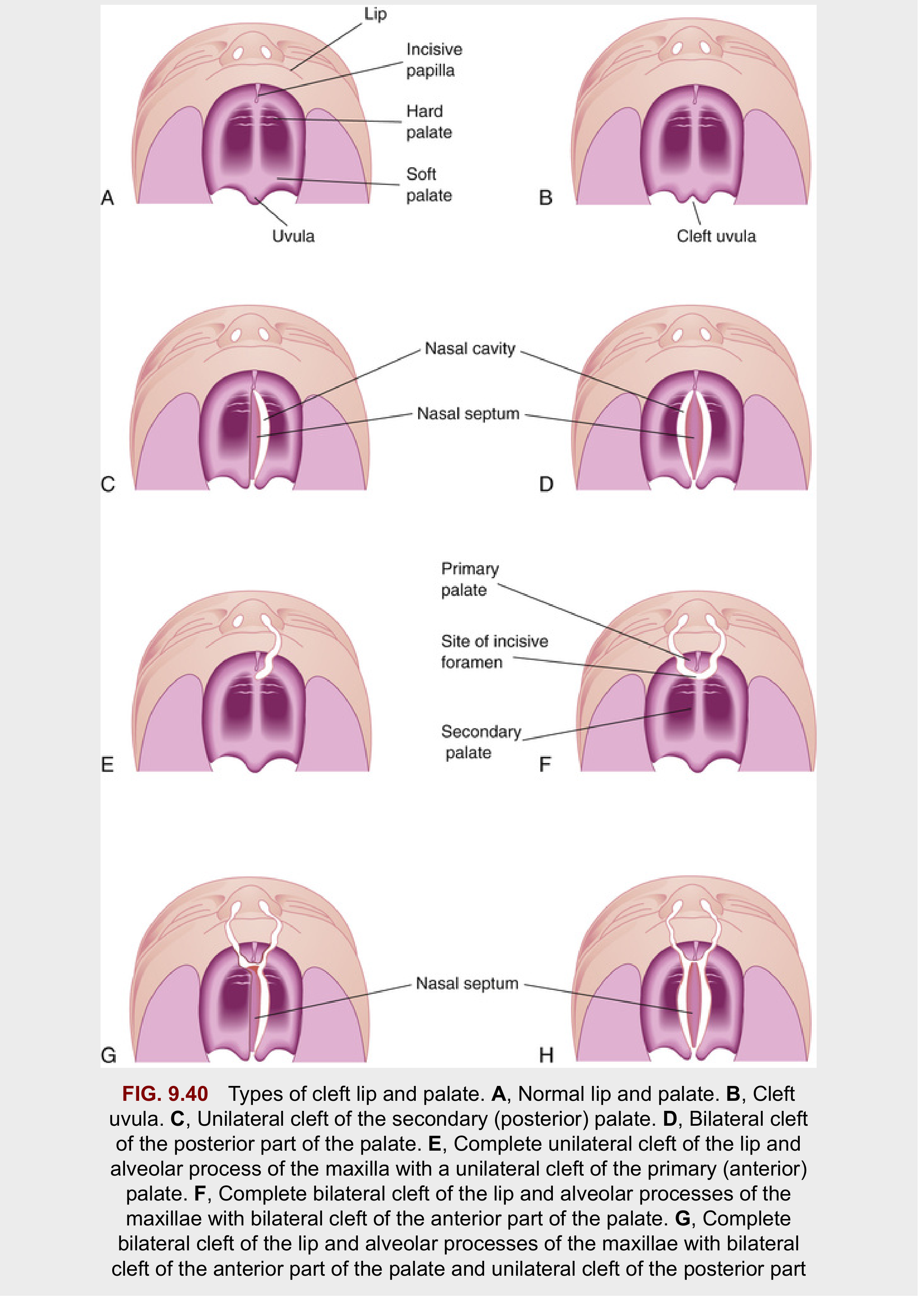
Anatomical Landmark - The Incisive Foramen
The incisive foramen is the key embryologic reference point dividing the palate into:
- Primary palate (anterior to incisive foramen): premaxilla, lip, nasal tip, and columella
- Secondary palate (posterior to incisive foramen): hard palate + soft palate, extending to the uvula
Two Major Phenotypic Groups
Group 1 - Cleft Lip with or without Cleft Palate (CL±P)
Involves structures anterior to the incisive foramen (primary palate), with or without extension posteriorly.
Group 2 - Isolated Cleft Palate (CP)
Involves the secondary palate only; embryologically and epidemiologically distinct from Group 1.
Classification of Cleft Lip
| Type | Description |
|---|---|
| Unilateral | One side only (specify left or right) |
| Bilateral | Both sides |
| Complete | Involves entire vertical height of upper lip, often with alveolar cleft |
| Incomplete | Involves only a portion of the lip height; a variable band of continuity remains across the cleft |
| Forme fruste / Microform | Minimal cleft - muscular diastasis with intact overlying skin only |
| Simonart band | A bridge of lip tissue (usually skin, sometimes with muscle) crossing an otherwise complete cleft gap |
(Source: Cummings Otolaryngology Head & Neck Surgery)
Classification of Cleft Palate
| Type | Description |
|---|---|
| Cleft uvula | Mildest form - bifid uvula only |
| Incomplete cleft palate | Soft palate ± part of hard palate; hard palate remains attached to nasal septum/vomer |
| Complete cleft palate | Full separation; nasal septum/vomer completely separated from palatine processes |
| Unilateral | Maxillary process on one side fused with nasal septum |
| Bilateral | No fusion of maxilla to nasal septum on either side |
| Submucous cleft palate (SMCP) | Least severe; intact mucosa but deficient/misdirected underlying musculature |
| Primary palate cleft | Anterior to incisive foramen (CL ± alveolus) |
| Secondary palate cleft | Posterior to incisive foramen (soft and/or hard palate) |
| Combined | Involves both primary and secondary palate |
(Source: Cummings Otolaryngology; Bailey & Love's Surgery)
Classification Diagram (The Developing Human - Moore)
Clinical Features
Cleft Lip
Unilateral Cleft Lip:
- Disruption of the nasolabial and bilabial muscle chains (orbicularis oris)
- The orbicularis muscle fibres, instead of running transversely, are misdirected and insert into the base of the columella on the cleft side and into the alar base
- Nasal deformity: the alar cartilage on the cleft side is displaced downward and outward; the columella is deviated away from the cleft
- The nasal tip is asymmetric, with a widened alar base on the cleft side

Bilateral Cleft Lip:
- Disruption is greater but often symmetrical
- Bilateral flaring of the nose (absence of nasolabial muscle continuity)
- Protrusive premaxilla - often projecting significantly forward
- Prolabium - a strip of skin in front of the premaxilla devoid of muscle
- Cartilaginous and skeletal deformities influence the overlying mucocutaneous tissues
Cleft Palate
Hard palate features:
- Failure of fusion of the two palatine shelves
- In complete cleft: the median part of the palatal vault is absent; palatal fibromucosa is reduced in size
- Communication between oral and nasal cavities
Soft palate features:
- In a normal palate, levator veli palatini fibres run transversely with no significant attachment to hard palate
- In a cleft palate, muscle fibres are oriented anteroposteriorly, inserting abnormally into the posterior edge of the hard palate
- This misdirected musculature critically impairs velopharyngeal closure
Submucous Cleft Palate (SMCP) - Classic Triad:
- Bifid uvula
- Zona pellucida - a bluish midline streak from deficient muscle under intact mucosa
- Notch in the posterior hard palate (palpable rather than visible)
(Note: Diagnosis of SMCP does not require all three features)
Functional Consequences
| Problem | Mechanism |
|---|---|
| Feeding difficulty | Inability to create negative intraoral pressure for suckling |
| Speech disorders | Velopharyngeal insufficiency; hypernasal speech |
| Recurrent otitis media / hearing loss | Eustachian tube dysfunction due to levator veli palatini abnormality |
| Dental abnormalities | Missing, supernumerary, or malformed teeth; malocclusion |
| Nasal deformity | Alar cartilage displacement, septal deviation |
| Psychosocial impact | Altered facial appearance and speech |
Associated Syndromes
Isolated cleft palate is more commonly syndromic than CL±P. Frequently associated syndromes include:
- Stickler syndrome (ophthalmic + musculoskeletal features)
- DiGeorge syndrome (cardiac + thymic anomalies; 22q11 deletion)
- Down syndrome (Trisomy 21)
- Apert syndrome (craniosynostosis + syndactyly)
- Treacher Collins syndrome (mandibulofacial dysostosis)
- Pierre Robin sequence (micrognathia + glossoptosis + CP)
Over 150 named syndromes are associated with cleft lip and palate. All children born with a cleft should be screened for other congenital abnormalities and offered genetic counselling where syndromic cause is suspected.
Sources: Bailey & Love's Short Practice of Surgery 28e, p. 762-765 | Cummings Otolaryngology Head & Neck Surgery, Ch. 188 | The Developing Human: Clinically Oriented Embryology, p. 537-541
This is a shared conversation. Sign in to Orris to start your own chat.