Leishman stain procedure
Reading File
Finding Sources
Searching the Web
Leishman stain procedure steps principle uses
Reading File
I now have enough information to give a thorough answer.
Leishman Stain - Complete Procedure
Background
Leishman stain was developed by William Boog Leishman in 1901. It is a Romanowsky-type polychromatic stain based on a methanolic mixture of polychrome methylene blue (azure B - basic dye) and eosin Y (acidic dye). It belongs to the same family as Giemsa, Wright's, Jenner's, and May-Grunwald stains.
- Henry's Clinical Diagnosis and Management by Laboratory Methods notes that Romanowsky-type stains include "Giemsa, Leishman's, Jenner's, May-Grunwald, MacNeal's, and various combinations."
Principle
The stain works through differential affinity of acidic and basic dyes:
| Cell Component | Dye | Resulting Color |
|---|---|---|
| Nucleus / nucleic acids (acidic) | Methylene blue/Azure B (basic dye) | Blue to purple |
| Cytoplasm, eosinophil granules (basic) | Eosin (acidic dye) | Pink to red |
| Neutrophil granules | Both dyes | Lilac/violet |
| Red blood cells | Eosin | Pink-orange |
Methanol in the stain serves a dual purpose:
- Acts as a fixative - prevents cell distortion and makes cells adhere to the slide
- Acts as a solvent for the dye components
The "Romanowsky effect" (azure-eosin interaction) produces the characteristic polychromatic staining that differentiates cell types.
Preparation of Leishman Stain Solution
Stock solution (0.15 g/100 mL):
- Leishman stain powder: 0.15 g
- Methanol (absolute, acetone-free): 100 mL
- Dissolve powder in methanol; filter before use
- Mature the stain by leaving it at room temperature for 1-2 weeks (or place in a water bath at 37°C for 24 hrs to accelerate)
Buffer (pH 6.8-7.0):
- Phosphate buffer at pH 6.8-7.0 (or pH 6.4 for malaria smears)
- Alternatively, use clean distilled water
Standard Procedure (Flood Slide Method)
Step 1 - Prepare the Blood Film
- Collect blood (finger prick or EDTA anticoagulated)
- Make a thin peripheral blood smear on a clean, grease-free glass slide
- Air dry completely - do not heat fix
Step 2 - Fix and Stain (Initial Flooding)
- Place the slide horizontally on a staining rack
- Flood the slide with Leishman stain (approx. 15-20 drops)
- Allow to act for 1-3 minutes (the methanol fixes the smear simultaneously)
- Do NOT rinse
Step 3 - Add Buffer Water (Dilution Step)
- Add double the volume of buffered distilled water (or phosphate buffer pH 6.8-7.0) directly on top of the stain
- Gently rock the slide or blow on it to mix
- Allow the diluted stain to act for 10-15 minutes
- A greenish metallic sheen should appear on the surface - this confirms adequate staining
Step 4 - Wash
- Wash with a gentle stream of buffered water (distilled water) until the slide acquires a pinkish tint
- Hold the slide horizontally during initial washing to prevent uneven washing
- Do NOT wash too vigorously
Step 5 - Dry and Examine
- Drain excess water and allow to air dry in an upright position
- Do NOT blot with paper (may cause scratches)
- Examine under oil immersion (100x objective)
Simplified Procedure Summary
| Step | Action | Time |
|---|---|---|
| 1 | Air-dry blood film | Until completely dry |
| 2 | Flood with Leishman stain | 1-3 min (fixation + initial staining) |
| 3 | Add double volume buffer water, mix | 10-15 min |
| 4 | Wash with buffered water | Until pinkish |
| 5 | Air dry and examine | - |
Staining Results (Expected Colors)
| Structure | Color |
|---|---|
| RBC | Pink-orange |
| Neutrophil nucleus | Dark purple/violet |
| Neutrophil granules | Lilac/pale pink |
| Eosinophil granules | Bright red-orange |
| Basophil granules | Dark blue-black |
| Monocyte nucleus | Blue-purple (kidney-shaped) |
| Lymphocyte nucleus | Deep purple |
| Platelet granules | Purple |
| Malarial parasites (ring forms) | Blue cytoplasm, red chromatin dot |
| Leishman-Donovan bodies (amastigotes) | Blue-purple |
Uses / Applications
- Routine peripheral blood smear - differential WBC count, morphology
- Malarial parasite identification - ring forms, trophozoites, gametocytes
- Trypanosomes in blood
- Bone marrow aspirate examination
- Leishmania (Leishman-Donovan bodies) - intracellular amastigotes in macrophages
- Other haemoparasites - Babesia, microfilariae
Common Staining Problems and Corrections
| Problem | Cause | Correction |
|---|---|---|
| Excessively blue stain | Thick film, prolonged staining, insufficient washing, high pH buffer | Shorten staining time, use less stain, lower pH buffer |
| Excessively pink stain | Insufficient staining, prolonged washing, acidic buffer (formic acid from oxidized methanol) | Increase staining time, use fresh methanol, raise pH |
| Precipitate on film | Dirty slides, stain drying during procedure, inadequate filtration | Use clean slides, keep slide wet, filter stain |
| Uneven staining | Uneven flooding, bubbles under stain | Ensure even flooding, remove bubbles |
Comparison with Other Romanowsky Stains
| Feature | Leishman | Wright | Giemsa |
|---|---|---|---|
| pH of buffer | 6.8-7.0 | 6.4-6.8 | 7.2 |
| Preferred use | General hematology, parasites | General hematology (routine) | Malaria, protozoa |
| Fixation | Built-in (methanol) | Built-in (methanol) | Separate fixation needed |
| Staining time | 10-15 min | 3-5 min | 20-45 min |
Leishman's stain is a versatile, reliable stain for both routine hematology and parasitology, with the convenience of built-in fixation making it practical for most laboratory settings.
Anaplastic large cell lymphoma FNAC microscopy description
Finding Sources
Finding Sources
Searching the Web
anaplastic large cell lymphoma FNAC cytology microscopy description hallmark cells
Finding Sources
Reading Web Page
https://www.pathologyoutlines.com/topic/lymphomanonbanaplast…
Reading File
Reading Web Page
https://www.jsltr.org/journal/57-3/P120-142_17023.pdf
I now have comprehensive information to give a detailed FNAC microscopy description of ALCL. Here is the full answer:
Anaplastic Large Cell Lymphoma (ALCL) - FNAC Microscopy Description
Overview
ALCL is an aggressive CD30+ T-cell non-Hodgkin lymphoma that characteristically presents with lymphadenopathy. FNAC (fine needle aspiration cytology) of involved lymph nodes typically yields a highly cellular aspirate with a distinctive and diagnostically recognizable cytomorphology.
FNAC Smear - General Features
- Cellularity: Highly cellular smear
- Background: Necrotic background may be present; lymphoglandular bodies usually sparse or absent (unlike reactive lymphadenopathy)
- Discohesion: Cells tend to appear loosely cohesive or in small clusters - cohesive grouping can mimic metastatic carcinoma
- Tissue fragments: Occasional loosely cohesive aggregates of large cells packing sinusoidal spaces
The Hallmark Cells (Pathognomonic Feature)
The "hallmark cell" is the defining cytological feature of ALCL (first described by Benharroch et al., also termed by Delsol):
Nuclear Features
- Large cells - significantly larger than normal lymphocytes
- Nuclei are bizarrely shaped: horseshoe-shaped, kidney-shaped, embryo-shaped, or lobulated
- Eccentric nucleus with a characteristic paracentral indentation or folded nuclear contour
- Open/vesicular chromatin (pale, finely granular)
- Multiple prominent nucleoli - often 1-3 large eosinophilic nucleoli
- Some cells show wreath-like or ring nuclei (nuclei arranged around the periphery of the cell)
- Reed-Sternberg-like cells (binucleate or multinucleate) may be seen
- "Donut cells" - cells with nuclear pseudoinclusions (nucleus appearing to have a hole)
Cytoplasmic Features
- Abundant cytoplasm - much more than typical lymphomas
- Cytoplasm is pale, amphophilic to basophilic (gray-blue on H&E/Giemsa)
- Prominent paranuclear Golgi zone - appears as a clear or slightly eosinophilic region adjacent to the nucleus (perinuclear eosinophilic hof)
- Cytoplasmic borders are distinct
Cell Populations in FNAC Smear
| Cell Type | Description |
|---|---|
| Hallmark cells | Large, horseshoe/kidney nucleus, abundant pale cytoplasm, prominent Golgi - always present in all variants |
| Reed-Sternberg-like cells | Binucleate or multinucleate with prominent nucleoli |
| Wreath cells | Multiple nuclei arranged in a wreath pattern |
| Donut cells | Nuclear pseudoinclusion giving a "donut" appearance |
| Small-medium cells | Variable depending on morphological variant |
| Background cells | Varies by variant (histiocytes, lymphocytes, neutrophils) |
Morphological Variants and Their FNAC Appearance
1. Common (Typical) Pattern (~70%)
- Sheets of large hallmark cells
- Diffuse effacement of lymph node architecture
- Cells pack the sinuses - sinus infiltration pattern (in ~75% of cases)
- Most recognizable pattern on FNAC
2. Lymphohistiocytic Variant
- Neoplastic hallmark cells are overshadowed by numerous histiocytes with pale/eosinophilic cytoplasm
- FNAC can be misleading - appear as histiocyte-rich smear
- Small lymphocytes and plasma cells in background
- Hallmark cells tend to cluster around blood vessels
- Most commonly misdiagnosed variant
3. Small Cell Variant
- Predominant population of small to medium cells with irregular nuclei and pale cytoplasm
- Hallmark cells present but sparse - tend to be perivascular
- Occasional "fried egg cells" and rare signet ring cells
- Can mimic peripheral T-cell lymphoma NOS
4. Hodgkin-like (1-3%)
- Resembles nodular sclerosis classic Hodgkin lymphoma
- Mononuclear cells predominate
- Binucleate Reed-Sternberg-like cells and mummified cells
- Eosinophils and neutrophils present but less than in classic HL
5. Sarcomatoid Variant
- Spindle-shaped or bizarre sarcomatoid cells
- May mimic soft tissue sarcoma
Key Diagnostic Clues on FNAC
- Hallmark cell morphology - horseshoe/kidney-shaped nucleus + abundant cytoplasm + Golgi zone = strongly suggestive
- Sinusoidal infiltration - clusters of large cells mimicking metastatic carcinoma
- Perivascular clustering of tumor cells
- Brisk mitotic activity - numerous mitoses and apoptotic cells
- Absence of typical lymphoid cell pattern - no germinal center cells, no tingible body macrophages
Differential Diagnosis on FNAC
| Condition | Differentiating Feature |
|---|---|
| Metastatic carcinoma | ALCL cells are cohesive but lack true intercellular bridges; cytokeratin negative; CD30+/ALK+ |
| Classic Hodgkin Lymphoma | RS cells in mixed inflammatory background; CD15+, CD30+, PAX5+; ALK- |
| Diffuse Large B-cell Lymphoma | Less pleomorphic; CD20+, CD79a+; CD30 usually negative |
| Peripheral T-cell Lymphoma NOS | No hallmark cells; CD30 weak/negative; ALK negative |
| Reactive lymphadenopathy | Polymorphous population; tingible body macrophages; follicular pattern |
Immunocytochemistry on FNAC Cell Block
| Marker | ALCL (ALK+) | ALCL (ALK-) |
|---|---|---|
| CD30 | Strongly + (membrane + Golgi) | Strongly + |
| ALK | + (nuclear + cytoplasmic with t(2;5)) | Negative |
| EMA | + | +/- |
| CD2, CD4 | + | +/- |
| CD3, CD5 | Variable loss | Variable loss |
| CD20, CD79a | Negative | Negative |
| CD15 | Negative | Negative |
| PAX5 | Negative | Negative |
| Cytokeratin | Negative | Negative |
Summary: FNAC Diagnostic Statement
A typical FNAC report would read:
"Smear shows a highly cellular aspirate comprising large pleomorphic lymphoid cells with hallmark cell morphology - cells having eccentric, horseshoe/kidney-shaped or lobulated nuclei, open chromatin, prominent nucleoli, and abundant pale cytoplasm with a conspicuous perinuclear Golgi zone. Reed-Sternberg-like cells and wreath cells are also noted. Brisk mitotic activity is present. Background shows scattered small lymphocytes. Findings are consistent with Anaplastic Large Cell Lymphoma. Immunocytochemistry/immunohistochemistry recommended for confirmation and ALK status."
Sources: Pathology Outlines - ALK+ ALCL | JSLTR - ALCL Review | Goldman-Cecil Medicine, Anaplastic Large Cell Lymphoma section | Modern Pathology - ALCL Histologic Spectrum
What is perinuclear golgi zone
Finding Sources
Searching the Web
perinuclear Golgi zone cytology microscopy appearance significance
Reading File
Finding Sources
Loading Image
Perinuclear Golgi Zone
What It Is
The perinuclear Golgi zone (also called the paranuclear hof, from the German word meaning "courtyard" or "halo") is a pale, clear or lightly eosinophilic area in the cytoplasm that sits immediately adjacent to the nucleus. It corresponds directly to the anatomical location of the Golgi apparatus within the cell.
Why It Appears Pale on Light Microscopy
The Golgi apparatus is a stack of flattened membranous sacs (cisternae) involved in protein processing, packaging, and secretion. This region appears lighter/clearer than the surrounding cytoplasm because:
- It lacks the ribosomes and rough endoplasmic reticulum that give surrounding cytoplasm its basophilic (blue) color
- It is relatively devoid of RNA (which is what methylene blue/haematoxylin stains)
- The membranous cisternae of the Golgi itself do not take up standard stains strongly
So on Romanowsky stains (Leishman, Giemsa, Wright): surrounding cytoplasm stains blue-purple while the Golgi zone stands out as a pale/white/clear crescent or oval.
Classic Example: Plasma Cell
The most well-known example is the plasma cell, where the perinuclear Golgi zone is a defining morphological feature.
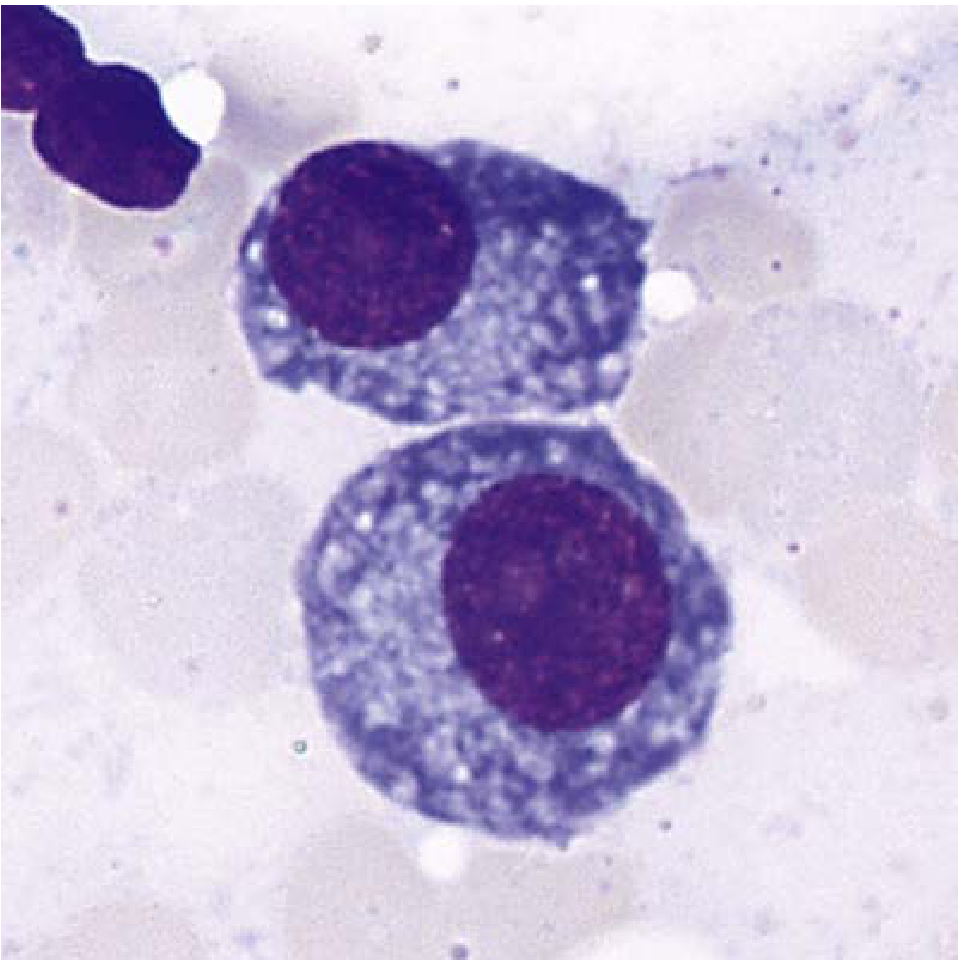
Plasma cells with abundant basophilic cytoplasm, eccentric nucleus, and perinuclear clear Golgi zone (Wright-Giemsa x1900). - Henry's Clinical Diagnosis and Management by Laboratory Methods
As described in the textbook: "Plasma cells have abundant blue cytoplasm, often with light streaks or vacuoles, an eccentric round nucleus, and a well-defined clear (Golgi) zone adjacent to the nucleus." - Henry's Clinical Diagnosis and Management by Laboratory Methods
The Golgi zone is prominent in plasma cells because they are high-output secretory cells - they produce massive amounts of immunoglobulin, so their Golgi apparatus is hypertrophied and very active.
Golgi Zone in Different Cell Types
| Cell Type | Golgi Zone Appearance | Significance |
|---|---|---|
| Plasma cell | Well-defined pale crescent directly touching the eccentric nucleus | Hallmark feature; hypertrophied due to active Ig secretion |
| Osteoblast | Large pale zone, but separated from the nucleus (not abutting it) | Distinguishes osteoblast from plasma cell |
| Myeloblast | Light unstained region in deep blue cytoplasm | Seen in early granulocyte precursors |
| ALCL hallmark cell | Prominent perinuclear eosinophilic region | The Golgi zone is more eosinophilic (pinkish) in ALCL, not pale |
| Promyelocyte | Golgi area often visible where cytoplasm is unstained | Present between the nucleus and azurophilic granules |
Golgi Zone in ALCL - Why It Differs
In Anaplastic Large Cell Lymphoma (ALCL), the perinuclear Golgi zone appears slightly differently. Rather than a clear/pale zone as in plasma cells, in ALCL it appears as a perinuclear eosinophilic (pinkish) region - this is because the Golgi in ALCL cells contains CD30 (Ki-1 antigen), which accumulates in the Golgi/endosomal compartment. On immunostaining for CD30, the Golgi zone stains intensely positive in a characteristic paranuclear dot-like pattern, which is one of the diagnostic clues for ALCL.
Summary
The perinuclear Golgi zone is the pale/clear cytoplasmic halo immediately adjacent to the nucleus, representing the physical location of the Golgi apparatus. It appears pale because the Golgi region lacks ribosomes (which provide basophilia). It is most prominently seen in plasma cells (classic "clock-face nucleus + perinuclear hof"), and is also a notable feature in ALCL hallmark cells and several other secretory cell types.
This is a shared conversation. Sign in to Orris to start your own chat.