Everything about tracheostomy procedure in detail
Reading File
Finding Sources
Searching the Web
tracheostomy procedure surgical technique indications complications 2024
Searching PubMed
tracheostomy procedure complications management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative surgical textbooks. Let me compile a thorough, well-organized answer.
Tracheostomy: A Comprehensive Overview
Tracheostomy is the surgical creation of an opening (stoma) in the anterior cervical trachea through which a tracheostomy tube is placed to establish a direct, stable airway. It is the most common surgical procedure in critically ill patients requiring prolonged mechanical ventilation.
1. History
- First open tracheostomy recorded over 3,500 years ago (ancient Egyptian stone slabs)
- Fabricius described the first tracheal cannula in 1617
- Sanctorio Sanctorius documented the first percutaneous approach in 1626
- The first cuffed tube was developed by Trendelenburg in 1869
- Chevalier Jackson standardized open surgical tracheostomy in the early 20th century
- Pasquale Ciaglia described modern percutaneous dilatational tracheostomy (PDT) in 1985
2. Relevant Anatomy
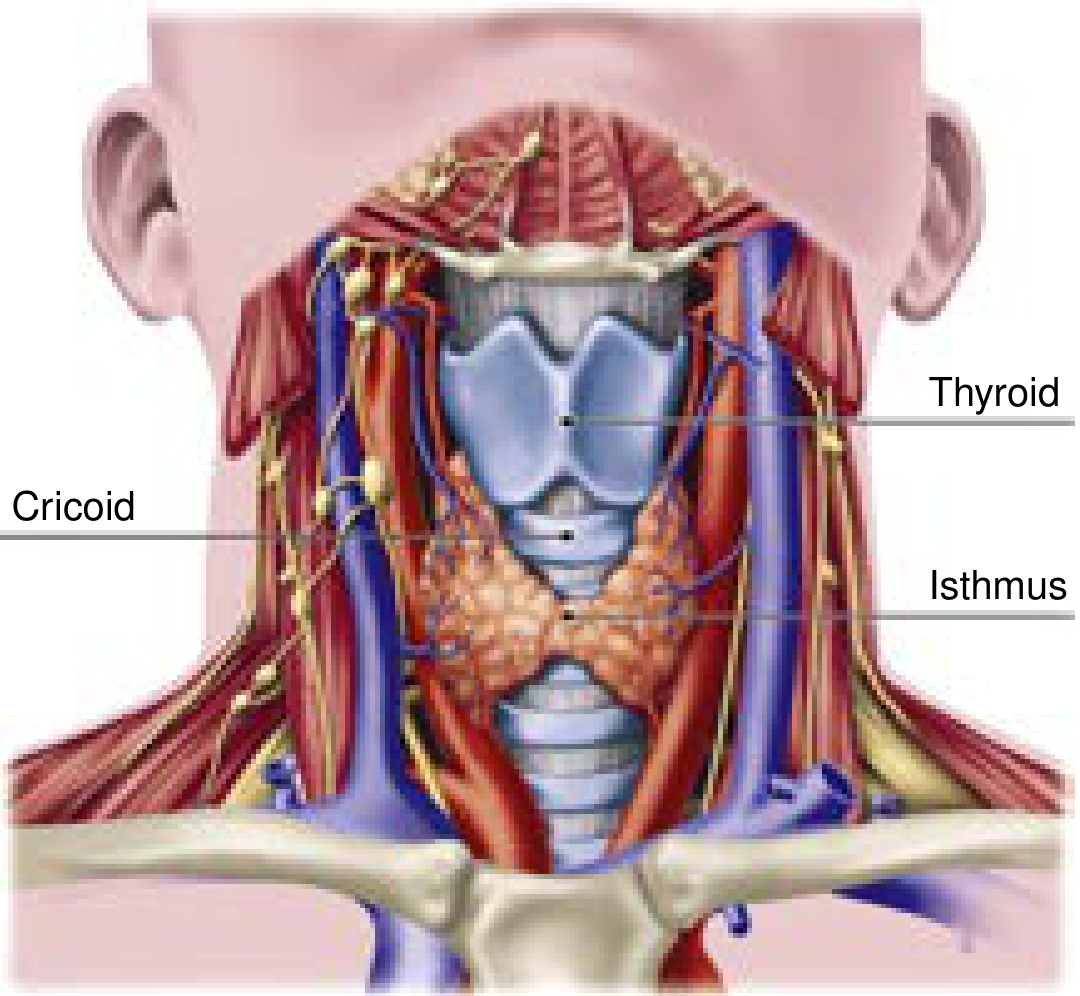
Tracheal anatomy - note thyroid cartilage, cricoid, and thyroid isthmus (Current Surgical Therapy 14e, Fig. 1)
Key anatomical points:
- The trachea extends obliquely from the superficial neck posteriorly into the mediastinum - average adult length 11 ± 1 cm (male) and 10 ± 1 cm (female)
- 18-22 incomplete semicircular cartilaginous rings maintain structural integrity; only the cricoid is a complete ring
- Tracheal diameter: 2.5-2.7 cm (men), 2.1-2.3 cm (women) - important for tube sizing
- The thyroid isthmus typically sits between the 2nd and 3rd tracheal rings - must be identified and managed
- The innominate artery crosses the anterior trachea obliquely distal to the 3rd ring near the sternal notch - violation causes catastrophic hemorrhage
- The inferior thyroid artery/vein and anterior jugular veins lie between skin and trachea
- The posterior tracheal wall (membranous trachea) - fibroelastic tissue abutting the esophagus anterolaterally - is vulnerable to perforation
- Current Surgical Therapy 14e, pp. 1591-1592
3. Indications
| Category | Examples |
|---|---|
| Upper airway obstruction | Head/neck malignancy, significant maxillofacial trauma, angioedema, subglottic/tracheal stenosis, radiation stricture, burns, obstructive sleep apnea |
| Prolonged mechanical ventilation | Chronic hypoxic/hypercapnic respiratory failure; cardiac or systemic causes |
| Neurologic conditions | Brain injury (acute or progressive), spinal cord injury, severe agitation/delirium, prolonged altered mental status |
| Pulmonary toilet | Chronic secretion management, neuromuscular disease |
| Emergency/failed airway | When orotracheal intubation fails - adjunct to or instead of cricothyrotomy |
- Sabiston Textbook of Surgery, Table 47.1
4. Contraindications
All contraindications are relative:
- Recent anterior neck surgery (<7 days)
- High ventilator settings: FiO₂ >50%, PEEP >10 cmH₂O, advanced ventilator modes
- Elevated intracranial pressure
- Hemodynamic instability
- Significant coagulopathy or bleeding risk
- Local infection or malignancy at the proposed site
- Predicted early mortality (procedure would not benefit patient)
5. Benefits of Tracheostomy Over Translaryngeal Intubation
- Reduced sedation needs (no glottic stimulation)
- Reduced airway dead space
- Reduced tube resistance and work of breathing
- Improved mouth care and oral hygiene
- Ongoing bronchopulmonary toilet during weaning
- Allows speech (with speaking valve or cuff deflation)
- Greater patient comfort and mobility
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1
6. Timing
This remains controversial. Key data:
- Early (≤4-7 days): some studies show reduction in ICU stay, ventilator days, and VAP, with one RCT showing significant mortality reduction (32% vs 62%) when tracheostomy at 48h vs. 14-16 days in patients predicted to need >2 weeks ventilation
- Late (>10 days): the largest RCT (TracMan, >900 UK patients) showed no mortality difference between early (within 4 days) vs. late (after 10 days); importantly, >50% of the late group never needed tracheostomy at all
- Current practice: individualized decision based on daily weaning attempts, predicted trajectory, and procedure risk
- For COVID-19 patients: data suggests tracheostomy after 10-14 days of ventilation is associated with lower ventilator duration without increased mortality
7. Tracheostomy Techniques
A. Surgical (Open) Tracheostomy
Setting: Operating room or ICU bedside (with full equipment, lighting, electrocautery)
Anesthesia: General anesthesia (rarely conscious sedation in a spontaneously breathing patient)
Step-by-step technique:
- Positioning: Patient supine, neck moderately extended with a shoulder roll; head of bed slightly elevated to reduce cervical venous pressure
- Landmark identification: Palpate thyroid cartilage, cricothyroid membrane, cricoid cartilage, tracheal rings
- Prep and drape: Sterile fashion from nipple line to above thyroid cartilage
- Skin incision: Transverse incision, 3-4 cm, placed 1 cm below the cricoid cartilage (not based on sternal notch, as the trachea and larynx move independently of the sternum)
- Soft tissue dissection: Subcutaneous tissue and platysma divided with electrocautery; sternohyoid and sternothyroid muscles retracted laterally
- Thyroid isthmus: Identified deep to strap muscles; can be retracted superiorly or ligated with sutures/electrocautery and divided
- Tracheal exposure: Tracheal rings exposed; often a stay suture (0 PDS) is placed on either side of the planned tracheal incision - these serve as traction sutures if accidental decannulation occurs
- Tracheal entry: Incision made between 2nd and 3rd tracheal rings; a Bjork flap (inferiorly based tracheal flap) may be created and sutured to the skin to facilitate recannulation
- Tube insertion: After the anesthesiologist partially withdraws the ETT above the planned tracheal entry site, the tracheostomy tube (loaded on its obturator) is inserted under direct vision with the cuff distal to the incision
- Cuff inflation and verification: Cuff inflated; ventilation confirmed via capnography and bilateral auscultation; ETT removed
- Securing: Tube secured with tracheostomy collar/tie (allow one finger between strap and skin); neck plate sutured or stapled to skin; one operator must always hold the tube while securing
- Current Surgical Therapy 14e, pp. 1592-1593
B. Percutaneous Dilatational Tracheostomy (PDT) - Ciaglia Technique
The most widely used elective tracheostomy technique in the ICU. Performed by critical care or surgical teams, usually under bronchoscopic guidance.
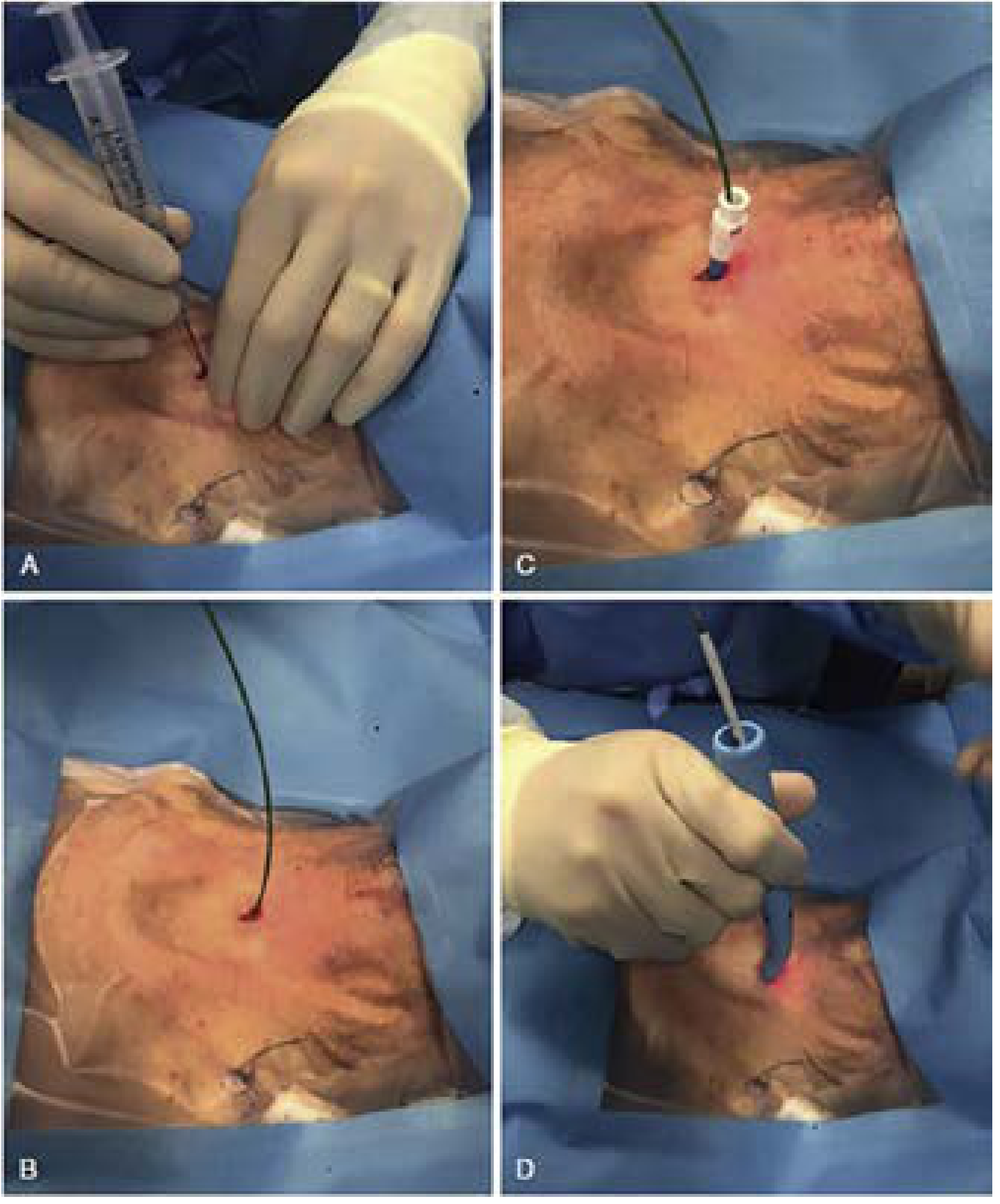
PDT technique steps - introducer needle, guidewire placement, serial dilation (Current Surgical Therapy 14e, Fig. 5)
Pre-procedure checks:
- PEEP should be <12 cmH₂O; increase FiO₂ as needed to maintain oxygenation
- Verify coagulation status; ensure anatomy can be palpated
- Set up bronchoscope (confirms midline needle entry into trachea)
Step-by-step PDT:
- Positioning and prep: Same as open technique - neck extended, shoulder roll, sterile prep
- ETT withdrawal: Anesthesiologist partially withdraws the ETT under bronchoscopic visualization to a position just below the cords, ensuring the cuff remains at the level of the stoma during dilation
- Local anesthesia and skin incision: Local anesthetic injected; a 1-2 cm transverse skin incision is made over the 2nd-3rd tracheal interspace
- Needle puncture: An introducer needle (with saline-filled syringe) is inserted in the midline between the 2nd and 3rd rings; air aspiration and bronchoscopic visualization confirm intratracheal position
- Guidewire placement: A Seldinger guidewire is passed through the needle into the tracheal lumen and advanced distally (confirmed bronchoscopically)
- Serial dilation: A 4 Fr dilator is passed over the wire to start the tract, followed by graduated Ciaglia dilators (single tapered dilator technique preferred now) to expand the stoma to appropriate size
- Tube insertion: Tracheostomy tube loaded on its obturator is threaded over the wire and advanced into the trachea; obturator and wire removed simultaneously
- Verification: Cuff inflated, ventilation confirmed via capnography and auscultation; bronchoscopy confirms position above the carina
- Securing: Identical to open technique
Alternative PDT variants:
- Griggs forceps technique: Uses a Howard-Kelly clamp over the wire
- PercuTwist: Single-step rotational dilator
- Ciaglia Blue Rhino: Single, curved tapered dilator (most widely used today)
8. Tracheostomy Tube Components and Types
A standard tracheostomy tube has three components:
- Outer cannula: The main body, held in place by flanges and securing ties
- Inner cannula: Removable for cleaning; critical for preventing tube obstruction from secretions
- Obturator: Used only for insertion; replaced immediately with the inner cannula after placement
Types of tubes:
| Type | Feature | Indication |
|---|---|---|
| Cuffed | Inflatable cuff seals airway | Positive pressure ventilation, aspiration risk |
| Uncuffed | No cuff | Weaning, long-term airway management in spontaneously breathing patients |
| Fenestrated | Hole in outer cannula | Allows airflow through vocal cords for speech; used in weaning |
| Speaking valve (Passy-Muir) | One-way valve - in on trach, out through larynx | Voicing with a tracheostomy |
| Adjustable flange (extra-long) | Adjustable neck plate depth | Obese patients or unusual anatomy |
| Subglottic suctioning port | Above-cuff suction lumen | Reduces VAP in ventilated patients |
| Reinforced (armored) | Flexible wire-reinforced | Head/neck surgery, unusual neck anatomy |
Tube sizing (Jackson size conversion):
| Jackson Size | Inner Diameter with Inner Cannula (mm) | Outer Diameter (mm) |
|---|---|---|
| 4 | 5.0 | 9.4 |
| 6 | 6.4 | 10.8 |
| 8 | 7.6 | 12.2 |
| 10 | 8.9 | 13.8 |
- Sabiston Textbook of Surgery, Table 47.2
9. PDT vs. Open Surgical Tracheostomy - Comparison
| Feature | PDT | Open Surgical |
|---|---|---|
| Setting | Bedside ICU | OR or bedside |
| Anesthesia | Sedation + NMB | General or local |
| Speed | Faster | Slower |
| Cost | Lower | Higher |
| Wound infection | Less frequent | More frequent |
| Posterior wall injury | Slightly higher (~50/10,000) | Rare (~6/10,000) |
| Tracheal ring fracture | More common | Very rare (direct vision) |
| Serious perioperative complications | Comparable | Comparable |
| Periprocedural mortality | <0.2% | Comparable |
| Preferred when | Standard ICU patient | Obesity, coagulopathy, abnormal anatomy, difficult neck |
Meta-analyses generally show equivalence in overall complication rates, with PDT having fewer wound infections and comparable bleeding rates. PDT is preferred in most elective ICU settings.
- Current Surgical Therapy 14e, pp. 1594-1596; Scott-Brown's Otorhinolaryngology, Vol. 1
10. Complications
Early/Perioperative Complications
| Complication | Notes |
|---|---|
| Hemorrhage | Most common early complication; usually from anterior jugular veins or thyroid isthmus. Managed by tightening collar, hemostatic agents (Surgicel, QuikClot), or local epinephrine injection |
| Accidental decannulation | Reinsertion through immature stoma can create a false tract - reintubate orally first, then replace tracheostomy under controlled circumstances |
| Posterior tracheal wall injury | Perforation of membranous trachea; risk of tracheoesophageal fistula |
| Paratracheal insertion | Tube placed outside tracheal lumen; confirmed by bronchoscopy |
| Pneumothorax | Rate ~0.85%; conservative management unless expanding or hemodynamically significant - then tube thoracostomy |
| Pneumomediastinum | Usually self-limiting; secondary to subcutaneous emphysema tracking |
| Subcutaneous emphysema | Rate ~1.4%; usually benign |
| Tracheal ring fracture | Rare with open technique; more likely with PDT |
| Airway fire | With electrocautery during open tracheostomy; avoid FiO₂ >0.4; if fire occurs, lower FiO₂, remove all foreign bodies, re-intubate via oral route |
| Loss of airway | Most feared immediate complication - requires immediate oral reintubation |
Late/Long-Term Complications
| Complication | Notes |
|---|---|
| Tracheal stenosis | At stoma site, subglottic level, or cuff level. Clinically significant only with >75% luminal reduction; stridor appears when diameter <5 mm. Incidence dramatically reduced since introduction of high-volume, low-pressure cuffs. Meta-analysis shows incidence as low as 0.16% after PDT |
| Tracheomalacia | Weakening and collapse of tracheal wall at cuff site from ischemic necrosis |
| Tracheoinnominate artery fistula (TIF) | Rare (<1%), usually 7-14 days post-procedure; mortality ~85.7%. Sentinel bleed precedes massive hemorrhage. Management: do NOT deflate cuff; obtain CT neck with contrast if stable; if actively bleeding - replace tracheostomy with ETT via cords (cuff distal to bleed) + digital pressure in stoma anteriorly + emergent OR for surgical repair. Prevention: place tube above 3rd ring, keep cuff pressure <25 mmHg |
| Tracheoesophageal fistula | From posterior wall injury or prolonged cuff pressure |
| Delayed stoma closure | After prolonged cannulation (>6 months); may require surgical closure |
| Wound infection | Higher with open surgical technique; manage with local wound care ± antibiotics |
| Granulation tissue | At stoma margins; managed endoscopically |
| Voice changes | From laryngeal injury during prolonged pre-tracheostomy intubation |
11. Tracheostomy Care (Post-Procedure)
- Cuff pressure: Monitor and maintain at 20-25 cmH₂O (15-18 mmHg) - high enough to prevent aspiration, low enough to avoid mucosal ischemia
- Humidification: HME (heat-moisture exchanger) or heated humidifier circuit - prevents drying of secretions and tube obstruction
- Suctioning: Sterile technique; suction catheter should not extend beyond tube tip; limit pass duration to <15 seconds
- Inner cannula care: Clean or replace every 8 hours (or as needed per secretion burden)
- Stoma care: Clean wound, change dressings daily; inspect for redness, granulation tissue, breakdown
- First tube change: Typically after 5-7 days (once a mature tract has formed); earlier if tube is displaced
- Cuff pressure monitoring: Every 4-8 hours; use minimal occlusive volume technique
12. Decannulation
Criteria for safe decannulation:
- Underlying condition has resolved or stabilized
- Patient can protect airway (intact cough, swallow, gag)
- Able to manage secretions without mechanical suctioning
- Respiratory drive sufficient to maintain oxygenation/ventilation without support
- No significant upper airway obstruction above the stoma (assess with flexible laryngoscopy)
Protocol:
- Downsize tube (to smaller size or uncuffed tube)
- Introduce fenestrated tube and speaking valve to test airflow through larynx
- Cap/plug the tube for progressive periods (hours to full day/night)
- Remove tube when patient tolerates complete plugging for 24+ hours without distress
- Stoma will close spontaneously in days to weeks; surgical closure rarely needed
13. Special Populations
- Obesity: PDT may be limited by kit depth; open surgical approach or extra-long adjustable-flange tubes preferred
- ECMO patients: Tracheostomy can be safely performed but complication rate (mainly bleeding) is higher; no difference between PDT and open technique
- COVID-19: Aerosol-generating procedure - full airborne + droplet PPE required; delay recommended until viral shedding subsides (typically >10-14 days)
- Pediatric patients: Surgical tracheostomy preferred; anatomy is smaller, more delicate; stay sutures especially important
- Coagulopathy: Correct coagulopathy before procedure when possible; open technique preferred for direct hemorrhage control
Sources:
- Sabiston Textbook of Surgery, The Biological Basis of Modern Surgical Practice, pp. 960-961
- Current Surgical Therapy, 14th Edition, pp. 1591-1596
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1, pp. 404-406
- Cummings Otolaryngology Head and Neck Surgery
- StatPearls: Tracheostomy - NCBI Bookshelf
This is a shared conversation. Sign in to Orris to start your own chat.