Compartment syndrome
Reading File
Finding Sources
Searching PubMed
"compartment syndrome" diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full, detailed response.
Compartment Syndrome
Definition
Compartment syndrome is raised pressure within a closed, non-expandable osseofascial compartment to a level that compromises tissue perfusion, leading to ischemia and irreversible damage to muscles and nerves. Normal compartment pressure is 0 mmHg; microcirculation is generally impaired at ≥30 mmHg.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Rosen's Emergency Medicine, 9th Ed.
Anatomy
The leg has four compartments: anterior, lateral, superficial posterior, and deep posterior. The forearm has three: superficial volar, deep volar, and dorsal.
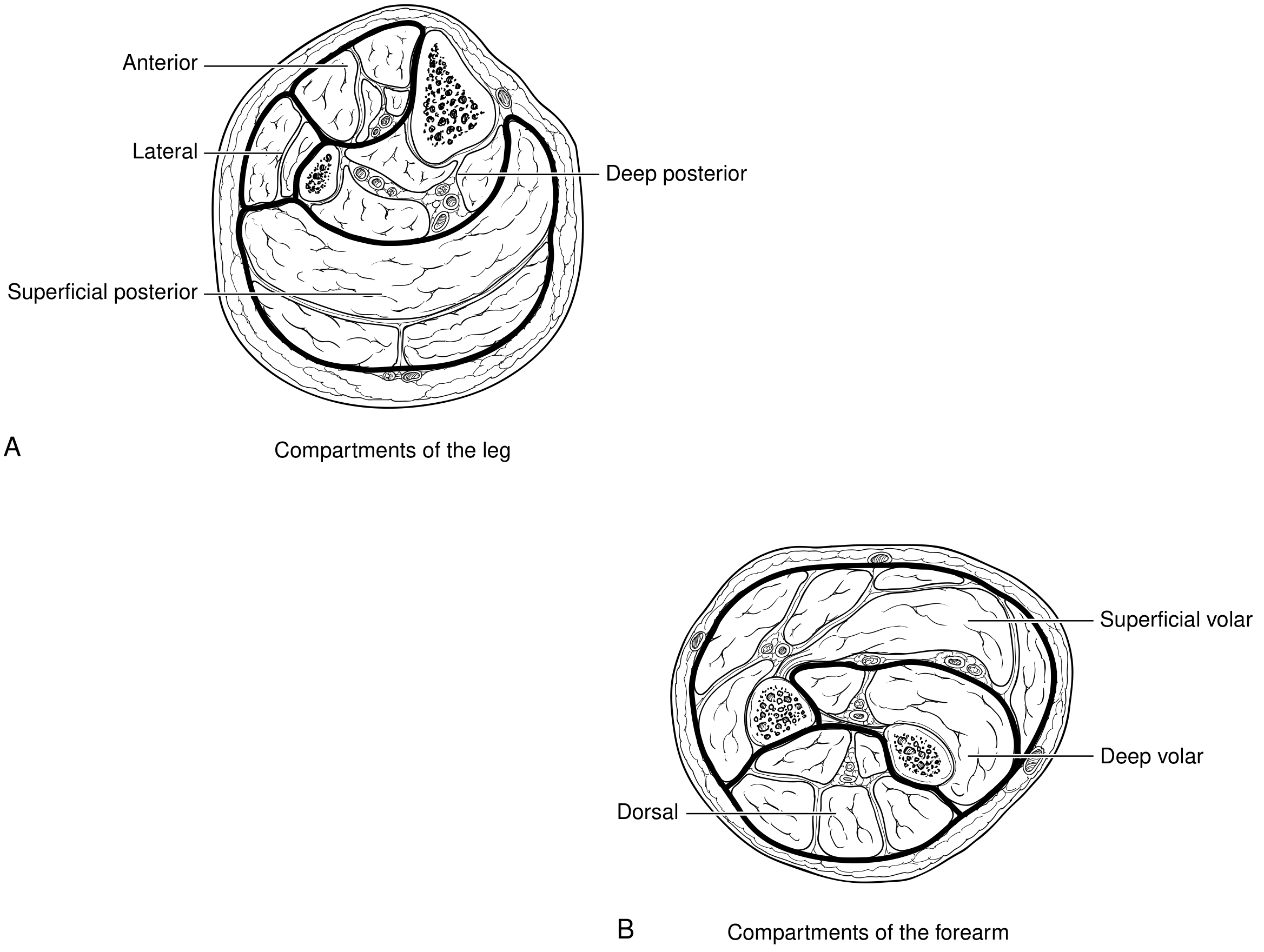
Current Surgical Therapy, 14th Ed. - The leg is most commonly involved, particularly the anterior compartment, due to its location and frequency of high-energy trauma.
Causes
Compartment syndrome arises from three mechanisms: increased compartment contents, decreased compartment volume, or external pressure.
Common causes - increased compartment content:
| Category | Examples |
|---|---|
| Fractures (most common, ~70%) | Tibial shaft fracture (most typical), long bone fractures |
| Soft tissue injury (~23%) | Crush injury, contusion |
| Bleeding | Vascular injury, coagulopathy, anticoagulation therapy |
| Reperfusion edema | Post-ischemic swelling after arterial repair/embolectomy |
| Burns | Circumferential third-degree burns (thermal, electrical) |
| Increased capillary filtration | Ergotamine ingestion, venous obstruction, nephrotic syndrome |
| Intensive muscle use | Exercise, seizures, eclampsia, tetany |
| Orthopedic procedures | ORIF, tibial osteotomy |
| Miscellaneous | IV extravasation, pressure transfusion, prolonged lithotomy/tuck positions |
Decreased compartment volume: closure of fascial defects, excessive traction on fractured limbs.
External pressure: tight casts, dressings, air splints, lying on limb.
- Rosen's Emergency Medicine (Box 41.3)
Pathophysiology
- Injury/edema raises tissue pressure within the closed fascial space
- Elevated tissue pressure increases venous pressure → reduces arteriovenous gradient → tissue hypoxia
- Histamine release attempts to dilate capillaries but also increases capillary permeability → protein/fluid leak → further pressure rise (vicious cycle)
- Venous blood flow impairment → arterial capillary flow falls below metabolic needs → ischemic necrosis of muscle and nerve
A key concept: perfusion becomes critically compromised when tissue pressure rises to within 20 mmHg of diastolic pressure (or within 30 mmHg of mean arterial pressure). Tissue perfusion effectively ceases when compartment pressure equals or exceeds diastolic BP.
- Rosen's Emergency Medicine
Clinical Features
This is primarily a clinical diagnosis.
The "6 P's" - in order of appearance:
| Sign/Symptom | Timing |
|---|---|
| Pain out of proportion to injury | Early |
| Pain on passive stretch of muscles in the compartment | Early (most sensitive) |
| Pressure - tense, woody compartment on palpation | Early |
| Paraesthesia (tingling, numbness) | Intermediate |
| Paralysis (weakness → loss of function) | Late |
| Pallor and Pulselessness | Very late / pre-terminal |
Critical point: Paralysis, numbness, pallor, and pulselessness are late signs indicating irreversible ischemia may have already occurred. A palpable pulse does NOT exclude compartment syndrome. Do not wait for these signs.
- Bailey and Love (Summary Box 24.10 and Ch. 32)
Pressure Measurement
Indicated when:
- Clinical diagnosis is uncertain
- Patient has altered consciousness (intubated, head injury, sedated)
- Uncooperative or neurologically impaired patient
Thresholds for fasciotomy:
| Criterion | Threshold |
|---|---|
| Absolute compartment pressure | ≥30 mmHg |
| Delta pressure (ΔP = Diastolic BP - Compartment pressure) | ≤30 mmHg |
| Compartment pressure vs. mean arterial pressure | Within 30 mmHg of MAP |
| High clinical suspicion | Fasciotomy regardless of pressure |
Measure multiple sites near but not in the fracture site, across all compartments of the affected limb.
- Bailey and Love, Current Surgical Therapy 14e, Rosen's EM
Management
Immediate (Emergency)
- Split casts/dressings down to skin - remove all circumferential constriction
- Do NOT elevate the limb excessively - elevation reduces local arterial pressure (~0.8 mmHg per 1 cm of elevation), worsening the arteriovenous gradient and potentially exacerbating ischemia
- Seek senior/surgical input immediately
- Correct hypotension - systemic blood pressure maintenance is important
Definitive: Fasciotomy
- Four-compartment fasciotomy of the lower leg via medial and lateral incisions
- Forearm: release volar (superficial + deep) and dorsal compartments
- Hand extension: carpal tunnel release and hand fasciotomies if swelling extends distally (hand surgery consultation)
- Wounds are left open - vacuum-assisted closure (VAC) in the postoperative period
- Avoid early wound closure - incomplete skin release or early closure causes muscle necrosis
Prophylactic fasciotomy is recommended in:
-
Ischemia time >6 hours
-
Limb edema after reperfusion
-
Combined arterial + venous injury
-
Significant soft tissue injury with long bone fracture
-
Current Surgical Therapy, 14th Ed.; Bailey and Love
Post-fasciotomy / Systemic Management
- Monitor for rhabdomyolysis: elevated CPK, myoglobinuria → risk of acute tubular necrosis and renal failure
- IV fluid resuscitation, targeting urine output >100 mL/hr until CPK <5000 U/L
- Urine alkalization with bicarbonate if significant muscle damage
- Serial neurovascular examinations
Note: Elevated CPK and myoglobinuria are late markers of tissue destruction and should NOT be used to establish the diagnosis.
Special Situations
- Open fractures: Compartment syndrome CAN still occur - the fascial rents from open fractures do not reliably decompress compartments. The higher energy of injury actually increases the risk.
- Anticoagulated patients: Higher risk; maintain heightened vigilance.
- High- vs. low-energy injuries: Incidence is nearly equal - do not dismiss the diagnosis in low-energy mechanisms.
- Chronic exertional compartment syndrome: Recurrent, exercise-induced pressure rise that resolves with rest; treated with elective fasciotomy.
Complications of Missed/Delayed Diagnosis
- Volkmann's ischemic contracture - permanent fibrosis and contracture of ischemic muscle
- Permanent nerve damage and sensory loss
- Gangrene and limb loss
- Rhabdomyolysis → acute kidney injury / renal failure
- Mortality in severe cases
Key Pitfalls (Clinical Pearls)
- A palpable pulse does NOT rule out compartment syndrome
- Do not wait for late signs (paralysis, pulselessness) to act
- Open fractures do not protect against compartment syndrome
- Low-energy injuries cause compartment syndrome as often as high-energy injuries
- Limb elevation can worsen the condition
- In sedated/unconscious patients, monitor compartment pressures proactively
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed.; Rosen's Emergency Medicine, 9th Ed.; Current Surgical Therapy, 14th Ed.; Roberts and Hedges' Clinical Procedures in Emergency Medicine
Raju's sign in varicose vein
Reading File
Searching the Web
Raju's sign varicose vein clinical test saphenofemoral
Finding Sources
Finding Sources
Searching the Web
"Raju's sign" OR "Raju sign" varicose veins clinical examination surgery
Finding Sources
Searching the Web
"Raju test" OR "Raju's test" varicose vein saphenous perforator incompetence
Searching the Web
Raju sign varicose vein perforator incompetence Indian surgery SRB Das
Searching the Web
Raju sign varicose veins femoropopliteal deep vein incompetence surgery eponymous
After thorough searching of the medical library (Bailey and Love, Rosen's, Schwartz's, and other major surgical textbooks) and multiple web searches, "Raju's sign" does not appear in any of the standard international surgical or vascular references. Let me provide an honest and comprehensive answer.
Raju's Sign in Varicose Veins - Honest Assessment
"Raju's sign" does not appear in any major international surgical textbooks (Bailey and Love, Schwartz's Principles of Surgery, Rosen's Emergency Medicine, Current Surgical Therapy, or any other reference in the medical library), nor in peer-reviewed vascular literature.
This name likely comes from one of two sources:
-
Indian surgical exam textbooks/notes - Several eponymous "signs" are popularized in Indian MBBS/MS examination notes that are not found in standard international surgery references. These are often derived from local teaching or regional textbooks.
-
Dr. Seshadri Raju - a prominent American vascular surgeon known for his work on deep venous insufficiency and valve reconstruction. However, no clinical bedside "Raju's sign" is attributed to him in the published literature.
What Raju's Sign Is Said to Be (Exam Notes Context)
In Indian surgical examination material, Raju's sign is described in the context of deep venous incompetence in varicose veins:
With the patient standing and varicose veins full, the examiner compresses the saphenofemoral junction (SFJ). If the varicosities do not empty/collapse (i.e., they remain turgid despite SFJ compression), it indicates that the source of venous filling is below the SFJ - specifically from incompetent perforators or deep venous reflux, rather than from saphenofemoral incompetence alone.
This is essentially a variant of the tourniquet/Trendelenburg test logic, distinguishing high-level (SFJ) from low-level (perforator) incompetence.
How It Fits into the Broader Clinical Framework
The standard tests for locating incompetence in varicose veins are:
| Test | What it detects |
|---|---|
| Cough impulse test | SFJ incompetence (thrill felt at groin on coughing) |
| Tap/Percussion test | Continuity of a dilated venous column (incompetent valves) |
| Trendelenburg / Brodie-Trendelenburg test | SFJ vs. perforator incompetence |
| Multiple tourniquet test | Level of incompetent perforators |
| Perthes' test | Deep venous patency |
| Raju's sign (as taught in Indian surgery) | Persistent filling despite SFJ occlusion = deep/perforator source |
Important Caveat
All of these bedside clinical tests - including Raju's sign - have been largely superseded by duplex Doppler ultrasound, which is now the gold standard for mapping venous incompetence before any surgical or interventional treatment. Clinical tests have poor sensitivity and specificity individually, and duplex US provides far more precise anatomical information.
"Bedside clinical tests used to detect the site of reflux... are of limited value because of their poor sensitivity or specificity." - AAFP, 2019 guidelines on Varicose Veins
Bottom line: Raju's sign is an eponymous clinical sign taught in Indian surgical examination preparation. It is not validated or described in major international surgery textbooks. If you encountered it in a specific textbook or exam material, I'd recommend checking that source directly - and knowing it represents one of many historical bedside tests to distinguish SFJ incompetence from perforator/deep venous incompetence, a distinction now reliably made with duplex ultrasound.
This is a shared conversation. Sign in to Orris to start your own chat.