Leukoplakia
Reading File
Finding Sources
Searching PubMed
leukoplakia oral AND malignant transformation
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have enough material for a thorough, well-structured answer. Let me compose it.
Leukoplakia
Definition
Leukoplakia is a clinical diagnosis of exclusion: a white patch or plaque of the oral mucosa that cannot be rubbed off and cannot be characterized as any other definable lesion or known disease (e.g., candidiasis, lichen planus, leukoedema, white sponge nevus). The white color arises because the thickened keratinized epithelium refracts light. It is the most common potentially malignant disorder of the oral mucosa.
- Cummings Otolaryngology, p. 1578
- Fitzpatrick's Dermatology, p. 1906
Epidemiology
| Feature | Detail |
|---|---|
| Global prevalence | 0.5% - 3.4% (up to 4.9% in India in adults >15 years) |
| Age | Most common in middle-aged and older individuals; rare below 30 |
| Sex | Male > female (2:1); rises to ~30% in men over 80 |
| Tobacco link | 6x more common in smokers; 73-81% of patients have tobacco history |
- Fitzpatrick's Dermatology, p. 1906; Cummings Otolaryngology, p. 1579
Etiology and Risk Factors
Primary etiologic factors:
- Tobacco (smoked and smokeless) - the strongest single risk factor; lesions may regress on cessation
- Alcohol - independent risk factor with synergistic effect alongside tobacco
- Areca (betel) nut - especially in South/Southeast Asia
- HPV (types 16 and 18) - detected in up to 22% of leukoplakia lesions; considered an independent or intensifying carcinogenic factor
- Chronic mechanical trauma - ill-fitting dentures, habitual cheek biting (produces frictional keratosis, which is not "true" leukoplakia as it reverses with removal of stimulus)
- Sun exposure (actinic cheilitis) - affects the lower lip vermilion
- Sanguinaria-containing products - leukoplakia along the maxillary alveolar mucosa
Paradoxically, leukoplakia in non-smokers is a higher-risk feature for malignant transformation (see Prognosis below).
- Fitzpatrick's Dermatology, pp. 1906-1907; Cummings Otolaryngology, p. 1759
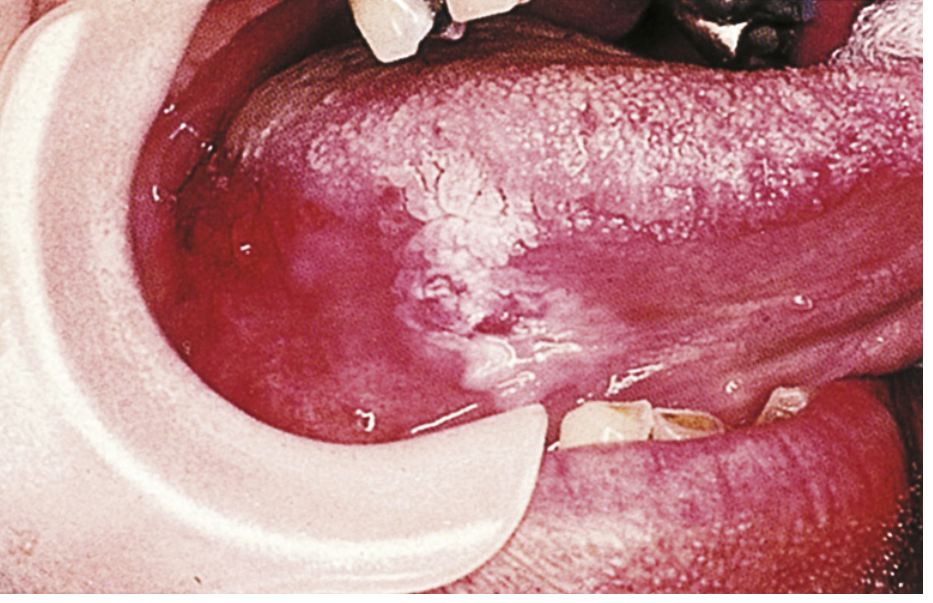
Clinical Features
Leukoplakia has a widely variable appearance:
Homogeneous (lower risk)
- Thin, flat, uniformly white plaque with a smooth, wrinkled, or corrugated surface
- Well- or ill-defined margins
- Tends to be asymptomatic
Non-homogeneous (higher risk)
- Speckled (erythroleukoplakia): white patches on an erythematous base - higher dysplasia risk; rebiopsy is mandatory if a lesion shifts to this pattern
- Nodular: small rounded white/red excrescences
- Verrucous/exophytic: surface projects above mucosa
- Ulcerative: erosion within the white lesion
Proliferative Verrucous Leukoplakia (PVL) - special subtype
- Multifocal, persistent, usually recurring
- Resembles verrucous carcinoma
- 70-87% of PVL cases progress to SCC
- Often occurs in patients who do not use tobacco
Common sites: buccal mucosa, gingiva, tongue (lateral/ventral), floor of mouth, lip vermilion. Tongue and floor-of-mouth locations carry the highest transformation risk.

- Cummings Otolaryngology, pp. 1579-1585; Sleisenger & Fordtran, p. 1014
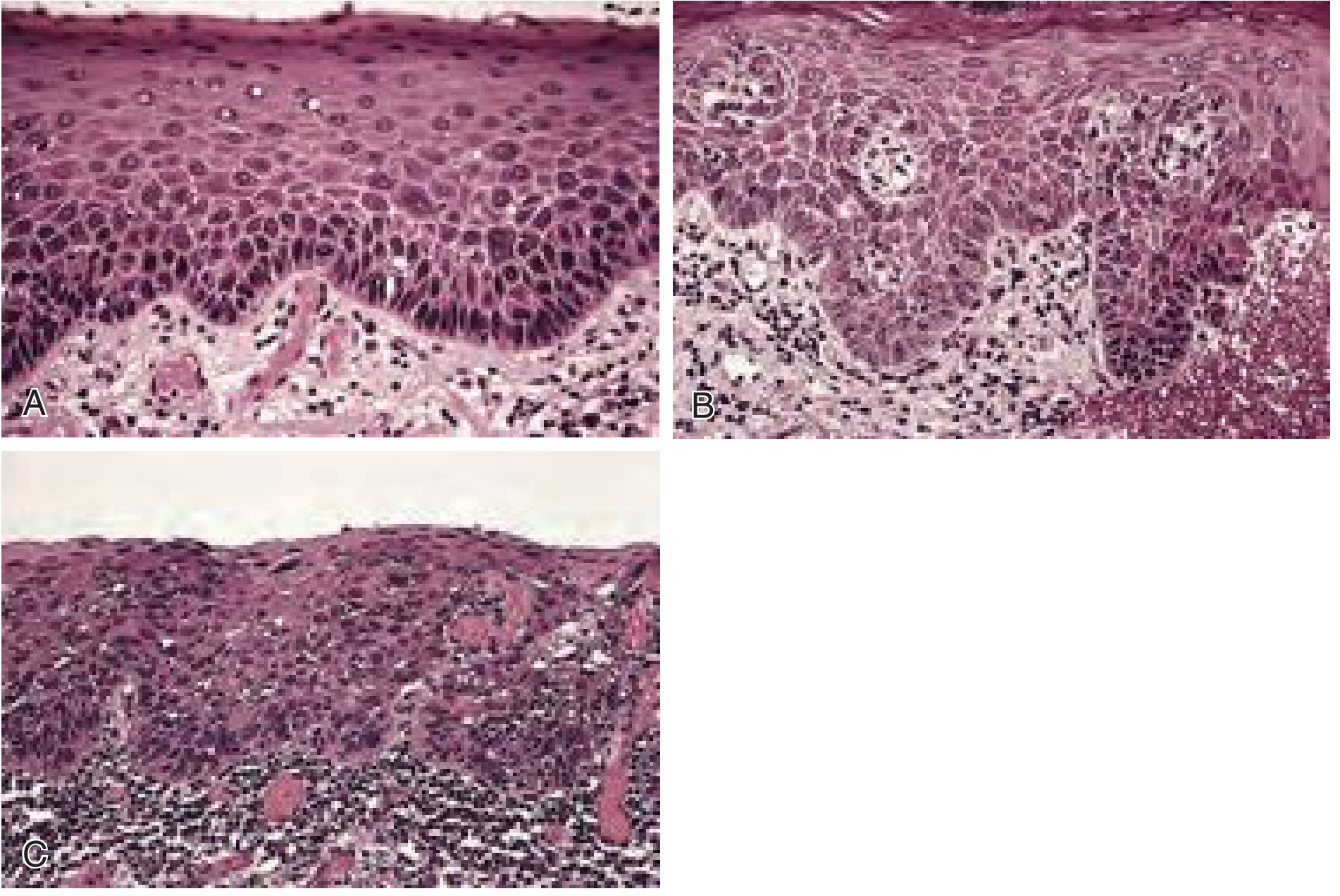
Histopathology
Microscopic findings range from benign hyperkeratosis to carcinoma in situ:
- Hyperkeratosis / parakeratosis with acanthosis - gives white color
- Epithelial dysplasia (mild, moderate, severe): cytologic atypia, increased mitoses (abnormal mitotic figures), loss of polarity, nuclear pleomorphism, hyperchromatism, loss of normal maturation
- Dysplasia is present in 3.7-28.7% of leukoplakias; older US studies found dysplasia, carcinoma in situ, and invasive SCC in 17-25% combined
- Carcinoma in situ: full-thickness ("top-to-bottom") epithelial atypia without basement membrane breach
- Invasive SCC: dysplastic cells breach the basement membrane
Grading of dysplasia (mild/moderate/severe) is the single most important histologic predictor of behavior.
- Cummings Otolaryngology, p. 1581; Fitzpatrick's, p. 1907; Robbins Pathology, p. 683
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Candidiasis (pseudomembranous) | Can be wiped off - leaves erythematous base |
| Oral hairy leukoplakia | Lateral tongue, vertical corrugations; EBV-driven; cannot be wiped off; immunocompromised |
| Lichen planus | Reticular/lacy white pattern; often bilateral; erosive variant; Wickham's striae |
| Leukoedema | Disappears on stretching the mucosa |
| White sponge nevus | Familial; widespread; no dysplasia |
| Lupus erythematosus | Central erythema with keratotic periphery |
| Verrucous carcinoma | Exophytic, already malignant |
| Linea alba | Thin white line on buccal mucosa at occlusal line; no treatment needed |
- Fitzpatrick's, p. 1907 (Table 110-8)
Malignant Transformation
- Overall annual transformation rate: ~2-3% per year (cumulative lifetime risk 0.13-34% across studies)
- ~50% of oral SCCs are associated with a pre-existing potentially malignant lesion
Risk factors for transformation to SCC:
Main risk factors:
- Presence of epithelial dysplasia (most important)
- Non-homogeneous clinical subtype (speckled, verrucous, nodular)
- Large size
- Location on tongue or floor of mouth
Other risk factors:
-
Female sex
-
Long duration
-
Leukoplakia in non-smokers (idiopathic leukoplakia)
-
Loss of heterozygosity at specific loci (useful for risk stratification)
-
Fitzpatrick's, p. 1907-1908 (Table 110-9); Goldman-Cecil Medicine, p. 23
Recent evidence (2025): A comprehensive systematic review and meta-analysis (Oral Dis 2025, PMID 39314164) confirmed and quantified malignant transformation rates. A separate meta-analysis (BMC Oral Health 2025, PMID 39893387) found 70-87% transformation in PVL specifically.
Hairy Leukoplakia (distinct entity)
-
Caused by EBV reactivation in immunosuppressed patients (HIV/AIDS, transplant recipients, hematologic malignancies)
-
White corrugated/fluffy ("hairy") plaques on the lateral border of the tongue - cannot be scraped off
-
Microscopy: hyperparakeratosis, acanthosis, "balloon cells" in the upper spinous layer; EBV RNA/proteins detectable
-
In HIV: median time to AIDS onset ~24 months; median time to death (pre-HAART) ~41 months
-
HAART has markedly decreased incidence
-
Treatment (if needed): acyclovir; often recurs after stopping
-
Robbins Pathology, p. 683; Cummings Otolaryngology, pp. 1582-1583
Diagnosis
- Clinical suspicion: white lesion that cannot be wiped off
- Eliminate causative agents (tobacco cessation, remove ill-fitting dentures) for 2-6 weeks; if regression occurs, not true leukoplakia
- Biopsy is mandatory if:
- No causative agent identified initially
- No regression after eliminating causative agents
- Lesion is symptomatic
- Lesion shifts to non-homogeneous morphology (rebiopsy)
- Multiple biopsies for extensive lesions; target most clinically suspicious areas (erythematous, granular, ulcerated, indurated)
- Histologic grading of dysplasia guides management
- Fitzpatrick's, p. 1907; Cummings Otolaryngology, p. 1580
Management
| Histology | Management |
|---|---|
| No dysplasia / mild dysplasia | Observation vs. elective excision; eliminate risk factors |
| Moderate dysplasia | Removal mandatory |
| Severe dysplasia / CIS | Removal mandatory; consider wider margins |
| Invasive SCC | Oncologic surgery |
Modalities for removal:
- Scalpel excision (preferred - allows complete histology, may identify unexpected carcinoma)
- CO2 laser ablation
- Electrocautery
- Cryotherapy (useful for recurrence after surgery)
- Photodynamic therapy (PDT)
Key caveat - field cancerization: Normal-appearing mucosa surrounding leukoplakia may harbor genetically abnormal cells; complete excision does not eliminate transformation risk, and recurrence rates are high regardless of modality.
Chemoprevention: Retinoids, antioxidants (beta-carotene, vitamin A), and COX-2 inhibitors have been studied but no agent has proven efficacy in preventing malignant transformation in RCTs.
Follow-up: Lifelong surveillance is required regardless of treatment, given the risk of recurrence and transformation at same or other sites.
- Cummings Otolaryngology, pp. 1580-1581; Fitzpatrick's, p. 1908
Summary Table
| Feature | Homogeneous | Non-homogeneous | PVL |
|---|---|---|---|
| Appearance | Flat, uniform white | Speckled, verrucous, nodular | Multifocal, verrucous, spreading |
| Dysplasia risk | Lower | Higher | Very high |
| Malignant transformation | ~2-3%/year overall | Higher than homogeneous | 70-87% |
| Tobacco association | Common | Common | Often absent |
Sources: Cummings Otolaryngology Head and Neck Surgery, pp. 1578-1585 | Fitzpatrick's Dermatology, pp. 1906-1908 | Robbins Pathologic Basis of Disease, p. 683 | Sleisenger & Fordtran's GI and Liver Disease, pp. 998-1020 | Goldman-Cecil Medicine, p. 23
This is a shared conversation. Sign in to Orris to start your own chat.