Explain in detail the HMP Pathway & its’ Clinical Significance
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pentose phosphate pathway" AND "clinical significance"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full detailed answer.
The Hexose Monophosphate (HMP) Pathway - A Detailed Overview
The Hexose Monophosphate (HMP) Pathway - also called the Pentose Phosphate Pathway (PPP) or Phosphogluconate Pathway - is an alternative route of glucose metabolism that runs parallel to glycolysis in the cytosol. Unlike glycolysis, it neither produces nor consumes ATP, but it serves two critical purposes: generation of NADPH (the cell's primary reducing power) and synthesis of ribose 5-phosphate (for nucleotide biosynthesis).
About 10% of cellular glucose is channeled through this pathway; the remaining 90% goes through glycolysis.
Pathway Overview
The HMP pathway has two distinct phases:
| Feature | Oxidative Phase | Nonoxidative Phase |
|---|---|---|
| Reversibility | Irreversible | Reversible |
| Products | NADPH, CO2, ribulose 5-P | Ribose 5-P, glycolytic intermediates |
| Key enzymes | G6PD, 6-PGD | Transketolase, Transaldolase |
Here is the detailed reaction diagram from Lippincott's Illustrated Reviews in Biochemistry:
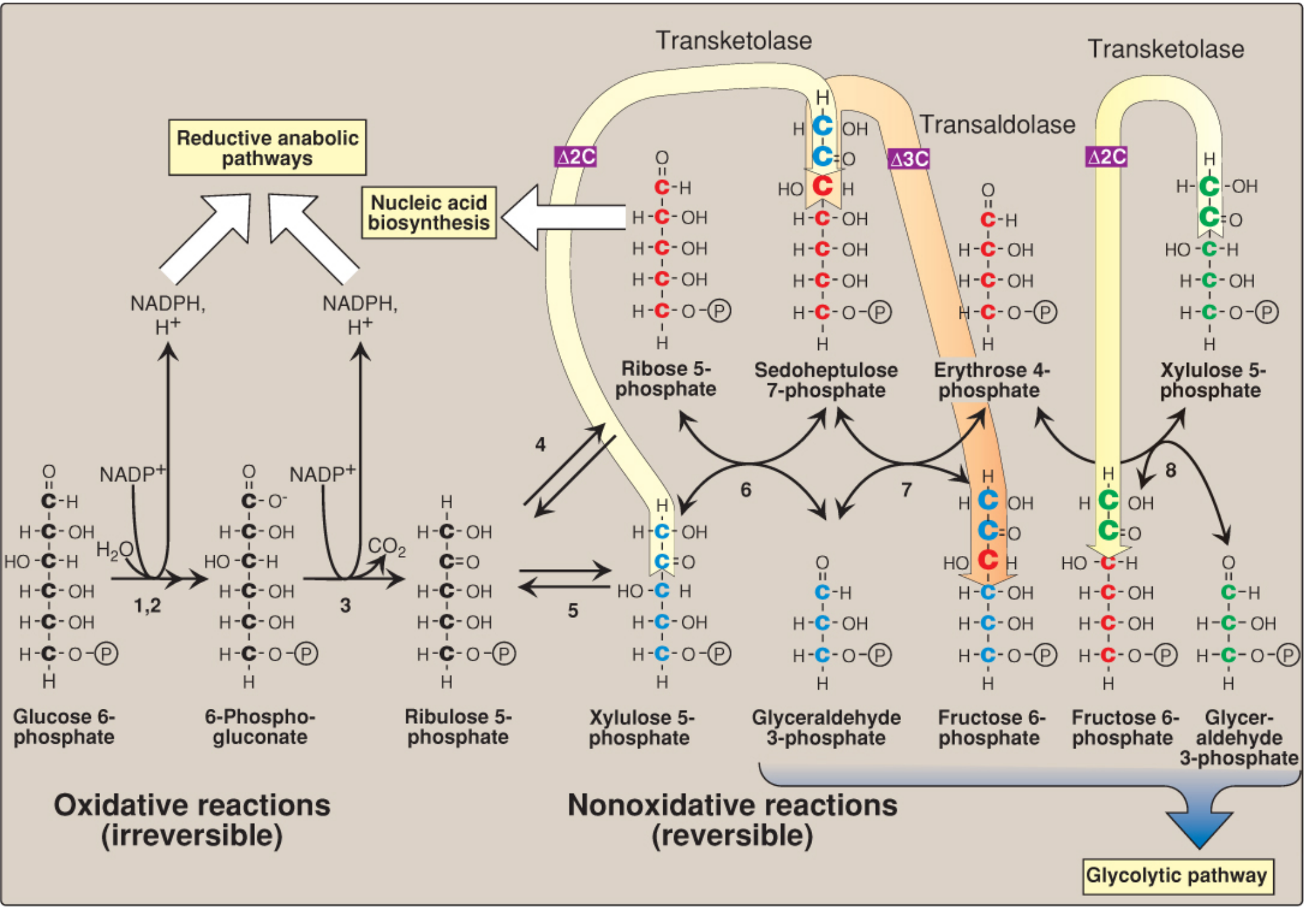
Phase 1: The Oxidative (Irreversible) Reactions
This phase consists of three irreversible reactions that convert glucose 6-phosphate into ribulose 5-phosphate, releasing CO2 and generating 2 NADPH per glucose 6-phosphate oxidized.
Step 1 - Glucose 6-Phosphate Dehydrogenase (G6PD)
- Glucose 6-phosphate + NADP⁺ → 6-phosphogluconolactone + NADPH + H⁺
- This is the committed, rate-limiting, and regulated step of the entire pathway
- G6PD is strongly inhibited by NADPH (product inhibition); when the NADPH/NADP⁺ ratio is high, the pathway is suppressed
- When NADPH is consumed (e.g., in oxidative stress), NADP⁺ rises, relieving inhibition and accelerating the pathway
- Insulin upregulates G6PD gene expression, increasing pathway flux in the absorptive (fed) state
- The enzyme requires Mg²⁺ as a cofactor
Step 2 - Gluconolactone Hydrolase
- 6-Phosphogluconolactone + H₂O → 6-phosphogluconate
- Spontaneous hydrolysis, but accelerated by this hydrolase
Step 3 - 6-Phosphogluconate Dehydrogenase (6-PGD)
- 6-Phosphogluconate + NADP⁺ → Ribulose 5-phosphate + CO₂ + NADPH + H⁺
- This is an oxidative decarboxylation - carbon 1 of glucose is released as CO₂
- Produces the second NADPH molecule
- Net from the oxidative phase: 2 NADPH + 1 CO₂ + 1 ribulose 5-phosphate per glucose 6-phosphate
Phase 2: The Nonoxidative (Reversible) Reactions
Ribulose 5-phosphate (a ketopentose) is the entry point. It can be converted to:
- Ribose 5-phosphate (by ribose 5-phosphate isomerase) - for nucleotide synthesis
- Xylulose 5-phosphate (by phosphopentose epimerase) - to enter the carbon-shuffling reactions
The carbon shuffling is carried out by two key enzymes that interconvert 3C, 4C, 5C, 6C, and 7C sugar phosphates:
Transketolase (requires Thiamine Pyrophosphate - TPP)
- Transfers 2-carbon units from a ketose donor to an aldose acceptor
- Reaction 1: Xylulose 5-P (5C) + Ribose 5-P (5C) → Sedoheptulose 7-P (7C) + Glyceraldehyde 3-P (3C)
- Reaction 2: Xylulose 5-P (5C) + Erythrose 4-P (4C) → Fructose 6-P (6C) + Glyceraldehyde 3-P (3C)
Transaldolase
- Transfers 3-carbon units from a ketose donor to an aldose acceptor
- Sedoheptulose 7-P (7C) + Glyceraldehyde 3-P (3C) → Fructose 6-P (6C) + Erythrose 4-P (4C)
Net outcome of combined phases (for 3 glucose 6-phosphate molecules):
3 Glucose 6-P + 6 NADP⁺ → 3 CO₂ + 6 NADPH + 6 H⁺ + 2 Fructose 6-P + Glyceraldehyde 3-P
The fructose 6-phosphate and glyceraldehyde 3-phosphate re-enter glycolysis or can be converted back to glucose 6-phosphate (via gluconeogenic enzyme fructose 1,6-bisphosphatase), allowing the pathway to completely oxidize glucose to CO₂ and water while generating 12 NADPH.
Regulation of the HMP Pathway
| Regulator | Effect |
|---|---|
| High NADPH/NADP⁺ ratio | Inhibits G6PD (product inhibition) - slows pathway |
| Oxidative stress (↑ NADP⁺) | Activates G6PD - accelerates NADPH production |
| Insulin (fed state) | Induces G6PD gene expression - increases pathway flux |
| Xylulose 5-phosphate | Activates protein phosphatase → ↑ phosphofructokinase activity → links HMP to glycolysis; also upregulates lipogenic gene expression |
Tissue Distribution
The pathway is highly active in tissues with high demand for NADPH or ribose:
| Tissue | Primary Use |
|---|---|
| Liver, adipose tissue | Fatty acid and cholesterol synthesis (reductive biosynthesis) |
| Adrenal cortex, gonads, placenta | Steroid hormone synthesis |
| Erythrocytes | Maintenance of reduced glutathione (antioxidant defense) |
| Activated phagocytes (neutrophils, macrophages) | NADPH oxidase-driven respiratory burst |
| Lactating mammary gland | Fatty acid synthesis for milk lipids |
| Lens of the eye | Protection against oxidative damage |
| All proliferating cells | Ribose 5-phosphate for nucleotide/nucleic acid synthesis |
The pathway is low in skeletal muscle (though muscle can still generate ribose 5-phosphate by running the nonoxidative reactions in reverse from fructose 6-phosphate).
Key Products and Their Uses
1. NADPH
NADPH is the cell's primary reductant and has multiple critical roles:
- Reductive biosynthesis: fatty acid synthesis (via fatty acid synthase), cholesterol synthesis (via HMG-CoA reductase), amino acid synthesis
- Glutathione system: reduces oxidized glutathione (GSSG → GSH) via glutathione reductase
- Cytochrome P450 reactions: drug detoxification and steroid hydroxylation in liver
- NADPH oxidase: generates superoxide (O₂⁻) in phagocytes for microbial killing
- Nitric oxide synthesis: NO synthase requires NADPH
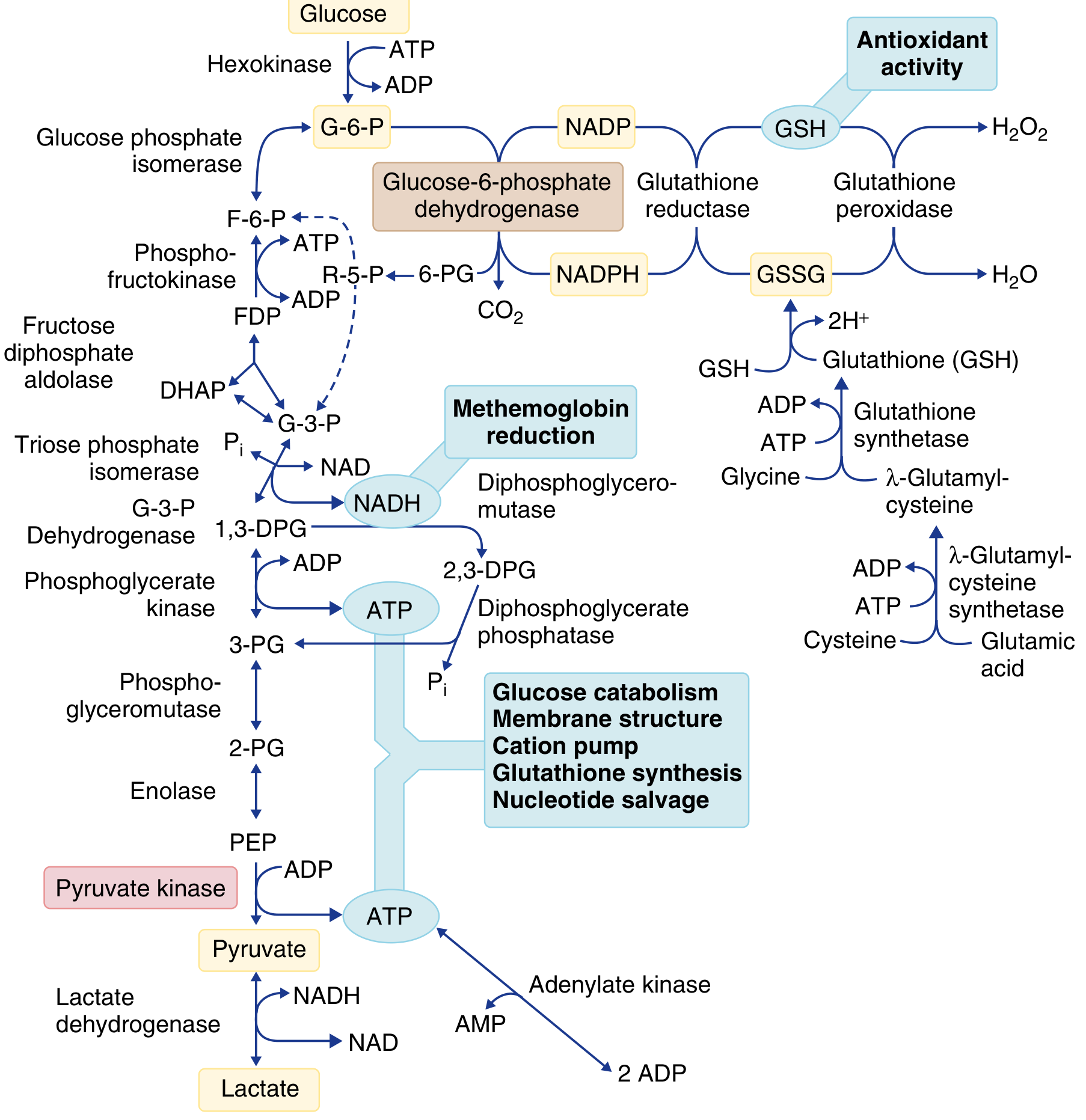
Here is the erythrocyte metabolism diagram showing the HMP shunt's role in antioxidant defense and its connection to glycolysis:
2. Ribose 5-Phosphate
- Precursor for purine and pyrimidine nucleotide synthesis (ATP, GTP, UTP, CTP, NAD⁺, FAD, CoA)
- Required for DNA and RNA synthesis in all proliferating cells
- Little ribose circulates in the bloodstream, so all tissues synthesize their own via this pathway
The Glutathione System - Bridge to Clinical Disease
The HMP pathway is the sole source of NADPH in red blood cells (RBCs lack mitochondria). NADPH is essential for regenerating reduced glutathione (GSH) from its oxidized form (GSSG):
GSSG + NADPH + H⁺ →[Glutathione reductase]→ 2 GSH + NADP⁺
GSH + H₂O₂ →[Glutathione peroxidase (Se-enzyme)]→ GSSG + 2H₂O
GSH neutralizes hydrogen peroxide (H₂O₂), superoxide anions (O₂⁻), and hydroxyl radicals (OH•) produced during:
- Normal oxidative metabolism of heme
- Exposure to oxidant drugs or chemicals
- Infection and phagocyte activation
Without adequate NADPH, GSH is depleted, and the RBC becomes defenseless against oxidative damage.
Clinical Significance
1. Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency - The Most Important Clinical Condition
G6PD deficiency is the most common inherited disorder of erythrocyte metabolism, affecting over 400 million people worldwide. It is X-linked (gene at Xq28), so it predominantly affects males.
Why RBCs are uniquely vulnerable: The HMP shunt is the only source of NADPH in mature erythrocytes (no mitochondria, no malic enzyme). Without NADPH, glutathione cannot be regenerated, and oxidative damage accumulates.
Pathophysiology of hemolysis:
- Oxidant exposure → H₂O₂ and free radicals accumulate
- GSH depleted → unable to neutralize oxidants
- Hb sulfhydryl groups oxidized → methemoglobin + intracellular Hb precipitates (Heinz bodies)
- Heinz bodies attach to RBC membrane → clustering of immunoglobulins and band 3 protein → opsonization and phagocytic removal
- Membrane phospholipid peroxidation + spectrin cross-linking → decreased membrane deformability → splenic trapping and hemolysis
- "Bite cells" appear on peripheral blood smear during acute episodes (from Heinz body removal by the spleen)
Common G6PD Variants:
| Variant | Population | Enzyme Activity | Severity |
|---|---|---|---|
| G6PD B (normal) | Worldwide | 100% | None |
| G6PD A+ | Africa | 85% | None |
| G6PD A- | Africa (~10% of African Americans) | 10-23% | Mild-moderate (WHO Class III) |
| G6PD Mediterranean | Middle East, S. Asia | <5% | Severe (WHO Class II) |
| G6PD Canton | Southeast Asia / China | ~4% | Moderate-severe |
| G6PD Mahidol | Southeast Asia | 0.6% | Severe (WHO Class II) |
The G6PD A- variant has a half-life of only 13 days (vs. ~60 days for normal G6PD B), so young RBCs have near-normal activity but older RBCs are severely deficient. This limits the degree of hemolysis in an acute episode.
Evolutionary significance: G6PD deficiency is so prevalent because G6PD-deficient RBCs confer protection against Plasmodium falciparum malaria - the parasite cannot survive optimally in oxidatively stressed RBCs.
Clinical Syndromes:
a) Acute Hemolytic Anemia - triggered by oxidant stress:
- Infections (most common trigger, via phagocyte-derived oxidants)
- Drugs: primaquine, dapsone, rasburicase, nitrofurantoin, sulfonamides, chloroquine
- Foods: fava beans (favism - due to vicine and convicine)
- Chemicals: naphthalene (moth balls), methylene blue, phenylhydrazine, dimercaprol (BAL)
- Metabolic acidosis
b) Neonatal Jaundice - onset typically days 2-3 of life; can be severe with risk of kernicterus. Worsened by concurrent Gilbert syndrome (UDPGT1 polymorphism). Rarely accompanied by significant anemia.
c) Chronic Non-Spherocytic Hemolytic Anemia (CNSHA) - caused by rare severe G6PD variants that cannot maintain basal NADPH production even without oxidant stress. Some patients require intermittent transfusions.
Diagnosis:
- Screening: Fluorescent spot test (NADPH fluoresces under UV light) - high sensitivity but semiquantitative
- Definitive: Spectrophotometric measurement of NADPH production rate
- Note: Testing during/shortly after hemolytic crisis may give false-negative results (young cells with more G6PD are reticulocytes)
- Cyanide-ascorbate test can detect female heterozygotes (can identify as few as 10-15% deficient cells)
2. Chronic Granulomatous Disease (CGD)
- Caused by NADPH oxidase deficiency in phagocytes
- NADPH from the HMP pathway normally powers the respiratory burst in neutrophils/macrophages
- Without functional NADPH oxidase: O₂⁻ is not generated → H₂O₂ → HOCl chain fails → bacteria not killed
- Results in recurrent, severe infections with catalase-positive organisms (Staphylococcus, Aspergillus, etc.) and formation of granulomas
- X-linked (most common form, gp91phox subunit) or autosomal recessive
3. Transketolase Deficiency - Wernicke-Korsakoff Syndrome
- Transketolase requires thiamine pyrophosphate (TPP) as coenzyme
- Thiamine (B1) deficiency impairs the nonoxidative phase of the HMP pathway
- Clinically manifests as Wernicke's encephalopathy (ophthalmoplegia, ataxia, confusion) and Korsakoff's psychosis (anterograde amnesia, confabulation)
- Erythrocyte transketolase activity is used as a biomarker for thiamine status in the TPP effect test
4. Favism
- A form of acute hemolysis in G6PD-deficient individuals after ingestion of fava beans (Vicia faba)
- The beans contain vicine and convicine, which are hydrolyzed to divicine and isouramil - potent oxidizing agents
- More severe in G6PD Mediterranean variant than G6PD A-
5. Drug Interactions and Pharmacogenomics
Because the HMP pathway is critical for protecting RBCs from oxidant damage, G6PD deficiency must be screened before prescribing certain drugs:
- Rasburicase (used for tumor lysis syndrome): contraindicated in G6PD deficiency - causes severe hemolysis
- Primaquine, tafenoquine (antimalarials): known hemolytic agents in G6PD-deficient patients; G6PD testing now required before tafenoquine use
- Dapsone (used in leprosy, PCP prophylaxis)
- High-dose aspirin, nitrofurantoin, sulfonamides
6. Cancer Metabolism
The HMP pathway is upregulated in many rapidly proliferating cancer cells, which have high demand for both NADPH (to manage oxidative stress and support lipid synthesis) and ribose 5-phosphate (for nucleotide synthesis). The pathway is considered a potential therapeutic target.
7. Diabetes Mellitus - Indirect Connection
Chronic hyperglycemia drives excess glucose through aldose reductase (polyol pathway), consuming NADPH in the process. This depletes the NADPH available for glutathione regeneration, contributing to oxidative damage in lens (cataracts), peripheral nerves (neuropathy), and retinal microvessels (retinopathy).
Comparison: HMP Pathway vs. Glycolysis
| Feature | HMP Pathway | Glycolysis |
|---|---|---|
| Location | Cytosol | Cytosol |
| Coenzyme | NADP⁺/NADPH | NAD⁺/NADH |
| ATP production | None | Yes (net 2 ATP) |
| CO₂ production | Yes (from C1) | No |
| Products | NADPH, ribose 5-P | Pyruvate, ATP, NADH |
| Regulation | G6PD by NADPH/NADP⁺ | PFK-1 by ATP/AMP |
| Key tissues | Liver, RBC, phagocytes, gonads | All tissues |
Summary of Key Clinical Points
| Condition | HMP Defect | Mechanism | Consequence |
|---|---|---|---|
| G6PD deficiency | G6PD enzyme | ↓ NADPH → ↓ GSH → oxidative hemolysis | Acute hemolysis, neonatal jaundice, CNSHA |
| Favism | G6PD (triggered by fava beans) | Exogenous oxidants + ↓ NADPH | Acute hemolytic crisis |
| Chronic granulomatous disease | NADPH oxidase (uses NADPH from HMP) | No respiratory burst | Recurrent infections, granulomas |
| Wernicke-Korsakoff | Transketolase (B1 deficiency) | Nonoxidative phase failure | Encephalopathy, amnesia |
| Neonatal jaundice (G6PD) | G6PD | ↓ NADPH → hemolysis → hyperbilirubinemia | Kernicterus risk |
Sources: Harper's Illustrated Biochemistry, 32nd Ed.; Lippincott Illustrated Reviews: Biochemistry, 8th Ed.; Basic Medical Biochemistry: A Clinical Approach, 6th Ed.; Goldman-Cecil Medicine, International Edition; Henry's Clinical Diagnosis and Management by Laboratory Methods; Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.