Vascular access for hemodialysis & associated complications. Peritoneal access devices: types of catheter, insertion techniques & associated complications. 7.02 BDTT-023-b Unit-B Complications of dialysis; a. Hemodialysis: acute & long term complications. b. Peritoneal dialysis: mechanical & metabolic complications Peritonitis & exit site infection. Recent advances and research in hemodialysis. BDTT- 7.03 023-c Unit-C a. Nocturnal dialysis. b. Online dialysis. c. Daily dialysis.
hemodialysis vascular access complications recent advances
recent advances hemodialysis 2024 2025 online hemodiafiltration incremental dialysis
Dialysis: Vascular Access, Complications & Recent Advances
UNIT A
1. Vascular Access for Hemodialysis
A. Arteriovenous Fistula (AVF) — Preferred access
- Surgically created direct anastomosis between an artery and vein (most commonly radiocephalic at the wrist, or brachiocephalic)
- Requires maturation time (~6–12 weeks) before use
- Lowest infection risk, longest survival, and least thrombosis
- Requires patent, adequate-caliber veins (assessed by duplex ultrasound pre-operatively)
- "Fistula First Breakthrough Initiative" (FFBI) has significantly increased AVF use and reduced central venous catheter (CVC) use in the USA
B. Arteriovenous Graft (AVG)
- Prosthetic conduit (usually PTFE) connecting artery to vein
- Can be used within 2–4 weeks of placement
- Higher rates of thrombosis and infection than AVF
- Preferred when native vessels are inadequate for fistula creation
C. Central Venous Catheter (CVC) — Last resort / bridge access
- Non-tunneled (temporary): Short-term use; inserted into internal jugular, subclavian, or femoral vein
- Tunneled (cuffed): e.g., Permcath / Hickman — Dacron cuff induces fibrosis to anchor and reduce infection; preferred for longer-term use when AVF/AVG unavailable
- Right internal jugular is preferred site (lower risk of stenosis vs. subclavian)
- Subclavian access is discouraged due to high risk of central venous stenosis impairing future AVF/AVG creation
Vascular Access Complications
| Access Type | Complications |
|---|---|
| AVF | Failure to mature, thrombosis, stenosis, steal syndrome (ischemia to hand), aneurysm, high-output cardiac failure (rare), infection |
| AVG | Thrombosis (most common), stenosis (especially at venous anastomosis), infection/graft loss, seroma, pseudoaneurysm |
| CVC (tunneled) | Infection/bacteremia (most serious — leading to sepsis), biofilm formation, thrombosis, central venous stenosis, pneumothorax (at insertion), air embolism, malposition |
2. Peritoneal Access Devices
Types of Peritoneal Dialysis (PD) Catheters
| Type | Features |
|---|---|
| Tenckhoff catheter (straight or coiled) | Standard; double-cuffed; most widely used |
| Swan-neck catheter | Permanent downward-directed exit site; reduces exit-site infection |
| Toronto Western Hospital (TWH) catheter | Disc-shaped silicone retention; reduces tip migration |
| Column-disc catheter | Flanged; intended to anchor catheter tip |
| Missouri swan-neck catheter | Designed for obese patients |
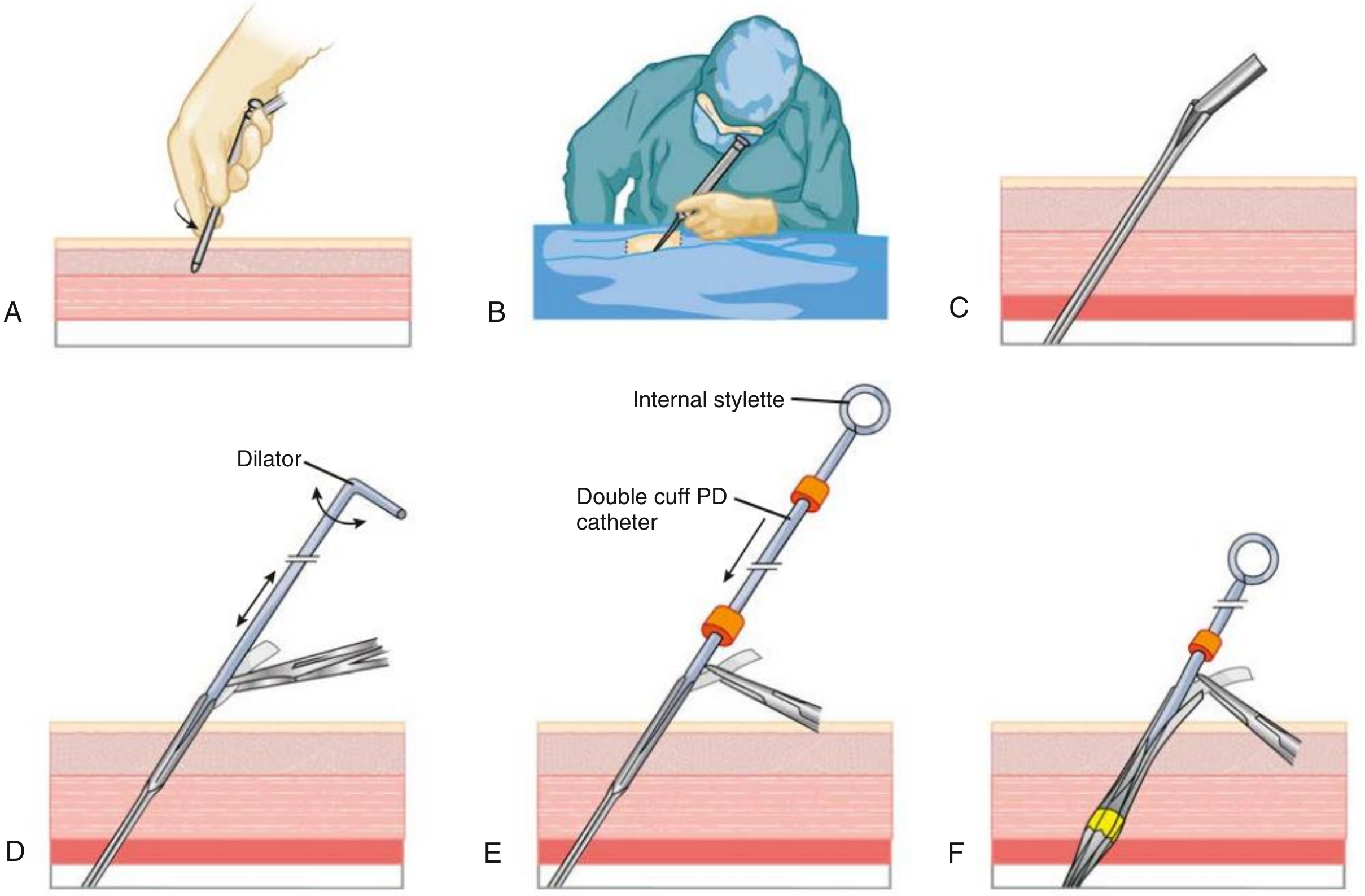
Insertion Techniques
- Small 2–3 cm skin incision; anterior rectus sheath not incised
- Trocar + cannula inserted at 45° through rectus muscle toward pelvis
- Peritoneoscope confirms intraperitoneal position
- Air (600–1000 mL) insufflated to separate peritoneal surfaces
- Bowel loops, adhesions, bladder identified under direct vision
- Spiral sheath advanced to pelvis, dilated to 6 mm; catheter passed over stylet
- Deep cuff implanted in rectus muscle with implanter tool; superficial cuff in subcutaneous tissue
- Can be used immediately for intermittent dialysis (risk of pericatheter leak if used continuously)
- Midline or paramedian incision under general/spinal anesthesia
- Direct visualization; cuffs placed under direct view
- Longer wound healing; pericatheter leak less common early
- Higher infection and outflow failure rates than peritoneoscopic technique
- Veress needle or trocar used for access; guidewire-based placement
- Catheter position confirmed by fluoroscopy
- Fewer complications than open surgery in skilled hands
- Useful in patients with prior abdominal surgery/adhesions
- Direct visualization; omentectomy/omentopexy can be performed simultaneously

Complications of PD Catheter Insertion
| Complication | Notes |
|---|---|
| Bowel perforation | Most feared; incidence 1–1.4% (surgical), 0.8% (peritoneoscopic/fluoroscopic). Managed conservatively if recognized early (bowel rest, IV antibiotics), or surgically |
| Bladder injury | Avoided by ensuring bladder voided before insertion |
| Hemorrhage | Injury to epigastric vessels |
| Pericatheter leaks | More common if used immediately after placement |
| Exit-site/tunnel infection | Early: usually Staphylococcus aureus or epidermidis; reduced by embedding technique |
| Catheter malposition/migration | Tip migrates out of pelvis; causes outflow failure |
| Omental wrapping | Causes complete inflow + outflow failure; requires omentopexy |
UNIT B
3. Complications of Hemodialysis
A. Acute (Intradialytic) Complications
1. Intradialytic Hypotension (IDH) — Most common, 15–30% of sessions
- Definition (KDOQI): drop in SBP ≥20 mmHg or MAP ≥10 mmHg with clinical symptoms
- Causes: excessive/rapid ultrafiltration, impaired cardiac reserve, vasodilation from heat transfer, reduced plasma osmolality, dysautonomia, arrhythmia
- Management: Reduce UF rate, Trendelenburg position, 100–250 mL normal saline bolus; reassess dry weight
- Prevention: limit UF rate (<10–13 mL/kg/hr), individualized dialysate sodium, cooling dialysate, avoid intradialytic food, review antihypertensives, bioimpedance monitoring
- Reassess dry weight
- Reduce interdialytic sodium/fluid intake
- Adjust dialysate calcium and sodium
- Avoid food during dialysis
- Adjust antihypertensive timing
- Increase treatment duration/frequency
2. Muscle Cramps
- Often accompany rapid fluid removal and hypotension
- Management: reduce UF rate, quinine, carnitine, vitamin E
3. Nausea & Vomiting
- Related to hypotension, disequilibrium, or vagal response
4. Headache
5. Dialysis Disequilibrium Syndrome
- Rapid solute removal → cerebral edema (urea osmole effect)
- More common at dialysis initiation in severely uremic patients
- Prevented by slow, gentle first sessions
6. Air Embolism
- Due to faulty tubing connections; potentially fatal; requires immediate left lateral decubitus/Trendelenburg position
7. Dialyzer Reactions
- Type A: Anaphylactic; within 5–20 minutes; IgE-mediated; caused by membrane material or ethylene oxide sterilant; can be fatal
- Type B: Complement-mediated; chest/back pain; less severe; occurs later in session. Reduced with modern biocompatible synthetic membranes (polysulfone, polyacrylonitrile)
8. Arrhythmias
- Triggered by electrolyte shifts (K⁺, Ca²⁺, Mg²⁺), rapid fluid shifts, myocardial ischemia
- Atrial fibrillation prevalent in >20% of HD patients
9. Bleeding
- Anticoagulation (heparin) for circuit patency; regional citrate anticoagulation preferred in high bleeding-risk patients
B. Long-Term (Chronic) Complications of Hemodialysis
1. Cardiovascular Disease — Leading cause of death
- Left ventricular hypertrophy (LVH): from hypertension, volume overload, anemia
- Coronary artery disease: accelerated atherosclerosis
- Myocardial stunning: repetitive HD-induced ischemia (shown by troponin release, regional wall motion abnormalities on echo)
- Pericardial disease: Uremic pericarditis (early dialysis or under-dialysis) vs. non-uremic (well-dialyzed); risk of tamponade; intensify dialysis ± anti-inflammatories ± pericardiocentesis
- Atrial fibrillation: Anticoagulation risk-benefit must be individualized
2. Infections
- Second leading cause of death
- Vascular access infections (especially CVC-related bacteremia) — biofilm on catheter surface
- Hepatitis B/C: Reduced by vaccination, isolation, universal precautions, serologic surveillance
- Uremia-induced immunodeficiency: impaired innate + adaptive immunity; reduced vaccine responses
3. Anemia
- Erythropoietin deficiency (primary driver), iron deficiency, chronic inflammation, blood loss
- Managed with erythropoiesis-stimulating agents (ESAs) + IV iron
4. Mineral Metabolism Disorders
- Secondary hyperparathyroidism → renal osteodystrophy, vascular calcification
- Calciphylaxis (calcific uremic arteriolopathy): rare, painful, life-threatening skin/subcutaneous calcification
5. Hypertension
- Volume-dependent; goal: achieve dry weight; control interdialytic Na⁺/fluid intake
6. Malnutrition (Protein-Energy Wasting)
- Due to hypercatabolism, inadequate intake, dialysate losses
7. Dialysis-Related Amyloidosis
- β₂-microglobulin accumulation → carpal tunnel syndrome, destructive arthropathy (usually after >10 years on HD)
8. Depression and Psychological Morbidity
- Serious, underrecognized; HD patients 3× more likely to commit suicide in Taiwanese registry data
9. Cancer Screening
- Routine screening may not be cost-effective in average HD patients; individualize based on life expectancy and transplant candidacy
4. Peritoneal Dialysis Complications
A. Mechanical Complications
| Complication | Details |
|---|---|
| Catheter malposition / tip migration | Causes outflow failure; tip migrates from pelvis; reposition with guidewire, laparoscope, or laxatives |
| Inflow failure | Kinking, clamps, fibrin plug; flush with heparinized saline; instill tPA (2 mg/40 mL) |
| Outflow failure | Constipation, omental wrapping, catheter migration; omentopexy/partial omentectomy |
| Pericatheter leak | Fluid leaking around catheter; rest dialysis + surgical repair |
| Hernia | Abdominal wall hernias (inguinal, umbilical, incisional) due to intraperitoneal pressure |
| Hydrothorax | Pleuroperitoneal fistula → pleural effusion; consider switch to HD |
| Hemoperitoneum | Usually benign; menstrual, ovulation-related |
| Catheter cuff extrusion | Superficial cuff becomes visible; requires shaving |
B. Metabolic Complications
| Complication | Mechanism |
|---|---|
| Hyperglycemia | Glucose absorption from dialysate (typical PD fluid: 1.5–4.25% dextrose) |
| Obesity / weight gain | Caloric load from glucose absorption |
| Dyslipidemia | Hypertriglyceridemia, low HDL — driven by glucose absorption, protein losses |
| Protein malnutrition | 5–15 g/day protein lost in dialysate; increased losses during peritonitis |
| Hypokalemia | Potassium removal; may require supplementation |
| Hyponatremia | Aquaporin-1 mediated free water transport during hypertonic exchanges |
| Encapsulating peritoneal sclerosis (EPS) | Rare but fatal; progressive peritoneal fibrosis after years of PD; peritoneal membrane failure |
C. Peritonitis & Exit-Site Infection
Peritonitis (CAPD-Associated)
- Cloudy dialysate (cardinal sign)
- WBC in effluent >100/µL with >50% PMNs (ISPD criteria)
- In automated PD (APD) with short dwell time: % PMNs more important than absolute WBC count
- Send dialysate for: cell count + differential, Gram stain, culture in blood culture bottles (improves yield; centrifuge large volume first)
- Staphylococcus species: ~45% (coagulase-negative S. epidermidis, and S. aureus — especially in nasal carriers)
- Gram-negative bacilli
- Candida species (fungal peritonitis → catheter removal mandatory)
- Multiple organisms → suspect secondary peritonitis (bowel perforation)
- Empirical: intraperitoneal (IP) antibiotics covering both gram-positive (vancomycin or first-generation cephalosporin) and gram-negative organisms (aminoglycoside or third-generation cephalosporin)
- Route: IP delivery is preferred (directly into dialysate bag)
- Tailor to culture/sensitivity after 48–72 h
- Duration: typically 2 weeks (gram-positive); 3 weeks (gram-negative, S. aureus)
- Catheter removal indications: refractory peritonitis >5 days, fungal peritonitis, tunnel infection with refractory peritonitis, fecal peritonitis
Exit-Site Infection (ESI) & Tunnel Infection
- ESI: purulent discharge ± erythema/crusting at catheter exit site
- Tunnel infection: infection along subcutaneous catheter tunnel; painful induration/erythema over tunnel; diagnosed clinically ± ultrasound
- Causative organisms: S. aureus (most common), Pseudomonas aeruginosa (difficult to eradicate)
- S. aureus nasal carriage is a major risk factor
- Management: oral/IP antibiotics; refractory ESI or tunnel infection → catheter removal
- Prevention: topical mupirocin or gentamicin at exit site (reduces S. aureus and Pseudomonas ESI)
UNIT C
5. Dialysis Modalities: Nocturnal, Online & Daily Dialysis
A. Nocturnal Dialysis
- 6–8 hours, 3× weekly, while patient sleeps
- Advantages: longer duration → better solute removal (especially middle molecules, phosphate), less cardiovascular stress
- Observational data show: regression of left ventricular mass, improved bone mineral indices, better quality of life
- 3–4 nights/week × 6–8 hours
- Better BP control, reduced phosphate binders requirement
- Concerns: more rapid decline in residual kidney function, more vascular access interventions, patient recruitment difficulty
- One RCT (FHN Nocturnal Trial) confirmed improvements in LV mass and BP but failed to show survival benefit (Brenner & Rector)
B. Short Daily Hemodialysis
- 5–6 sessions/week × 2–4 hours each
- NIH-sponsored FHN (Frequent Hemodialysis Network) Daily Trial — largest RCT:
- ✅ Reduced LV mass
- ✅ Improved self-reported physical health
- ✅ Reduced predialysis serum phosphate
- ✅ Reduced predialysis systolic BP
- ❌ No improvement in survival or hospitalization rates
- ❌ No improvement in serum albumin
- ❌ No reduction in ESA dose
- Shorter interdialytic interval → less fluid accumulation, better hemodynamic tolerability
C. Online Hemodiafiltration (HDF) / Online Dialysis
- Principle: combines diffusion (small solute removal) + convection (middle/large molecule removal), e.g., β₂-microglobulin, FGF-23, cytokines
- Requires ultra-pure water system and specific machine capability
- High-volume online HDF (≥23 L substitution volume per session) associated with:
- Reduced all-cause and cardiovascular mortality in observational studies
- Reduced dialysis-related amyloidosis
- Better phosphate control and reduction in pruritus
- CONVINCE Trial (2023): Large multicenter RCT — online HDF reduced all-cause mortality by ~23% vs. high-flux HD (PMID: 40123557 — Systematic Review: "Alpha to Omega of Dialysis Access" 2025)
- Used increasingly in Europe; gaining ground worldwide as evidence base strengthens
Wearable and Portable Artificial Kidney (Research Frontier)
- Miniaturized dialysis devices aiming for continuous, ambulatory dialysis
- Prototype wearable artificial kidneys (WAK) under clinical trials; ESKD patients could theoretically dialyze continuously while ambulatory
- Challenges: anticoagulation, sorbent regeneration, miniaturized pumps, and regulatory approval
High-Cutoff (HCO) Dialyzers
- Designed to remove large middle molecules (e.g., free light chains in myeloma kidney, cytokines in sepsis-AKI)
- Under investigation in clinical trials
Incremental Dialysis
- Starting with once or twice weekly HD (rather than thrice-weekly) in patients with significant residual kidney function (RKF)
- Preserves RKF longer, reduces cost, better quality of life
- Growing evidence base for safety in carefully selected patients (eGFR >4–5 mL/min/1.73 m²)
Summary Table
| Domain | Key Points |
|---|---|
| Best vascular access | AVF (lowest infection, longest survival) |
| Worst vascular access | CVC (highest infection, biofilm) |
| Best PD catheter insertion | Peritoneoscopic (fewer complications) |
| Most common HD acute complication | Intradialytic hypotension |
| Most common cause of HD death | Cardiovascular disease |
| CAPD peritonitis threshold | >100 WBC/µL + >50% PMNs in effluent |
| Most common peritonitis organism | Coagulase-negative Staphylococcus |
| Peritonitis rate improvement | Y-set: 1/9 months → 1/24 months |
| Nocturnal HD benefit | LV mass regression, BP control, phosphate |
| Online HDF benefit | Convective removal of middle molecules; possible mortality benefit (CONVINCE Trial) |
| Daily HD (FHN Trial) | LV mass ↓, BP ↓, PO₄ ↓ — but no survival benefit |
Telemedicine in dialysis practice. 7.05 BDTT-023-e Unit-E Introduction to kidney transplantation immunology, procedure and Immunosuppressive medications. BDTT-023-f 7.06 Unit-F Live donor and cadaver transplantation; paired exchange transplantation and ABO incompatible transplantation; transplant in sensitized recipients. Explain in for exam purpose
telemedicine hemodialysis dialysis remote monitoring
PMID: 38190131
PMID: 39547777
BDTT-023-d/e/f: Telemedicine in Dialysis, Kidney Transplant Immunology, Donors & Special Transplant Programs
UNIT D — Telemedicine in Dialysis Practice
Definition & Background
Applications in Dialysis Practice
1. Remote Patient Monitoring (RPM) in Home HD & PD
| Parameter Monitored Remotely | Relevance |
|---|---|
| Blood pressure & weight (pre/post-dialysis) | Volume management, dry weight adjustment |
| Blood flow rate, dialysate conductivity | Adequacy monitoring |
| Ultrafiltration volume | Intradialytic hypotension prevention |
| Dialysis machine alarms | Safety alerts to nursing staff |
| Patient-reported symptoms | Early complication detection |
| Laboratory results (uploaded portals) | Kt/V, hemoglobin, phosphate trending |
2. Telehealth Consultation
- Video consultations replace in-center visits for stable patients
- Reduces patient travel burden (especially important for rural/remote patients)
- Allows prescribing adjustments, medication reviews, and education sessions remotely
- Particularly useful for pre-dialysis education, modality selection counseling, and diet/fluid counseling
3. Virtual Training for Home Dialysis Patients
- Step-by-step video guidance for PD exchanges and HD cannulation
- Reduces training time and supports caregiver confidence
- Platforms include telehealth apps with interactive protocols
Evidence Base
| Study | Finding |
|---|---|
| Mata-Lima et al. 2024 (Syst. Review) [PMID: 39547777] | RPM can reduce costs, improve efficiency of healthcare resources, reduce human error, and improve quality of life in kidney patients |
| Biebuyck et al. 2022 (Syst. Review) [PMID: 35999512] | Telehealth interventions in PD care: feasible, high patient acceptance, may improve clinical outcomes |
| Nygård et al. 2022 (Syst. Review) [PMID: 36600376] | Remote monitoring in home dialysis: technically feasible; limited evidence on hard outcomes |
| El Shamy 2026 (Review) [PMID: 41123424] | Remote monitoring in PD remains underutilized despite strong evidence of feasibility and benefit |
| Lew et al. 2024 (CJASN Review) [PMID: 38190131] | AI and artificial neural networks can optimize and personalize dialysis prescriptions; healthcare equity challenges remain |
Benefits of Telemedicine in Dialysis
- Fewer clinic visits → reduced patient burden, lower infection exposure
- Early detection of fluid overload, hypertension, vascular access problems
- Improved adherence through remote coaching and reminders
- Support for home dialysis expansion — enables more patients to dialyze at home safely
- Reduced hospitalizations via proactive problem-solving
- Healthcare equity — access to specialist nephrology in underserved areas
Challenges & Limitations
- Digital divide: elderly/low-literacy patients struggle with technology
- Regulatory barriers: reimbursement policies vary by country
- Data security and patient privacy concerns
- Limited RCT evidence on mortality/hospitalization hard outcomes
- Provider workflow changes required
- Internet connectivity issues in rural/remote areas
Future Directions
- AI-driven prescription optimization: algorithms adjusting UF rates, session length based on real-time biometrics
- Wearable sensors: continuous BP and fluid monitoring between sessions
- Virtual reality for patient education
- Integration with electronic health records (EHR) for seamless care coordination
UNIT E — Introduction to Kidney Transplantation Immunology, Procedure & Immunosuppressive Medications
1. Immunology of Kidney Transplantation
The Alloimmune Response
Key Immunologic Concepts
- HLA Class I (A, B, C) — expressed on all nucleated cells; recognized by CD8⁺ cytotoxic T-cells
- HLA Class II (DR, DQ, DP) — expressed on antigen-presenting cells (APCs), activated endothelium; recognized by CD4⁺ helper T-cells
- HLA mismatch between donor and recipient drives alloreactivity
| Pathway | Mechanism |
|---|---|
| Direct | Recipient T-cells recognize intact donor HLA on donor APCs (dendritic cells in the graft); major driver of acute rejection |
| Indirect | Recipient T-cells recognize donor HLA peptides presented by self APCs; major driver of chronic rejection |
| Semi-direct | Recipient APCs acquire intact donor MHC molecules |
- Signal 1: Antigen recognition — TCR binds HLA-peptide complex
- Signal 2: Co-stimulation — CD28 on T-cell binds B7 (CD80/86) on APC → activates NF-κB and AP-1 → IL-2 production
- Signal 3: Cytokine proliferation signal — IL-2 binds IL-2R → mTOR activation → T-cell proliferation
- CD4⁺ T-helper cells provide signals to B-cells → plasma cells → donor-specific antibodies (DSA)
- DSA bind donor HLA on graft endothelium → complement activation → C4d deposition → endothelial injury → antibody-mediated rejection (AMR)
2. Types of Rejection
| Type | Timing | Mechanism | Key Features |
|---|---|---|---|
| Hyperacute | Minutes–hours | Preformed antibodies (anti-HLA or anti-ABO) → immediate complement activation | Now rare due to crossmatch testing; graft thrombosis |
| Accelerated acute | 2–5 days | Sensitized T-cells from prior exposure | |
| Acute T-cell–mediated (TCMR) | Days–weeks | Clonal T-cell expansion; tubulitis, interstitial infiltrate on biopsy | Responds to steroids ± rATG |
| Acute antibody-mediated (AMR) | Days–weeks | DSA → endothelial injury; neutrophils/macrophages in peritubular capillaries; C4d⁺ | Plasma exchange + IVIG ± rituximab |
| Chronic active AMR | Months–years | Indolent humoral response → transplant glomerulopathy, microvascular inflammation | Leading cause of late graft loss |
3. Transplant Procedure (Brief)
- ABO blood group compatibility
- HLA typing (recipient and donor)
- Crossmatch: Donor lymphocytes + recipient serum — positive crossmatch = preformed DSA = contraindication (unless desensitized)
- Panel Reactive Antibody (PRA) / calculated PRA: measures degree of sensitization
- Heterotopic transplant: donor kidney placed in iliac fossa (extraperitoneal)
- Donor renal artery → recipient external iliac artery (end-to-side)
- Donor renal vein → recipient external iliac vein
- Ureter → bladder (ureteroneocystostomy, often with ureteral stent)
- Native kidneys left in situ (unless causing hypertension, infection, pain, or polycystic kidneys)
4. Immunosuppressive Medications
Phase 1: Induction Therapy (at time of transplant)
90% of US recipients receive induction (SRTR 2018): 72% T-cell depleting, 20% IL-2 receptor antibody.
| Agent | Type | Target | Dose | Notes |
|---|---|---|---|---|
| Basiliximab (Simulect) | Non-depleting | IL-2 receptor (CD25) on T-cells | 20 mg IV days 0 and 4 | Minimal side effects; low immunologic risk patients |
| rATG (Thymoglobulin) | Depleting | Multiple T-cell surface antigens | 1–1.5 mg/kg IV × 4–14 days | High immunologic risk; more infections/malignancy |
| Alemtuzumab (Campath) | Depleting | CD52 on T- and B-cells | 30–60 mg × 1–2 doses | Prolonged lymphopenia (6–12 months); cost-prohibitive in USA |
| Methylprednisolone | — | Broad anti-inflammatory | 250–500 mg IV at induction | Used with all induction regimens |
Phase 2: Maintenance Immunosuppression
A. Calcineurin Inhibitors (CNI) — Backbone
| Drug | Mechanism | Key Side Effects |
|---|---|---|
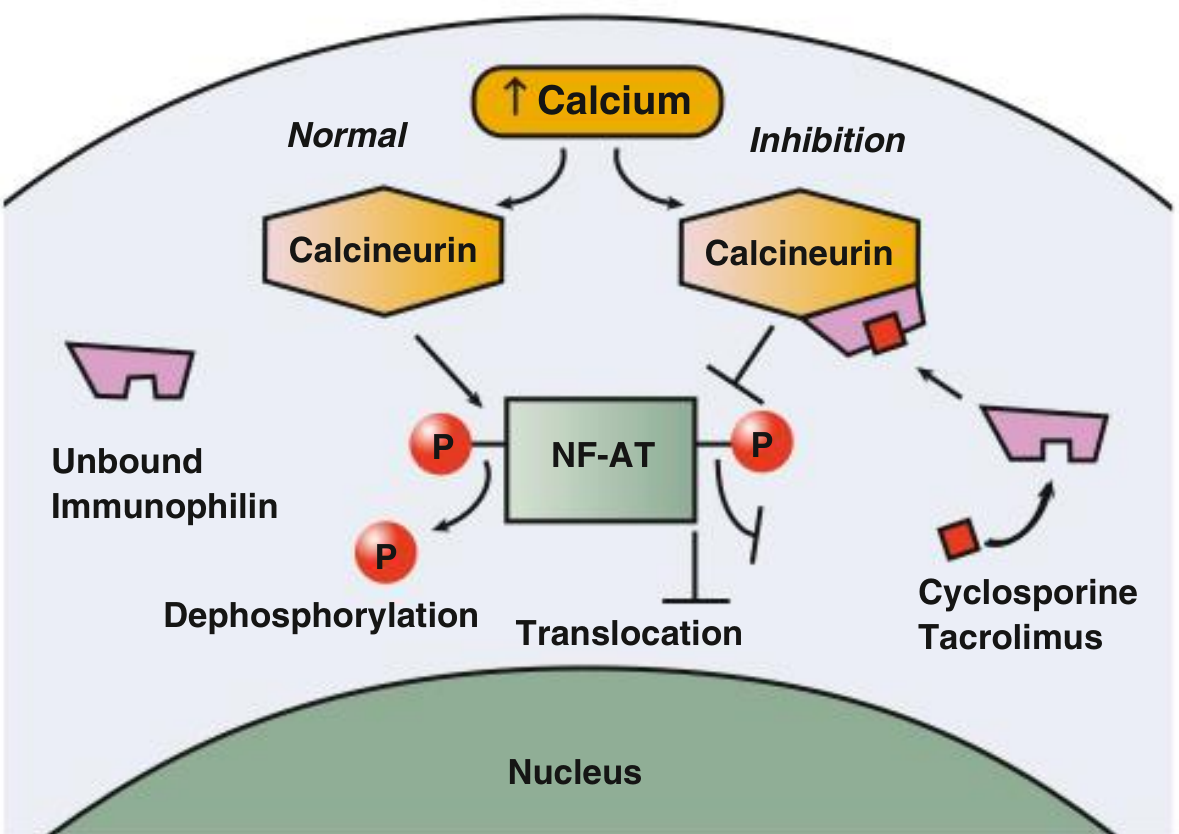
| Tacrolimus (FK506, Prograf) | Binds FKBP12 → inhibits calcineurin → blocks NF-AT → ↓ IL-2 transcription | New-onset diabetes (NODAT), nephrotoxicity, neurotoxicity (tremor), hypertension, alopecia, hypomagnesemia |
| Cyclosporine (Neoral) | Binds cyclophilin → inhibits calcineurin → ↓ IL-2 | Nephrotoxicity, hypertension, hyperlipidemia, gingival hyperplasia, hirsutism, less NODAT than tacrolimus |
B. Antiproliferative Agents
| Drug | Mechanism | Key Side Effects |
|---|---|---|
| Mycophenolate mofetil (MMF) / Mycophenolic acid (MPA) | Inhibits inosine monophosphate dehydrogenase (IMPDH) → blocks de novo purine synthesis → inhibits lymphocyte proliferation | Leukopenia, GI intolerance (diarrhea, nausea), anemia; MPA (enteric-coated) has fewer GI effects |
| Azathioprine (AZA) | Purine analog → inhibits DNA synthesis | Leukopenia, hepatotoxicity, pancreatitis; interaction with allopurinol (life-threatening myelosuppression) |
C. mTOR Inhibitors
| Drug | Mechanism | Key Side Effects | Special Use |
|---|---|---|---|
| Sirolimus (Rapamycin) | Binds FKBP12 → inhibits mTOR → blocks G1→S cell cycle progression | Impaired wound healing, proteinuria, hyperlipidemia, pneumonitis, delayed graft function recovery | Avoid early post-transplant; useful in CNI-sparing protocols, post-skin cancer |
| Everolimus | Same as sirolimus | Similar to sirolimus | TRANSFORM trial: reduced-CNI everolimus comparable to standard CNI/MMF at 12 months |
D. Corticosteroids
- Mechanism: Suppress cytokines (IL-1, IL-2, TNF-α), inhibit NF-κB via IκB induction, inhibit phospholipase A2 via lipocortin → block prostaglandins/leukotrienes
- Induction: Methylprednisolone 250–500 mg IV
- Maintenance: Prednisone 5 mg/day (or steroid-free protocols)
- Acute rejection treatment: Methylprednisolone 3–5 mg/kg (250–500 mg) IV × 3–5 days
- Side effects: Diabetes, hypertension, hyperlipidemia, osteoporosis, avascular necrosis, cataracts, peptic ulcer disease, Cushing syndrome, infection
E. Belatacept (Costimulation Blocker)
- Fusion protein (CTLA4-Ig); blocks CD28–B7 co-stimulation (Signal 2)
- IV monthly infusion; avoids CNI nephrotoxicity
- Slight higher acute rejection risk; associated with post-transplant lymphoproliferative disorder (PTLD) in EBV-seronegative recipients
- Used in CNI-intolerant patients
Phase 3: Treatment of Acute Rejection
| Rejection Type | Treatment |
|---|---|
| Acute TCMR | Methylprednisolone IV × 3–5 days; steroid-resistant: rATG |
| Acute AMR | Plasma exchange (2–5 sessions) + IVIG (100–200 mg/kg after each PE) ± Rituximab (375 mg/m²) ± Bortezomib (1.3 mg/m² × 4 doses) ± Eculizumab |
| Drug | Notable Side Effects |
|---|---|
| Tacrolimus | NODAT, nephrotoxicity, neurological (tremor), alopecia |
| Cyclosporine | Hypertension, hirsutism, gingival hyperplasia, nephrotoxicity |
| MMF | GI intolerance, leukopenia, anemia |
| Azathioprine | Myelosuppression (allopurinol interaction!), hepatitis |
| Corticosteroids | Diabetes, osteoporosis, Cushing's, peptic ulcer |
| Sirolimus/Everolimus | Poor wound healing, proteinuria, pneumonitis |
| Belatacept | PTLD risk in EBV-seronegative recipients |
UNIT F — Donor Types, Paired Exchange, ABO-Incompatible & Sensitized Recipients
1. Live Donor Transplantation
- Better graft survival (longer half-life)
- Shorter cold ischemia time
- Elective scheduling; better pre-transplant optimization
- Superior short- and long-term outcomes
- Comprehensive medical (rule out diabetes, hypertension, cardiovascular disease, CKD, malignancy), surgical, and psychosocial evaluation
- CT angiogram or MR angiogram of kidneys: defines vascular anatomy, excludes anomalies, determines which kidney to remove
- Left kidney preferred (longer renal vein → easier anastomosis)
- Donor mortality: ~0.03%
2. Deceased Donor (Cadaver) Transplantation
A. Brain-Dead Donors (DBD — Donation after Brain Death)
- Cardiac function maintained on ventilator
- Organs well-perfused until procurement
- Standard deceased donor
B. Donors after Cardiac/Circulatory Death (DCD)
- Cardiopulmonary support withdrawn in controlled setting after catastrophic brain injury (not meeting brain-death criteria)
- Organ procurement after cardiac arrest → higher warm ischemia time
- Higher risk of delayed graft function (DGF), but comparable long-term outcomes to DBD
- DCD donors represent ~10% of deceased donors in the USA (rapidly increasing)
- Kidney Donor Profile Index (KDPI): Score 1–100; lower score = better predicted kidney longevity
- Estimated Post-Transplant Survival (EPTS) score for recipients: lowest EPTS (longest predicted survival) get the best KDPI kidneys
- Extended Criteria Donors (ECD): Age ≥60, or age 50–59 with ≥2 of: history of hypertension, terminal creatinine >1.5 mg/dL, or CVA as cause of death → higher DGF risk but expand donor pool
3. Paired Kidney Exchange (PKE) Transplantation
Concept
- Pair A: Donor A (blood group A) → incompatible with Recipient A (blood group B)
- Pair B: Donor B (blood group B) → incompatible with Recipient B (blood group A)
- Exchange: Donor A gives kidney to Recipient B; Donor B gives kidney to Recipient A
Programs
- National Kidney Registry (NKR) — USA
- UK Living Kidney Sharing Schemes
- Extended to chains and non-directed altruistic donors (stranger/Good Samaritan donors initiate chains)
Outcomes
- Paired exchange accounted for 14% of living donor transplants in the USA in 2018 (up from 5% in 2009)
- No difference in graft or patient survival at 3, 5, and 7 years vs. direct living donor transplants (NKR data) — despite higher risk-factor burden (Comprehensive Clinical Nephrology, 7th Ed.)
Logistics
- Surgeries must be simultaneous (to prevent donor withdrawal after recipient receives kidney)
- Complex matching algorithms (maximize compatible pairs)
4. ABO-Incompatible (ABOi) Transplantation
Background
Desensitization Protocol
- Rituximab (anti-CD20) given 2–4 weeks pretransplant → depletes B-cells → reduces antibody production
- Plasmapheresis (PE) — removes circulating anti-A/B isohemagglutinins (2–4 sessions until titers acceptable, typically IgG titer ≤1:8 to 1:16)
- IVIG — after each PE session (100–200 mg/kg) or high-dose (1–2 g/kg) → modulates B-cell function
- Some protocols add immunoadsorption columns (A/B antigen-specific) — more efficient antibody removal than PE
- Maintenance immunosuppression as per standard protocol
5. Transplantation in Sensitized Recipients
Who is Sensitized?
- Prior kidney transplant
- Blood transfusions
- Pregnancy
- PRA 0–20%: Low sensitization
- PRA 20–80%: Moderate
- PRA >80%: Highly sensitized (extremely difficult to find compatible donor)
- Virtual crossmatch (cPRA): Uses HLA antibody specificity to computationally predict crossmatch results
Options for Sensitized Recipients
| Strategy | Description |
|---|---|
| Waiting for compatible deceased donor | Long wait; favorable crossmatch required |
| Paired kidney exchange | Find "less incompatible" donor through exchange, then desensitize |
| Desensitization protocol | Reduce DSA level sufficiently to perform transplant across a positive crossmatch |
| Hybrid approach | Exchange + desensitization (for highly sensitized patients) |
Desensitization Protocol for HLA-Incompatible Transplantation
| Agent | Mechanism | Role |
|---|---|---|
| Plasmapheresis | Removes DSA | 2–5 sessions pre- and post-transplant |
| IVIG (high-dose 2 g/kg) | Inhibits antibody, modulates B-cells | Given after plasmapheresis |
| Rituximab (375 mg/m²) | Anti-CD20; B-cell depletion | Given pretransplant |
| Bortezomib (1.3 mg/m² × 4 doses) | Proteasome inhibitor; plasma cell death | For refractory DSA |
| Eculizumab | Anti-C5; terminal complement inhibition | Peri-transplant to prevent complement-mediated endothelial injury in high-risk crossmatch-positive transplants |
Summary Table for Exam
| Topic | Key Exam Points |
|---|---|
| Telemedicine | RPM transmits HD/PD data; benefits: home dialysis support, fewer clinic visits, early complication detection; challenges: digital divide, regulatory barriers |
| Allorecognition | Direct (acute rejection) vs. indirect (chronic rejection) pathways; 3-signal T-cell activation model |
| Rejection classification | Banff criteria; C4d for AMR; acute TCMR (tubulitis, interstitial infiltrate) vs. AMR (peritubular capillaritis, C4d) |
| Standard maintenance IS | Tacrolimus + MMF ± Prednisone |
| Most nephrotoxic IS | CNIs (tacrolimus, cyclosporine) |
| NODAT risk | Tacrolimus > cyclosporine |
| Acute rejection Rx | TCMR: steroids ± rATG; AMR: plasmapheresis + IVIG ± rituximab |
| Best living donor | Left kidney (longer vein); laparoscopic nephrectomy |
| DCD donors | Higher DGF risk; comparable long-term outcomes to DBD |
| Paired exchange | 14% of US living donor transplants (2018); no survival difference vs. direct donation |
| ABOi transplant | Rituximab + plasmapheresis + IVIG; reduce isohemagglutinin titer pretransplant |
| Sensitized recipient | Desensitize with PE + IVIG + rituximab ± bortezomib ± eculizumab; hybrid with PKE |
| KDPI | Lower score = better kidney; matched to lowest EPTS recipients |
Telemedicine in dialysis practice. 7.05 BDTT-023-e Unit-E Introduction to kidney transplantation immunology, procedure and Immunosuppressive medications. BDTT-023-f 7.06 Unit-F Live donor and cadaver transplantation; paired exchange transplantation and ABO incompatible transplantation; transplant in sensitized recipients. Explain in easy way for exam
BDTT-023-d/e/f — Easy Exam Notes
UNIT D — Telemedicine in Dialysis Practice
What is Telemedicine?
How is it Used in Dialysis?
1. Remote Patient Monitoring (RPM)
| What is Monitored | Why it Matters |
|---|---|
| Blood pressure & weight | Detect fluid overload early |
| Ultrafiltration volume | Prevent hypotension |
| Blood flow rate | Check adequacy |
| Machine alarms | Safety |
| Lab results (uploaded) | Adjust prescriptions |
2. Video Consultations
- Replace routine in-center visits for stable patients
- Used for: medication reviews, diet counseling, blood pressure review, pre-dialysis education
- Especially valuable for patients in rural or remote areas
3. Virtual Training
- Patients learn PD exchanges and HD cannulation via video guides
- Reduces time needed for in-person training
Benefits
| Benefit | Explanation |
|---|---|
| Fewer hospital visits | Saves time & reduces infection exposure |
| Early detection of problems | Remote data catches issues before they become emergencies |
| Supports home dialysis | More patients can safely dialyze at home |
| Better access | Rural patients get specialist care |
| Cost reduction | Fewer hospital admissions |
Challenges
- Digital divide — elderly patients struggle with technology
- Privacy concerns — patient data security
- Connectivity — poor internet in rural areas
- No RCT evidence yet on survival benefit
- Reimbursement — regulatory/payment policies vary by country
Future
- AI algorithms adjusting dialysis prescriptions automatically
- Wearable sensors for continuous BP and fluid monitoring
- Integration with Electronic Health Records (EHR)
📖 COVID-19 was a major accelerant for telemedicine adoption in dialysis globally. Patient acceptance is very high. — Lew et al., CJASN 2024
UNIT E — Kidney Transplantation: Immunology, Procedure & Immunosuppression
Why Does the Body Reject a Transplanted Kidney?
Key Immunology Concepts
HLA (Human Leukocyte Antigens)
- Proteins on cell surfaces that act as "identity badges"
- HLA Class I (A, B, C): on all nucleated cells → recognized by CD8⁺ T-cells
- HLA Class II (DR, DQ, DP): on immune cells & activated endothelium → recognized by CD4⁺ T-cells
- The more HLA mismatches between donor and recipient → higher rejection risk
Two Pathways of Rejection
| Pathway | How it Works | Main Role |
|---|---|---|
| Direct recognition | Recipient T-cells see donor HLA directly on donor cells | Drives ACUTE rejection |
| Indirect recognition | Recipient T-cells see donor HLA peptides presented by recipient's own APCs | Drives CHRONIC rejection |
T-Cell Activation — The 3-Signal Model
Signal 1: T-cell receptor sees donor HLA antigen
Signal 2: Co-stimulation (CD28 on T-cell binds B7 on APC) → NF-κB → IL-2 production
Signal 3: IL-2 binds IL-2 receptor → mTOR → T-cell proliferation
Key exam point: Each signal corresponds to a drug target!
- Signal 1 blocked by: CNIs (tacrolimus, cyclosporine) → block IL-2 production
- Signal 2 blocked by: Belatacept (CTLA4-Ig) → blocks CD28–B7 co-stimulation
- Signal 3 blocked by: mTOR inhibitors (sirolimus, everolimus)
Types of Rejection (Simple Table)
| Type | When? | Mechanism | Biopsy Finding | Treatment |
|---|---|---|---|---|
| Hyperacute | Minutes after surgery | Pre-formed antibodies (anti-HLA or anti-ABO) → complement → thrombosis | Fibrin thrombi, necrosis | Prevention only (crossmatch test); no treatment — graft lost |
| Acute T-cell mediated (TCMR) | Days to weeks | CD4/CD8 T-cells infiltrate graft | Tubulitis + interstitial lymphocytes | IV methylprednisolone; if resistant: rATG |
| Acute Antibody-mediated (AMR) | Days to weeks | Donor-specific antibodies (DSA) damage graft vessels | Neutrophils in peritubular capillaries; C4d positive | Plasmapheresis + IVIG ± rituximab |
| Chronic (active AMR) | Months to years | Ongoing antibody injury | Transplant glomerulopathy | Hard to reverse; adjust IS |
The Transplant Procedure (Simplified)
- ABO blood group match
- HLA typing of donor and recipient
- Crossmatch test: Mix donor cells + recipient blood serum. If antibodies present → POSITIVE crossmatch = danger of hyperacute rejection → usually contraindication to transplant
- Donor kidney placed in the right or left iliac fossa (lower abdomen) — NOT where the original kidneys are (those stay unless problematic)
- Artery → external iliac artery
- Vein → external iliac vein
- Ureter → bladder (ureteroneocystostomy)
- Takes ~3–4 hours
Immunosuppressive Medications
Phase 1: INDUCTION (at the time of transplant)
| Drug | Type | How it Works | Key Notes |
|---|---|---|---|
| Basiliximab | Non-depleting | Blocks IL-2 receptor → stops T-cell growth | Low-risk patients; minimal side effects |
| rATG (Thymoglobulin) | T-cell depleting | Destroys T-cells | High-risk patients; more infections |
| Alemtuzumab | T-cell + B-cell depleting | Targets CD52 on lymphocytes | Long lymphopenia (6–12 months) |
| Methylprednisolone | Steroid | Broad anti-inflammatory | Always given at time of transplant |
Phase 2: MAINTENANCE (long-term)
A. Calcineurin Inhibitors (CNIs) — BACKBONE of maintenance
| Drug | How it Works | Side Effects to Know |
|---|---|---|
| Tacrolimus (FK506) | Binds FKBP12 → inhibits calcineurin → blocks IL-2 gene → T-cells can't multiply | NODAT (new diabetes), nephrotoxicity, tremor, alopecia, hypomagnesemia |
| Cyclosporine | Binds cyclophilin → same mechanism | Hypertension, gum hyperplasia, hirsutism, hyperlipidemia, nephrotoxicity |
🧠 Memory: "Tacrolimus takes your Tremor and Type 2 diabetes" | "Cyclosporine = Curly hair + Calloused gums"
B. Antiproliferative Agents — Stop lymphocyte division
| Drug | How it Works | Side Effects |
|---|---|---|
| Mycophenolate Mofetil (MMF) | Blocks IMPDH → stops purine synthesis → lymphocytes can't divide (they rely on de novo synthesis) | Diarrhea, leukopenia, anemia |
| Azathioprine (AZA) | Purine analog → inhibits DNA synthesis | Myelosuppression; DANGER: never give with allopurinol (causes fatal bone marrow suppression) |
C. mTOR Inhibitors
| Drug | How it Works | Side Effects | When Used |
|---|---|---|---|
| Sirolimus | Blocks mTOR → stops cell cycle G1→S | Poor wound healing, proteinuria, hyperlipidemia, pneumonitis | Avoid early post-transplant; CNI-sparing; skin cancer history |
| Everolimus | Same as sirolimus | Similar | TRANSFORM trial: comparable outcomes with reduced CNI |
D. Corticosteroids
- Prednisone 5 mg/day (maintenance)
- Side effects: Diabetes, osteoporosis, Cushing syndrome, peptic ulcer, hypertension, cataracts, avascular necrosis of hip
E. Belatacept (newer agent)
- Blocks Signal 2 (CD28–B7 co-stimulation)
- IV monthly infusion
- Avoids CNI nephrotoxicity
- Risk: PTLD in EBV-seronegative recipients (contraindicated)
Phase 3: TREATMENT OF REJECTION
| Rejection Type | Treatment |
|---|---|
| Acute TCMR | Methylprednisolone 500 mg IV × 3 days; if resistant → rATG |
| Acute AMR | Plasmapheresis (remove DSA) + IVIG (100–200 mg/kg) ± Rituximab ± Bortezomib ± Eculizumab |
Side Effects — Quick Memory Table
| Drug | Most Important Side Effect |
|---|---|
| Tacrolimus | NODAT (new diabetes) |
| Cyclosporine | Gingival hyperplasia + hirsutism |
| MMF | Diarrhea + leukopenia |
| Azathioprine | Allopurinol interaction → fatal myelosuppression |
| Steroids | Diabetes + osteoporosis |
| Sirolimus | Poor wound healing |
| Belatacept | PTLD (EBV-seronegative) |
UNIT F — Donor Types, Paired Exchange, ABOi & Sensitized Recipients
1. Live Donor Transplantation
- Better graft survival
- Shorter waiting time
- Planned surgery → better preparation
- Less ischemia time
- Must be healthy: no diabetes, hypertension, CKD, malignancy, cardiovascular disease
- CT or MR angiogram → look at kidney anatomy, decide which kidney to take
- Left kidney preferred (longer renal vein = easier surgery)
- Psychosocial evaluation to confirm voluntary, informed decision
- Donor mortality: very low (~0.03%)
2. Deceased (Cadaveric) Donor Transplantation
A. Brain-Dead Donor (DBD)
- Patient declared brain-dead (irreversible loss of all brain function)
- Heart still beating on life support
- Best organ quality (good perfusion until retrieval)
- Most common type of deceased donor
B. Donation after Cardiac Death (DCD)
- Patient has devastating brain injury but doesn't meet brain-death criteria
- Family/team decides to withdraw life support
- Organs harvested after the heart stops
- More warm ischemia time → higher risk of delayed graft function (DGF)
- Long-term outcomes similar to DBD
- ~10% of deceased donors in USA
- KDPI (Kidney Donor Profile Index): 1–100; lower = better kidney
- EPTS (Estimated Post-Transplant Survival): Best kidneys go to recipients with best predicted survival
3. Paired Kidney Exchange (PKE) Transplantation
The Problem
The Solution: Swap donors!
Imagine:
🔴 Patient A (blood group B) + Donor A (blood group A) → INCOMPATIBLE
🔵 Patient B (blood group A) + Donor B (blood group B) → INCOMPATIBLE
Solution: Donor A → Patient B | Donor B → Patient A ✅
Both patients get a compatible kidney!
Key Points
- Surgeries are simultaneous (so no one backs out after their recipient gets a kidney)
- Extended to chains — a non-directed (altruistic/stranger) donor starts a chain of transplants
- National Kidney Registry (USA): Computerized matching system
- PKE = 14% of living donor transplants in USA (2018), up from 5% in 2009
- Outcomes: Same graft and patient survival at 3, 5, 7 years vs. direct living donation
4. ABO-Incompatible (ABOi) Transplantation
The Problem
The Solution: Remove those antibodies first!
| Step | Agent | Purpose |
|---|---|---|
| 2–4 weeks before | Rituximab (anti-CD20) | Destroys B-cells → stops antibody production |
| 1–2 weeks before | Plasmapheresis × 2–4 sessions | Physically removes anti-A/anti-B antibodies from blood |
| After each PE | IVIG (100–200 mg/kg) | Neutralizes remaining antibodies + modulates immune response |
| At transplant | Standard IS (TAC + MMF + steroids) | Prevent rejection |
| Goal | Isohemagglutinin titer ≤1:8 | Safe level to proceed with transplant |
If PKE can find a compatible pair, that's preferred over ABOi. But when no exchange is possible, ABOi with desensitization is a valid option.
5. Transplantation in Sensitized Recipients
Who is Sensitized?
- Previous kidney transplant (most common)
- Blood transfusions
- Pregnancy
How is Sensitization Measured?
| PRA Level | Meaning |
|---|---|
| 0–20% | Low sensitization — easy to find donor |
| 20–80% | Moderate sensitization |
| >80% | Highly sensitized — very hard to find compatible donor; long wait list |
| 100% | Virtually impossible to find compatible donor without desensitization |
Options for Sensitized Patients
| Option | When Used |
|---|---|
| Wait for compatible deceased donor | Acceptable sensitization; access to compatible kidney eventually |
| Paired kidney exchange | Find less-incompatible donor via exchange; reduce DSA with desensitization |
| Desensitization + transplant | Positive crossmatch; reduce DSA level then transplant |
| Hybrid | Exchange to find a "less incompatible" donor + desensitization |
Desensitization Protocol
Plasmapheresis × 2–5 sessions (removes DSA from blood)
+
IVIG (2 g/kg total) — neutralizes antibodies, modulates B-cells
+
Rituximab 375 mg/m² — depletes B-cells → reduces DSA production
+/-
Bortezomib (1.3 mg/m² × 4 doses) — kills plasma cells → long-term DSA reduction
+/-
Eculizumab — anti-C5 complement blocker → protects graft endothelium peri-transplant
Summary — All 4 Special Transplant Scenarios
| Situation | Problem | Solution |
|---|---|---|
| Incompatible blood groups, another incompatible pair exists | Blood type mismatch | Paired kidney exchange |
| Incompatible blood groups, no exchange available | Anti-A/anti-B antibodies | ABOi desensitization (rituximab + PE + IVIG) |
| Positive HLA crossmatch (sensitized) | Anti-HLA DSA | HLA desensitization (PE + IVIG ± rituximab ± bortezomib) |
| Highly sensitized, positive crossmatch + incompatible donor | Both problems | Hybrid: exchange + desensitization |
One-Page Exam Cheat Sheet
IMMUNOSUPPRESSION REGIMEN (Standard):
Induction: rATG (high risk) or Basiliximab (low risk) + Methylprednisolone
Maintenance: TACROLIMUS + MMF ± PREDNISONE
Rejection Rx: TCMR → Steroids ± rATG
AMR → Plasmapheresis + IVIG ± Rituximab
KEY DRUG SIDE EFFECTS:
Tacrolimus → New-onset Diabetes (NODAT)
Cyclosporine → Gum hyperplasia + Hirsutism
MMF → Diarrhea + Leukopenia
Azathioprine → NEVER with Allopurinol!
Steroids → Diabetes + Osteoporosis
Sirolimus → Poor wound healing
REJECTION TYPES:
Hyperacute → Pre-formed antibodies → minutes → Prevent with crossmatch
Acute TCMR → Days–weeks → Tubulitis → Steroids
Acute AMR → Days–weeks → C4d+ → PE + IVIG + Rituximab
Chronic AMR → Months–years → Transplant glomerulopathy → Leading cause of late graft loss
PAIRED EXCHANGE:
PKE = 14% of US living donor transplants
Simultaneous surgeries → Same outcomes as direct donation
DESENSITIZATION:
ABOi → Rituximab + Plasmapheresis + IVIG → Titer ≤1:8
HLA+ → Plasmapheresis + IVIG ± Rituximab ± Bortezomib ± Eculizumab