Explain DDH
Reading File
Finding Sources
Finding Sources
Searching PubMed
"developmental dysplasia of the hip"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
developmental dysplasia of the hip DDH Barlow Ortolani Pavlik harness
Reading File
I now have comprehensive content. Let me compile a thorough answer.
Developmental Dysplasia of the Hip (DDH)
Definition & Spectrum
DDH describes abnormal development or dislocation of the hip secondary to capsular laxity and mechanical factors. It is a spectrum, not a single entity:
| Grade | Description |
|---|---|
| Dysplasia | Shallow acetabulum with normal femoral head position |
| Subluxation | Partial loss of contact between femoral head and acetabulum |
| Dislocation | Complete loss of contact |
| Teratologic | Dislocated in utero, irreducible at birth; associated with neuromuscular conditions (arthrogryposis, Larsen syndrome) |
| Late dysplasia | Presents in adolescence/adulthood |
- Miller's Review of Orthopaedics, 9th ed.
Epidemiology & Risk Factors
Risk factors in order of importance:
- Breech positioning (30–50% of DDH cases)
- Positive family history / ligamentous laxity (≥20%)
- Female sex (~85% of cases)
- Firstborn child (less intrauterine space)
- Increased maternal estrogens
- Left hip most commonly affected (67% of cases)
Also associated with: postnatal swaddling with hips in extension, torticollis (20%), metatarsus adductus (10%). No association with clubfoot.
A 2025 meta-analysis (PMID 39853978) confirmed breech presentation as the single strongest risk factor for DDH before 3 months of age.
Pathophysiology
If untreated:
- Muscles around the hip become contracted
- The acetabulum becomes progressively dysplastic
- The acetabular cavity fills with fibrofatty tissue (pulvinar)
Obstacles to concentric reduction (important surgically — see illustration):
- Iliopsoas tendon
- Pulvinar
- Hypertrophied ligamentum teres
- Contracted inferomedial hip capsule
- Transverse acetabular ligament
- Inverted labrum
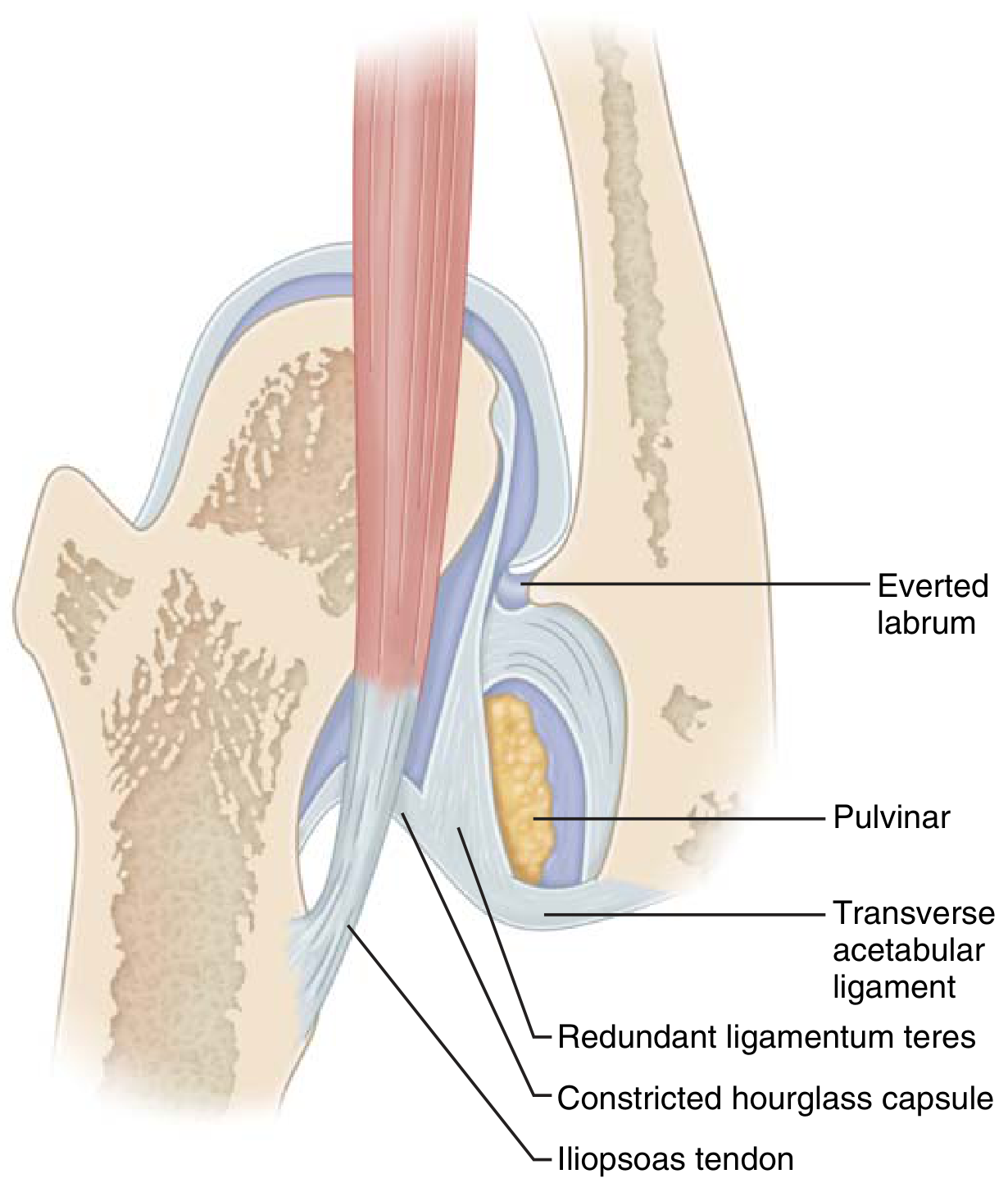
Blocks to reduction in DDH: iliopsoas tendon, pulvinar, transverse acetabular ligament (Miller's Review of Orthopaedics)
Clinical Diagnosis
Neonatal Screening Tests (most useful <3 months)
| Test | Technique | Positive Finding |
|---|---|---|
| Ortolani | Elevate + abduct the flexed hip | Palpable clunk as dislocated head reduces back into acetabulum |
| Barlow | Adduct + depress the flexed hip | Palpable clunk as reduced head dislocates |
- Ortolani-positive = dislocated but reducible
- Barlow-positive = reduced but dislocatable
Caution: bilateral dislocations may show symmetric abduction limitation, masking the finding.
Signs in Older Infants (>3 months)
- Limited hip abduction (most reliable sign as laxity resolves)
- Galeazzi sign: feet held together, knees flexed — apparent femoral shortening on the affected side
- Trendelenburg gait (older children)
- Asymmetric gluteal folds (less reliable)
- Increased lumbar lordosis, pelvic obliquity

Imaging
| Age | Modality | Notes |
|---|---|---|
| < 4–6 months | Ultrasound (dynamic) | Gold standard — bones not yet ossified; uses Graf angle classification |
| > 4–6 months | Plain X-ray (AP pelvis) | Femoral head ossifies; assess Hilgenreiner's line, Perkin's line, acetabular index, Shenton's line |
Graf classification on ultrasound:
- Type I: Normal (α angle >60°)
- Type IIa: Physiologically immature (<3 months)
- Type IIb: Delayed ossification (>3 months)
- Type IIc/D: Critical zone — at risk for dislocation
- Type III/IV: Dislocated
Selective ultrasound screening is recommended for high-risk infants (breech, family history).

Treatment — Age-Based Algorithm
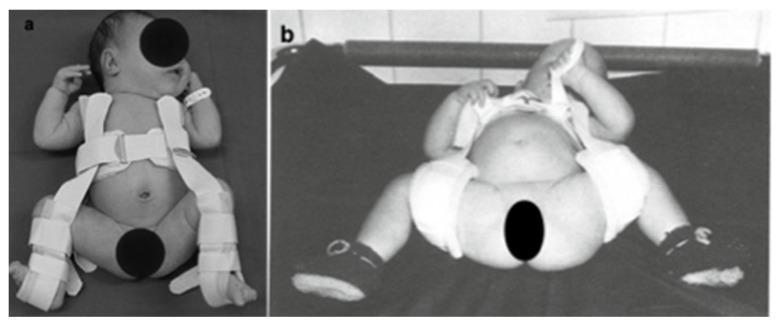
0–6 Months: Pavlik Harness
- First-line treatment
- Maintains hips in ~100° flexion and mild abduction (the "human position")
- Worn 23 hours/day until exam and ultrasound normalize
- Hip must stay within the safe zone of Ramsey (between maximum adduction before redislocation and excessive abduction causing AVN)
- "Pavlik disease": if reduction not achieved in 3 weeks, discontinue → risk of erosion above acetabulum making future reduction harder
- Contraindications: teratologic dislocation; narrow safe zone (<40°, consider adductor tenotomy)
- Complications: femoral nerve palsy (excessive flexion), avascular necrosis (excessive abduction)
6–18 Months: Closed Reduction + Spica Cast
- Hip arthrography + percutaneous adductor tenotomy + closed reduction + spica cast
- Post-reduction CT or MRI confirms concentric reduction
- If closed reduction fails → open reduction
18 Months–3 Years: Open Reduction
- Open reduction with femoral shortening osteotomy ± acetabular osteotomy (capsulorrhaphy)
3–8 Years: Acetabular Osteotomy
- Salter, Dega, Pemberton, or Staheli procedure
>8 Years: Osteotomy (growth-plate status dependent)
- Growth plate open: triple (Steele), double pelvic (Southerland), or Staheli
- Growth plate closed: Ganz or Chiari procedures
Adults: Total Hip Arthroplasty (THA)
Complications
- Avascular necrosis (AVN) / osteonecrosis of the femoral head — most dreaded complication of both disease and treatment
- Degenerative joint disease if untreated
- Re-dislocation
- Femoral nerve palsy (Pavlik harness)
- Persistent acetabular dysplasia requiring further surgery
Key Points Summary
| Feature | Detail |
|---|---|
| Commonest form | Left hip, female, firstborn, breech |
| Neonatal test | Ortolani (reduce) / Barlow (dislocate) |
| Best imaging <6 mo | Ultrasound (Graf classification) |
| Best imaging >6 mo | AP pelvis X-ray |
| Treatment <6 mo | Pavlik harness |
| Worst complication | AVN of femoral head |
| Untreated adult sequela | Severe OA requiring THA |
Sources: Schwartz's Principles of Surgery, 11th ed.; Miller's Review of Orthopaedics, 9th ed.; recent evidence from PMID 39853978 (meta-analysis, JAMA Network Open 2025).
This is a shared conversation. Sign in to Orris to start your own chat.