Development of larynx and write on laryngeal web in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
laryngeal web congenital treatment endoscopic
Finding Sources
Reading Article
PMID: 36939597
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
DEVELOPMENT OF LARYNX AND LARYNGEAL WEB
(RGUHS University - 20 Mark Answer)
Sources: Cummings Otolaryngology, Scott-Brown's Otorhinolaryngology (Vol 1 & 2), K.J. Lee's Essential Otolaryngology, The Developing Human (Moore & Persaud - Clinically Oriented Embryology), Gray's Anatomy for Students + Recent PubMed Evidence
PART A: DEVELOPMENT OF LARYNX
I. EMBRYOLOGICAL TIMELINE AT A GLANCE
WEEK 4: Laryngotracheal groove forms in floor of primordial pharynx
↓
WEEK 4: LT diverticulum evaginates; lung bud appears
↓
WEEK 5: Tracheoesophageal septum divides foregut → LT tube (ventral) + esophagus (dorsal)
↓
WEEK 5-6: Arytenoid swellings appear → primordial glottis = T-shaped inlet
↓
WEEK 6-8: Epithelial proliferation → TEMPORARY OCCLUSION of laryngeal lumen
↓
WEEK 10: RECANALIZATION → laryngeal ventricles form → vocal folds + vestibular folds
↓
BIRTH: High larynx in neonate; descends over first 2 years of life
II. ORIGIN OF LARYNGEAL STRUCTURES
┌─────────────────────────────────────────────────────────────────────┐
│ SOURCES OF LARYNGEAL COMPONENTS │
├──────────────────────────────┬──────────────────────────────────────┤
│ Structure │ Embryological Origin │
├──────────────────────────────┼──────────────────────────────────────┤
│ Epithelial lining │ Endoderm of cranial LT tube │
│ Glands of larynx │ Endoderm │
│ Cartilages (thyroid, │ Mesenchyme from 4th & 6th │
│ cricoid, arytenoid, │ pharyngeal arches (neural crest │
│ cuneiform, corniculate) │ derived) │
│ Epiglottis │ Hypopharyngeal eminence │
│ │ (3rd + 4th arch ventral ends) │
│ Cricothyroid muscle │ 4th pharyngeal arch myoblasts │
│ All other intrinsic │ 6th pharyngeal arch myoblasts │
│ laryngeal muscles │ │
│ Connective tissue, │ Splanchnic mesoderm surrounding │
│ smooth muscle │ the foregut │
│ Vasculature │ Splanchnic mesenchyme │
└──────────────────────────────┴──────────────────────────────────────┘
Reference: - Cummings Otolaryngology Head and Neck Surgery, p. 3940
Reference: - The Developing Human - Clinically Oriented Embryology, p. 570
Reference: - Scott-Brown's Otorhinolaryngology, Vol 1, p. 927
III. STEP-BY-STEP DEVELOPMENT (DETAILED)
STEP 1 - Respiratory Primordium (Week 4)
The respiratory system begins as the laryngotracheal groove - a median outgrowth in the floor of the caudal anterior foregut (primordial pharynx), caudal to the 4th pair of pharyngeal pouches. The endodermal lining of this groove forms the pulmonary epithelium and glands of the larynx. Connective tissue, cartilage, and smooth muscle derive from the surrounding splanchnic mesoderm.
- The Developing Human, p. 565
STEP 2 - Laryngotracheal Diverticulum (End of Week 4)
The laryngotracheal groove evaginates to form a pouch-like laryngotracheal diverticulum ventral to the caudal foregut. Its distal end enlarges to form the lung bud (globular respiratory bud). The diverticulum maintains communication with the pharynx through the primordial laryngeal inlet.
STEP 3 - Tracheoesophageal Septum (Week 5)
Longitudinal tracheoesophageal folds develop in the diverticulum, approach each other, and fuse to form the tracheoesophageal septum, dividing the cranial foregut into:
- Ventral portion = laryngotracheal tube (larynx, trachea, bronchi, lungs)
- Dorsal portion = primordium of oropharynx and esophagus
Key signaling molecules involved: Nkx2.1, Shh, Wnt7b, Sox2, Bmp4, Fgf10 (mutations → esophageal atresia ± TEF)
- The Developing Human, p. 567-568
STEP 4 - Arytenoid Swellings (Weeks 5-6)
Mesenchyme at the cranial end of the laryngotracheal tube proliferates, producing paired arytenoid swellings (Fig. 10.4B). These swellings:
- Grow toward the tongue
- Convert the slit-like primordial glottis → T-shaped laryngeal inlet
- Reduce the developing laryngeal lumen to a narrow slit
- Elongate cranially, creating a cleft bounded laterally by aryepiglottic folds
STEP 5 - Temporary Occlusion (Weeks 6-10)
Laryngeal epithelium proliferates rapidly causing temporary occlusion of the laryngeal lumen. This is a normal developmental event, NOT a pathological process.
STEP 6 - Recanalization (Week 10)
Vacuolization and recanalization restores the lumen by the 10th week:
- Laryngeal ventricles form (recesses of mucous membrane)
- True vocal folds (cords) emerge as folds of mucous membrane
- Vestibular folds (false cords) form similarly
- Cummings Otolaryngology, p. 3940; The Developing Human, p. 570
Epiglottis Development
The epiglottis develops from the caudal part of the hypopharyngeal eminence, produced by mesenchyme in the ventral ends of the 3rd and 4th pharyngeal arches. The rostral part of this eminence forms the posterior one-third of the tongue.
STEP 7 - Innervation
- 4th arch (cricothyroid) → Superior laryngeal nerve (SLN) (branch of CN X)
- 6th arch (all other intrinsic muscles) → Recurrent laryngeal nerve (RLN) (branch of CN X)
Position of Larynx
The neonatal larynx occupies a HIGH position in the neck - the epiglottis contacts the soft palate, providing near-separate respiratory and digestive tracts, obligatory nasal breathing in neonates. Structural descent of the larynx occurs over the first 2 years of life.
- The Developing Human, p. 571
IV. DIAGRAM - DEVELOPMENT OF LARYNX (Successive stages)
(From Moore & Persaud - The Developing Human, Fig 10.4)
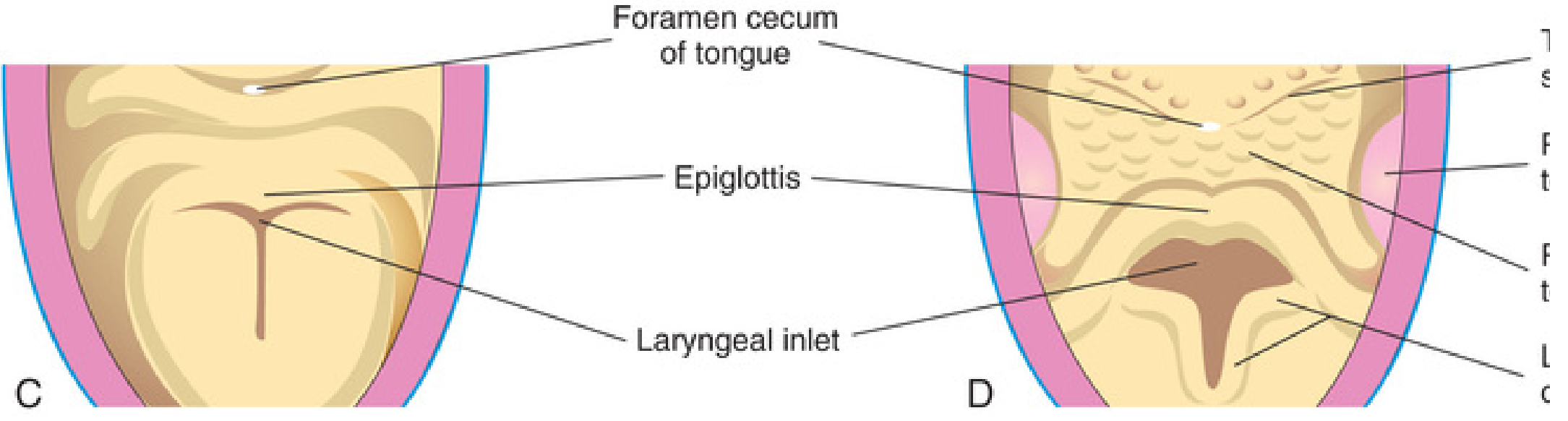
Fig. 10.4 (C & D): Successive stages in the development of the larynx. Note the laryngeal inlet changes from a slit-like opening to a T-shaped inlet as mesenchyme proliferates. The epiglottis is formed from the hypopharyngeal eminence. - The Developing Human, Clinically Oriented Embryology
PART B: LARYNGEAL WEB (DETAILED - 20 Marks)
I. DEFINITION
A laryngeal web is a congenital or acquired membrane/band of fibrous tissue stretching across the laryngeal lumen, most commonly at the anterior glottis, fusing the vocal cords over a variable portion of their length and causing variable degrees of respiratory obstruction and dysphonia.
- Scott-Brown's Vol 2, p. 523
- Cummings Otolaryngology, p. 3895
- K.J. Lee's Essential Otolaryngology, p. 939
II. CLASSIFICATION
A. Based on Etiology:
| Type | Etiology |
|---|---|
| Congenital | Failure of recanalization of larynx during 10th week |
| Acquired | Post-intubation, trauma, laryngeal surgery, inflammation, irradiation |
B. Based on Location:
| Location | Features |
|---|---|
| Anterior (most common, ~75%) | Anterior commissure; fuses anterior vocal cords |
| Posterior | Interarytenoid; may be associated with cricoarytenoid joint fixation |
| Supraglottic | Very rare; aryepiglottic folds involved |
C. Cohen's Classification of Glottic Webs (MOST IMPORTANT - Cummings Table 206.4):
┌────────┬────────────────────────┬──────────────────────────────────┬─────────────────────────────────┐
│ Grade │ Glottic Obstruction │ Subglottic Involvement │ Symptoms │
├────────┼────────────────────────┼──────────────────────────────────┼─────────────────────────────────┤
│ Type 1 │ < 35% │ None or little │ Mild hoarseness only │
│ Type 2 │ 35% – 50% │ Thin anterior web, little │ Hoarse/weak cry, stridor on │
│ │ │ subglottic extension │ exertion │
│ Type 3 │ 50% – 75% │ Thin-thick web, extends to │ Severe hoarseness, moderate │
│ │ │ lower border of cricoid │ airway obstruction │
│ Type 4 │ > 75% │ Thick web to below cricoid; │ Aphonia, severe obstruction │
│ │ │ subglottic "sail" configuration │ Neonatal emergency │
└────────┴────────────────────────┴──────────────────────────────────┴─────────────────────────────────┘
Reference: Cohen SR - Congenital glottic webs in children. Ann Otol Rhinol Laryngol Suppl, 1985, cited in Cummings
III. EMBRYOLOGICAL BASIS (PATHOGENESIS)
FLOWCHART: PATHOGENESIS OF CONGENITAL LARYNGEAL WEB
Normal Development:
Laryngeal lumen occluded (Wk 6-8)
↓
Vacuolization & Recanalization (Wk 10)
↓
Complete recanalization → NORMAL LARYNX
Abnormal Development:
FAILURE / INCOMPLETE RECANALIZATION (Week 10)
↓
├──► Partial failure → LARYNGEAL WEB (connective tissue
│ covered with mucous membrane)
└──► Complete failure → LARYNGEAL ATRESIA (CHAOS Syndrome)
The Developing Human: "Incomplete atresia, or laryngeal web, is a defect in which the connective tissue between the vocal folds is covered with a mucous membrane; this causes airway obstruction and a hoarse cry in the neonate. This defect results from incomplete recanalization of the larynx during the 10th week." - p. 572
Glottic webs exist on a spectrum of embryologic severity ultimately in continuity with complete laryngeal atresia. - Cummings, p. 3895
IV. INCIDENCE AND ASSOCIATIONS
- Rare - estimated 1:10,000 - 1:70,000 live births (Dhingra; Hazarika)
- More common in males
- 22q11.2 deletion syndrome is the most important association:
- In one series of 17 patients with anterior glottic webs, 11 (65%) had chromosome 22q11.2 deletions (Cummings, p. 3895)
- Phenotypes include: DiGeorge syndrome, Velocardiofacial (Shprintzen) syndrome, conotruncal heart malformations
- Richieri-Costa Pereira syndrome: laryngeal anomalies including microwebs, hypoplasia of epiglottis
- Cardiac anomalies are frequently associated - all patients require thorough cardiovascular evaluation including aortic arch assessment (vascular ring may mimic laryngeal web symptoms)
- Associated chromosomal and cardiac anomalies reported by multiple authors (Stell & Maran)
V. CLINICAL FEATURES
FLOWCHART: CLINICAL PRESENTATION BASED ON GRADE
LARYNGEAL WEB
│
┌──────────────┼──────────────┐
▼ ▼ ▼
GRADE I GRADE II GRADE III/IV
│ │ │
Mild hoarse Weak/hoarse Severe airway
voice only cry, exertional obstruction +
May be stridor aphonia +
incidental neonatal
finding emergency
Key clinical features (Scott-Brown, Cummings, Dhingra, Hazarika):
- Weak, hoarse cry from birth - pathognomonic
- Inspiratory stridor - characteristically high-pitched
- Squeaky, high-pitched voice - characteristic
- Respiratory distress - degree depends on grade
- Aphonia - in severe types (Grade IV)
- Recurrent croup in infancy - combination of weak cry from birth + recurrent croup should always raise suspicion (Scott-Brown, p. 536)
- Thin webs may be lysed unrecognized during intubation
"The combination of a weak cry from birth and recurrent croup in infancy should always raise suspicion of a laryngeal web" - Scott-Brown's Otorhinolaryngology Vol 2
VI. DIAGNOSIS
DIAGNOSTIC ALGORITHM FOR SUSPECTED LARYNGEAL WEB
Neonate/Child with:
Weak cry + Stridor + Hoarse voice
│
▼
AWAKE FLEXIBLE NASOPHARYNGOSCOPY (First investigation)
│
┌─────┴──────┐
│ │
Web seen Inconclusive
│ │
▼ ▼
MICROLARYNGOSCOPY CT Neck/Chest
& BRONCHOSCOPY (assess subglottic
(Gold standard) extent, vascular ring)
│
├── Confirm grade (Cohen classification)
├── Assess subglottic extension
├── Assess associated lesions
└── Thickness of web (thin vs cartilaginous)
│
▼
GENETIC SCREENING (22q11.2 FISH/microarray)
ECHOCARDIOGRAPHY (cardiovascular anomalies)
Endoscopic findings:
- Anterior grayish-white membrane across the anterior glottis
- Thin posteriorly near free edge, thicker anteriorly
- "Sail" configuration of subglottis in Grade 3/4 (Cummings)
- Grade determines extent and need for open vs. endoscopic surgery
Endoscopic image (Cummings, Fig 206.4 - Anterior glottic web):

Fig. 206.4 Anterior glottic web - Cummings Otolaryngology Head and Neck Surgery
Endoscopic image (Scott-Brown Vol 2, Fig 30.3 - Anterior glottic web):
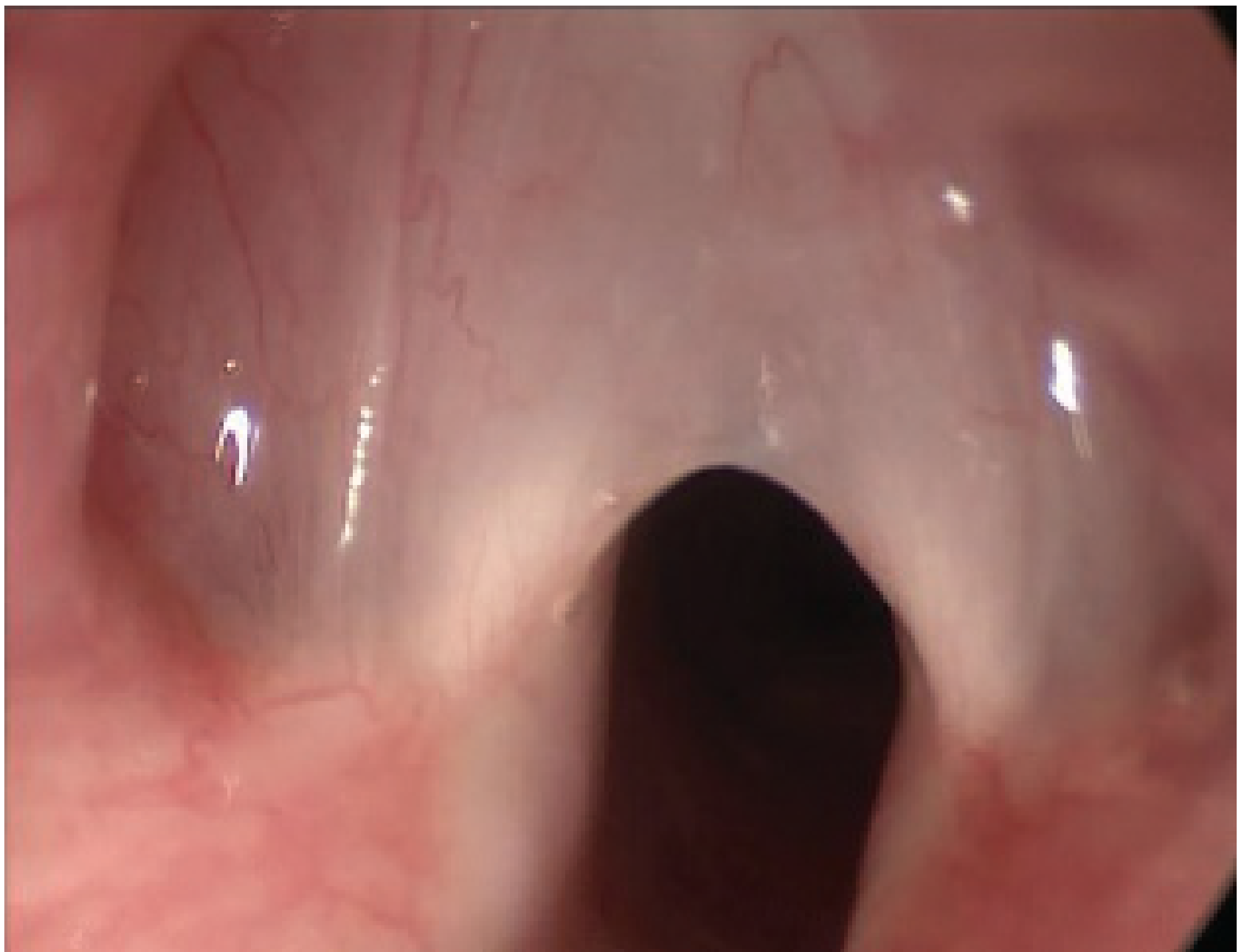
Figure 30.3 - Anterior glottic web - Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2
VII. TREATMENT
TREATMENT FLOWCHART FOR LARYNGEAL WEB
LARYNGEAL WEB DIAGNOSED
│
┌──────────┴───────────┐
│ │
GRADE I/II GRADE III/IV
(< 50% obstruction) (> 50% obstruction)
│ │
▼ ▼
Small, thin, asymptomatic? TRACHEOSTOMY first
│ (to secure airway)
┌──────┤ │
│ │ ▼
Yes No LARYNGOTRACHEAL RECONSTRUCTION (LTR)
│ │ - Anterior cartilage graft
▼ ▼ - Laryngofissure + stent/keel
CONSERVATIVE ENDOSCOPIC or
(observe) APPROACH: OPEN APPROACH:
- Cold knife - Thyrotomy + keel
division placement (Montgomery
- CO2 laser keel)
division - LTR with cartilage
- Keel grafting
placement - Cricotracheal resection
(endoscopic) (in selected cases)
Detailed treatment options:
1. Conservative (Grade I, minimal symptoms)
- No intervention needed for very small, asymptomatic webs
- Regular follow-up
2. Endoscopic Lysis (Grade I and selected Grade II)
- Division with cold knife or CO2 laser along margin of one vocal cord
- Keel placement endoscopically after division to prevent re-web formation
- If web is very thin: subsequent endoscopic dilation may be sufficient
- In young children with small larynx: covering tracheostomy is required for 2 weeks while keel is in place
- Scott-Brown's Vol 2, p. 550-564
3. Open Surgery (Grade III and IV)
- Laryngotracheal reconstruction (LTR) with anterior cartilage grafting
- Can be done as single-stage (infant, post-op ETT stenting 5-7 days) or double-stage (tracheostomy first, LTR at 1-2 years when larynx is larger)
- Laryngofissure with keel (Montgomery keel) placement
- Voice outcomes after repair are often less favorable, particularly with multiple/revision procedures
- Cummings, p. 3895-3896
4. EXIT Procedure (Grade IV, Laryngeal Atresia/CHAOS)
- Ex utero intrapartum treatment (EXIT): airway secured before delivery is complete
- Prenatal diagnosis via fetal MRI (enlarged echogenic lungs, inverted diaphragms, massive ascites, dilated airways)
- Cummings, p. 3896
VIII. SPECIAL ENTITY: LARYNGEAL ATRESIA AND CHAOS SYNDROME
CHAOS SYNDROME (Congenital High Airway Obstruction Syndrome)
│
Complete failure of recanalization
│
┌─────────┼─────────────┐
▼ ▼ ▼
Laryngeal Subglottic Tracheal
atresia atresia atresia
│
▼
PRENATAL FEATURES (on USS/MRI):
- Enlarged echogenic lungs
- Inverted diaphragm
- Dilated airways distal to obstruction
- Fetal ascites/hydrops
│
▼
POSTNATAL: Aphonia + extreme respiratory
distress + cyanosis at birth
│
▼
MANAGEMENT: EXIT procedure (ex utero
intrapartum treatment) + tracheostomy
Cummings Otolaryngology, p. 3940; The Developing Human, p. 572
IX. ACQUIRED LARYNGEAL WEB
Causes (Hazarika, Dhingra, Stell & Maran):
- Post-intubation trauma (commonest acquired cause)
- Post-surgical (after laryngeal procedures, irradiation)
- Inflammatory (diphtheria, syphilis, lupus)
- Post-laryngeal injury
Pathology: Bilateral raw areas on opposing mucosa heal by fusion → cicatricial web usually at anterior commissure.
Treatment: Same principles as congenital - endoscopic lysis + keel/stent or open LTR for thick webs.
X. RECENT ADVANCES (2021-2026)
Key Systematic Review (PMID: 36939597 | Moore AE et al., 2023, Otolaryngol Head Neck Surg):
A systematic review and meta-analysis of 24 articles (126 patients) comparing endoscopic vs. open approaches:
| Outcome | Grade I/II | Grade III/IV |
|---|---|---|
| Tracheostomy avoidance/decannulation | Endoscopic = Open (100% both) | Open 96% vs Endoscopic 84% (p=0.081) |
| Revision surgery rate | No difference | Open 30.9% vs Endoscopic 77.8% (p=0.008) |
Conclusion: For Grades I and II - no difference between approaches. For Grades III and IV - open surgery achieves significantly lower revision rates, but with higher morbidity. Open surgery should be preferred for higher-grade webs.
Other recent advances:
- Prenatal diagnosis - fetal MRI for CHAOS/laryngeal atresia with EXIT procedure planning improving survival
- Genetic testing - routine 22q11.2 microarray in all congenital laryngeal webs
- KTP and CO2 laser techniques - office-based angiolytic laser (KTP 532nm) for thinner webs
- Balloon dilation - as adjunct after endoscopic lysis
- Mitomycin C application post-lysis to reduce re-web formation (some centers)
- 3D endoscopic imaging and narrow-band imaging for better characterization
- Tissue-engineered scaffolds - experimental, for LTR grafts
XI. PROGNOSIS
- Voice outcomes are often suboptimal even after successful airway reconstruction
- Grade I/II: Good prognosis for both airway and voice
- Grade III/IV: Airway patency is achievable; voice may remain permanently impaired
- Multiple/revision procedures worsen voice outcome
- Associated 22q11.2 deletion may affect overall prognosis due to cardiac/immune issues
SUMMARY TABLE (Quick Revision for RGUHS)
| Aspect | Key Point |
|---|---|
| Embryological origin | Failure of recanalization at week 10 |
| Most common type | Anterior glottic (congenital) |
| Classification | Cohen Grade I-IV |
| Pathognomonic feature | Weak cry from birth + hoarse voice |
| Key investigation | Microlaryngoscopy + bronchoscopy |
| Important association | 22q11.2 deletion (65% cases) |
| Grade I/II treatment | Endoscopic lysis ± keel |
| Grade III/IV treatment | Open LTR with anterior cartilage graft |
| Most severe form | Laryngeal atresia → CHAOS syndrome |
| Recent evidence | Endoscopic = Open for Grade I/II; Open better for Grade III/IV (Moore et al., 2023) |
REFERENCES FOR RGUHS ANSWER
- Cummings Otolaryngology Head and Neck Surgery - Chapter 206 (Congenital Laryngeal Anomalies) & Chapter 209 (Laryngeal Stenosis)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2 - Chapter 30 (Paediatric Laryngeal Conditions)
- K.J. Lee's Essential Otolaryngology - Chapter: Developmental Anatomy / Laryngeal Web or Atresia
- The Developing Human - Clinically Oriented Embryology (Moore & Persaud) - Chapter 10: Respiratory System (Development of Larynx, pp. 570-572)
- Dhingra PL - Diseases of Ear, Nose and Throat - Chapter on Congenital Laryngeal Anomalies
- Hazarika P - Textbook of Ear Nose Throat & Head Neck Surgery - Chapter on Larynx
- Stell & Maran's Head and Neck Surgery - Relevant chapter on Laryngeal Anomalies
- Cohen SR - Congenital glottic webs in children: a retrospective review of 51 patients. Ann Otol Rhinol Laryngol Suppl 121:2-16, 1985 (ORIGINAL CLASSIFICATION)
- Moore AE, Walker A, Kanotra SP - Endoscopic Versus Open Surgical Intervention for Congenital Laryngeal Webs: A Systematic Review and Meta-Analysis. Otolaryngol Head Neck Surg 2023 Aug; PMID: 36939597 (Level 1 Evidence)
RGUHS Exam Tip: For a 20-mark question, structure your answer as: (1) Development of Larynx with flowchart of stages (6 marks), (2) Definition + Classification of Laryngeal Web with Cohen table (4 marks), (3) Etiology + Pathogenesis flowchart (2 marks), (4) Clinical features + Diagnosis flowchart (4 marks), (5) Treatment flowchart with management algorithm (4 marks). Always mention 22q11.2 association, Cohen classification, and EXIT procedure for full marks.
This is a shared conversation. Sign in to Orris to start your own chat.