Development of branchial arches and their anomalies with diagrams. Ms ent university exam pattern for 20 marks.
branchial arch development anomalies diagram ENT
Development of Branchial Arches and Their Anomalies
INTRODUCTION
EMBRYOLOGY OF THE BRANCHIAL APPARATUS
Timing and Formation
- Development begins at 4 weeks' gestation
- 6 branchial arches form in total (numbered 1, 2, 3, 4, 5, 6)
- The 5th arch obliterates almost as soon as it appears and has no significant derivatives
- Between adjacent arches: external clefts (grooves) on the ectoderm side, and internal pouches on the endoderm (pharyngeal) side
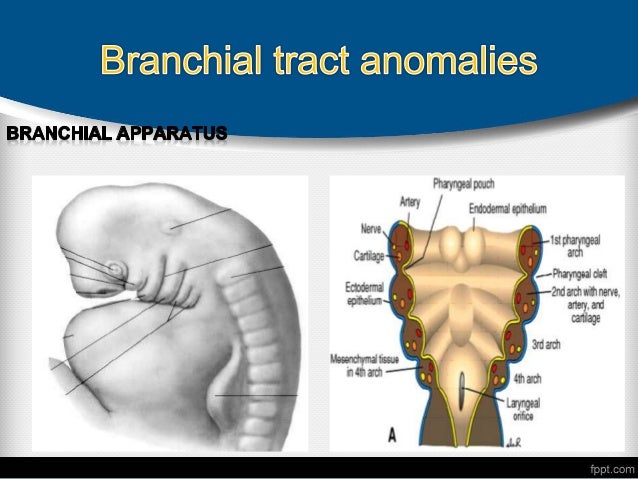
Components of Each Arch
- A cranial nerve (its nerve)
- A cartilaginous bar (skeletal element)
- A muscle group
- An aortic arch artery
DIAGRAM 1 - The Branchial Apparatus
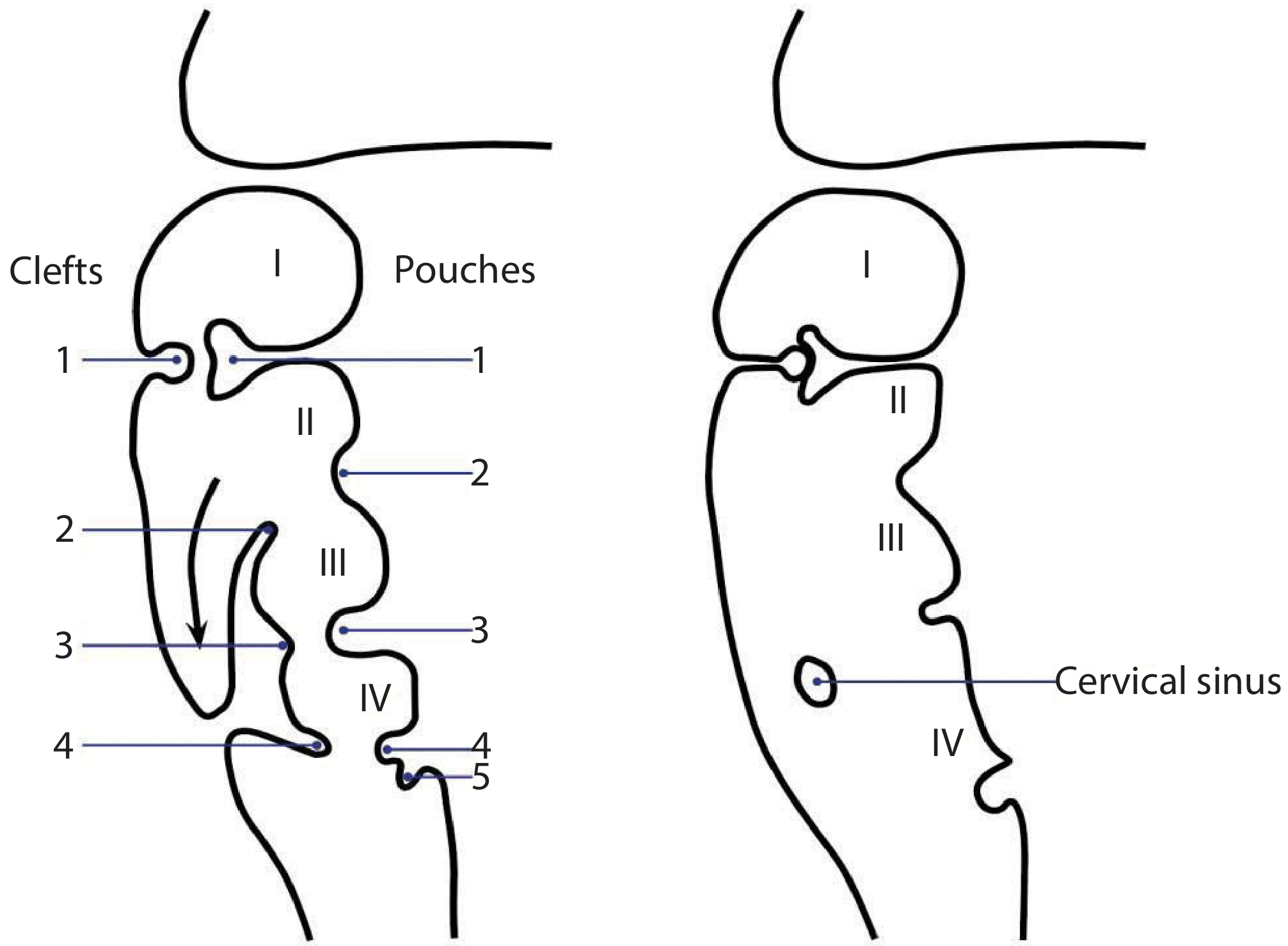
DIAGRAM 2 - Arch Components and Derivatives
DERIVATIVES OF EACH BRANCHIAL ARCH
ARCH 1 - Mandibular Arch
| Component | Derivative |
|---|---|
| Nerve | Trigeminal - mandibular branch (V3) |
| Cartilage (Meckel's) | Maxilla, mandible, malleus, incus, sphenomandibular ligament, anterior malleal ligament |
| Muscles | Muscles of mastication, mylohyoid, anterior belly of digastric, tensor tympani, tensor veli palatini |
| Artery | Maxillary artery (1st aortic arch) |
| Pouch (1st) | Eustachian tube, middle ear cleft, medial surface of tympanic membrane |
| Cleft (1st) | External auditory meatus, lateral surface of tympanic membrane |
ARCH 2 - Hyoid Arch
| Component | Derivative |
|---|---|
| Nerve | Facial nerve (VII) |
| Cartilage (Reichert's) | Stapes superstructure, styloid process, stylohyoid ligament, lesser cornu and upper body of hyoid |
| Muscles | Muscles of facial expression, stapedius, posterior belly of digastric, stylohyoid, platysma |
| Artery | Stapedial artery (2nd aortic arch) |
| Pouch (2nd) | Palatine tonsil |
| Cleft (2nd) | Overgrows and buries clefts 2, 3, 4 to form cervical sinus of His |
ARCH 3
| Component | Derivative |
|---|---|
| Nerve | Glossopharyngeal (IX) |
| Cartilage | Greater cornu and lower body of hyoid |
| Muscles | Stylopharyngeus, superior and middle constrictors |
| Artery | 3rd aortic arch (common carotid arteries) |
| Pouch (3rd) | Inferior parathyroid glands, thymic duct |
ARCH 4
| Component | Derivative |
|---|---|
| Nerve | Vagus - Superior laryngeal nerve |
| Cartilage | Thyroid lamina |
| Muscles | Cricothyroid |
| Artery | 4th aortic arch (arch of aorta on left, right subclavian on right) |
| Pouch (4th) | Superior parathyroid glands |
ARCH 6
| Component | Derivative |
|---|---|
| Nerve | Vagus - Recurrent laryngeal nerve |
| Cartilage | Cricoid, arytenoid cartilages |
| Muscles | Intrinsic muscles of larynx, inferior constrictor |
| Artery | 6th aortic arch (pulmonary arteries; ductus arteriosus on left) |
| Pouch (5th/6th - ultimobranchial body) | Parafollicular C cells of thyroid |
DIAGRAM 3 - Cartilaginous Derivatives
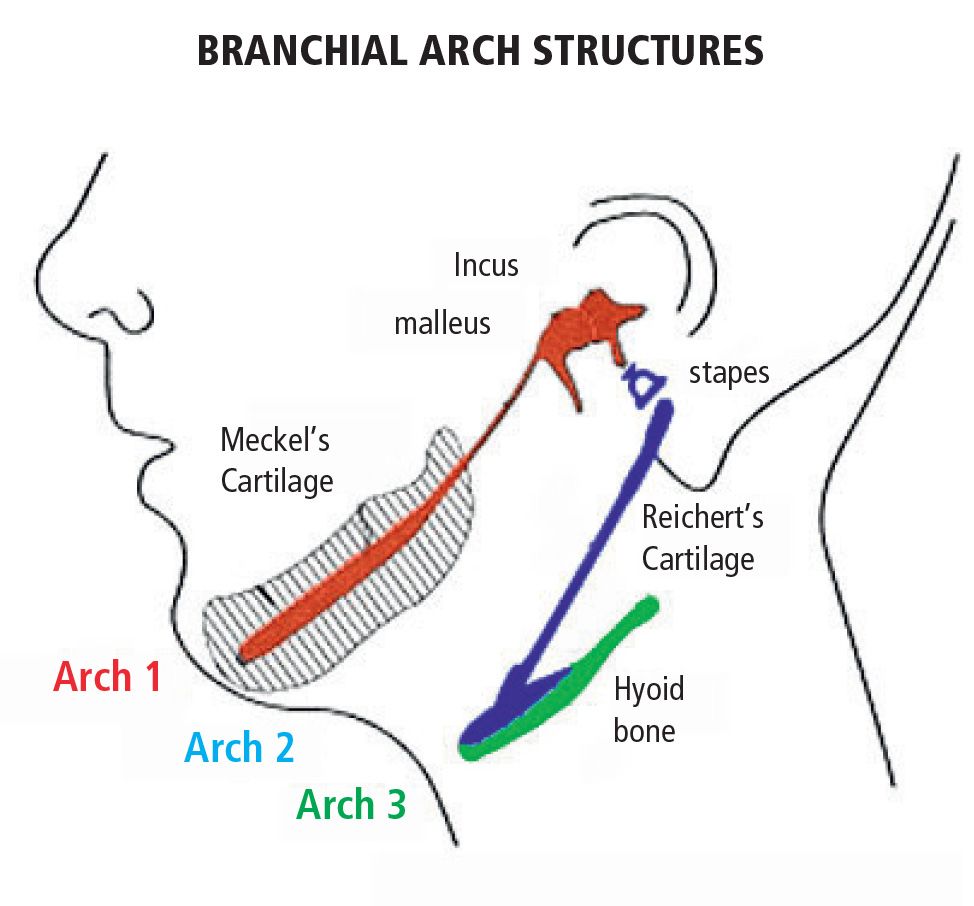
DIAGRAM 4 - Comprehensive Arch/Pouch/Cleft Summary
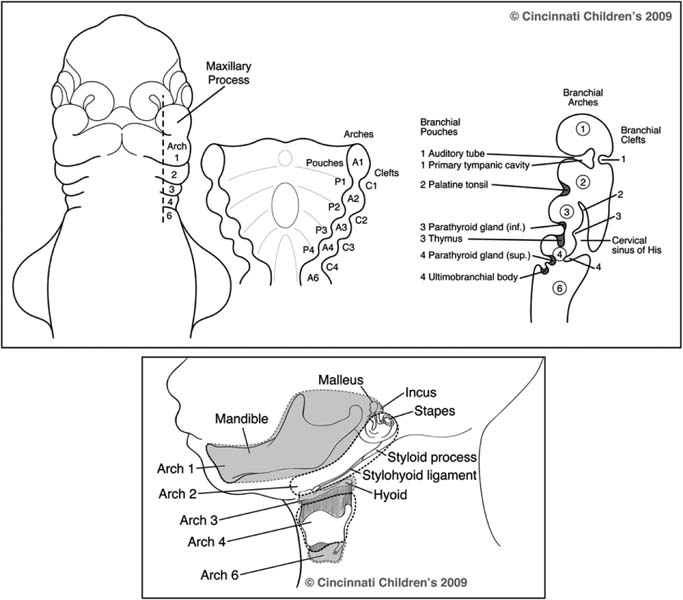
CERVICAL SINUS OF HIS
- The 2nd arch grows caudally over the 3rd, 4th, and 5th clefts, enclosing them in an ectodermal-lined space called the cervical sinus of His
- This sinus normally obliterates completely
- Failure of obliteration is the basis of 2nd, 3rd, and 4th branchial arch anomalies
BRANCHIAL ARCH ANOMALIES
- Cyst - enclosed remnant with no opening
- Sinus - has one opening (internal or external)
- Fistula - has both internal and external openings
"Branchial cleft anomalies are the 2nd most common congenital lesions of the head and neck in children." (Scott-Brown's)
FIRST BRANCHIAL CLEFT ANOMALIES
- Incidence: ~5% of all branchial anomalies
- Classification (Work, 1972):
| Type | Description |
|---|---|
| Type I | Duplication of external auditory canal (ectoderm only). External opening anterior and inferior to tragus. Tract superficial to facial nerve. |
| Type II | Duplication of membranous EAC and pinna (ectoderm + mesoderm). Opening near angle of mandible internally to EAC or conchal bowl. Inconstant relationship with facial nerve - may run deep or superficial. |
- Presentation: Recurrent pre-auricular or periauricular discharge, abscess, skin sinus
- Key danger: Facial nerve (CN VII) is at risk during surgery
- Treatment: Complete surgical excision with CN VII monitoring
SECOND BRANCHIAL CLEFT ANOMALIES
- Most common - approximately 90% of all branchial anomalies
- External opening: Anterior border of sternocleidomastoid muscle (lower third)
- Internal opening: Tonsillar fossa (between pillars)
- Course of tract: Passes between the internal and external carotid arteries, deep to the hypoglossal nerve, superficial to the glossopharyngeal nerve
- Bailey's classification of 2nd arch cysts:
- Type I: Deep to platysma, anterior to SCM
- Type II: Anterior and deep to SCM, adjacent to carotid sheath (most common)
- Type III: Passes between carotid vessels to pharyngeal wall
- Type IV: Adjacent to pharyngeal wall, medial to carotid vessels
- Presentation: Lateral neck mass ± intermittent discharge with URTI
- Treatment: Surgical excision, avoiding carotid vessels and hypoglossal nerve
THIRD BRANCHIAL CLEFT ANOMALIES
- Rare (~2% of anomalies)
- External opening: Anterior border of lower SCM
- Internal opening: Piriform fossa / pyriform sinus (opens into the pharynx just above the upper esophageal sphincter)
- Course: Passes posterior to common carotid artery, deep to glossopharyngeal nerve
- Presentation: Recurrent neck abscess or suppurative thyroiditis (especially left-sided)
- Treatment: Surgical excision; endoscopic cautery of pyriform sinus opening (less invasive alternative)
FOURTH BRANCHIAL CLEFT ANOMALIES
- Very rare
- External opening: Lower anterior SCM
- Internal opening: Apex of piriform fossa, below the superior laryngeal nerve
- Course: Follows recurrent laryngeal nerve, loops around the aorta (left side) or subclavian artery (right side)
- Often presents as recurrent left-sided suppurative thyroiditis
- Distinguishing 3rd from 4th arch anomalies can be difficult clinically
OTHER FIRST AND SECOND ARCH SYNDROMES
- Hemifacial Microsomia (First and Second Arch Syndrome, Lateral Facial Dysplasia): Underdevelopment of structures from arches 1 and 2 - microtia, mandibular hypoplasia, facial asymmetry, hearing loss
- Treacher Collins Syndrome (Mandibulofacial Dysostosis): Autosomal dominant; bilateral hypoplasia of arch 1 derivatives - malar hypoplasia, micrognathia, coloboma of lower eyelid, conductive hearing loss
- Pierre Robin Sequence: Micrognathia, glossoptosis, cleft palate
HILLOCKS OF HIS (Auricular Development)
- External ear develops from 6 mesenchymal hillocks in the 5th week of gestation, fusing at week 12
- Hillocks 1-3 (from arch 1): Tragus, helical crus, helix
- Hillocks 4-6 (from arch 2): Antihelix, antitragus, lobule
- Anomaly: Preauricular sinuses and tags arise from incomplete fusion of hillocks
SUMMARY TABLE - Anomalies at a Glance
| Arch | Incidence | External Opening | Internal Opening | Key Structure at Risk |
|---|---|---|---|---|
| 1st | 5% | Anterior/inferior to tragus | EAC or conchal bowl | Facial nerve (VII) |
| 2nd | 90% | Anterior SCM (lower) | Tonsillar fossa | Internal carotid, hypoglossal nerve |
| 3rd | ~2% | Anterior SCM (lower) | Piriform fossa (superior) | Glossopharyngeal nerve |
| 4th | Rare | Anterior SCM (lower) | Piriform fossa apex | Recurrent laryngeal nerve, aorta |
CLINICAL PEARLS FOR EXAM
- Arch 1 nerve = V (Trigeminal); Arch 2 nerve = VII (Facial) - easiest to confuse, always high-yield
- Meckel's cartilage (Arch 1) → Malleus + Incus; Reichert's cartilage (Arch 2) → Stapes + styloid + lesser hyoid
- Arch 3 pouch → Inferior parathyroid + Thymus (they migrate together and then separate)
- Arch 4 pouch → Superior parathyroid (counterintuitively - arises lower, descends less)
- 2nd branchial cyst is the most common neck anomaly after reactive lymphadenopathy in children
- Work's classification applies to 1st branchial cleft anomalies; Bailey's classification to 2nd arch cysts
- A recurring left-sided thyroid abscess in a child = 3rd or 4th arch fistula until proven otherwise
- The cervical sinus of His = buried clefts 2, 3, 4 by 2nd arch overgrowth; its incomplete obliteration = lateral neck cyst
- Branchial cyst theory controversy: Cervical sinus theory (most accepted) vs. inclusion of skin adnexa theory vs. thymopharyngeal duct theory
Microscopic anatomy of vocal cords and its role in phonation. Ms ent university exam pattern for 20 marks with relevant diagrams.
vocal cord microscopic anatomy lamina propria layers histology phonation diagram
Microscopic Anatomy of the Vocal Cords and Its Role in Phonation
INTRODUCTION
GROSS ORIENTATION
- The true vocal folds lie at the glottic level
- Covered by non-keratinized stratified squamous epithelium on their superior and medial vibratory surfaces (unlike the rest of the larynx, which is covered by pseudostratified ciliated columnar/respiratory epithelium)
- The false (vestibular) folds lie superior to true folds, separated by the laryngeal ventricle; they do not vibrate normally and are covered by respiratory epithelium
DIAGRAM 1 - Five Layers of the Vocal Fold (Hirano's Model)

DIAGRAM 2 - 3D Structural Representation (Cover-Body Model)

MICROSCOPIC LAYERS IN DETAIL
Layer 1: Stratified Squamous Epithelium (0.05 mm)
- Non-keratinized stratified squamous epithelium covers the superior and medial (vibratory) surfaces
- Acts as a protective barrier against mechanical trauma during vibration
- Contains no mucous glands (relies on overlying mucus from the supraglottic mucosa)
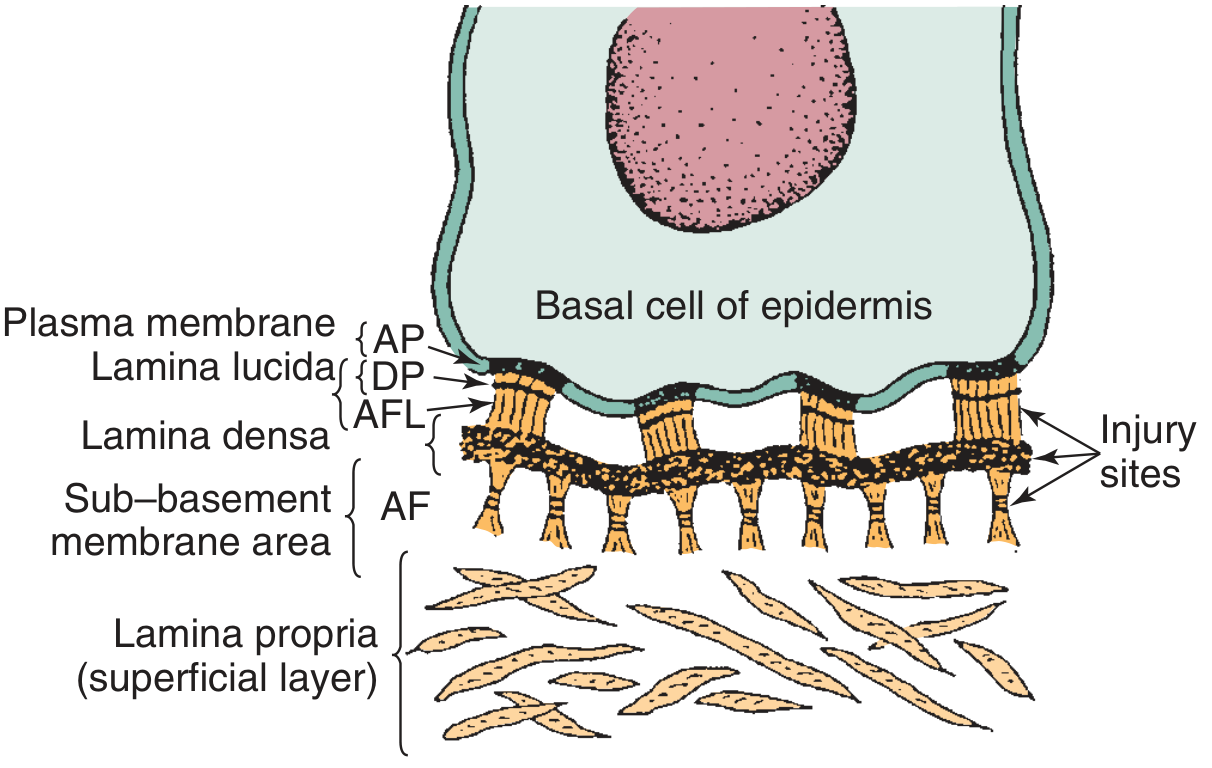
- Anchored to the superficial lamina propria via the basement membrane zone (BMZ)
- The BMZ contains: attachment plaques (AP), lamina lucida, subbasal dense plate (DP), anchoring filaments (AFL), lamina densa, and anchoring fibers (AF) - these allow passive stretch during vibration
DIAGRAM 3 - Basement Membrane Zone (Electron Microscopy)
Layer 2: Lamina Propria - Superficial Layer (SLP) = REINKE'S SPACE (0.3-0.5 mm)
- The most phonatorically critical layer
- Composed of very loose fibrous connective tissue (areolar)
- Rich in hyaluronic acid, water, and fibroblasts producing extracellular matrix proteins
- Contains scattered fibroblasts but virtually no collagen or elastic fibers
- Collagen type III and VII fibers from the deep layer intertwine at the BMZ interface, fixating the BMZ while allowing passive stretch
- This layer allows the overlying epithelium to vibrate freely and independently over the underlying vocal ligament
- Clinical significance: Reinke's edema (polypoid degeneration) occurs here due to fluid/mucinous accumulation, especially from smoking
- Vocal fold nodules cause widening of the BMZ and changes in this layer
Layer 3: Lamina Propria - Intermediate Layer (ILP)
- Denser than SLP
- Rich in elastic fibers running parallel to the long axis of the fold
- Responsible for the elastic recoil properties of the vocal fold
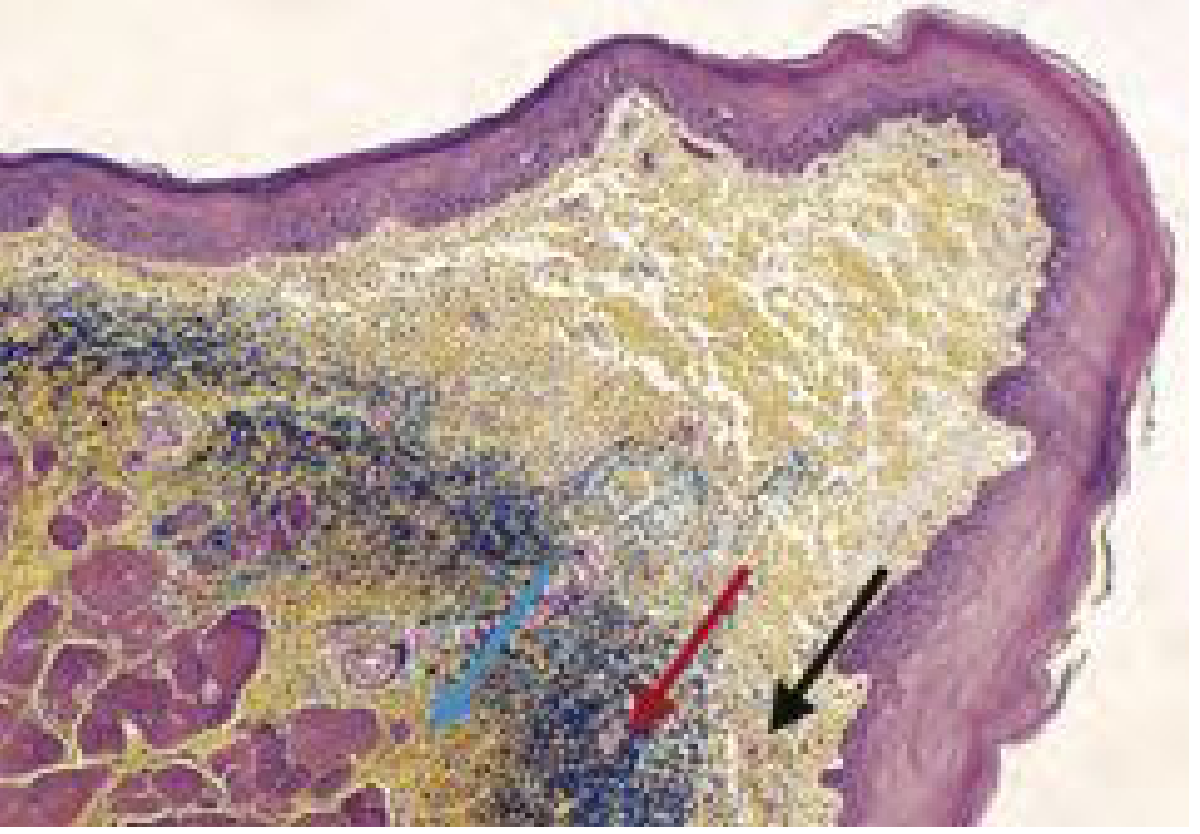
- Appears black on elastin stains (Movat stain)
Layer 4: Lamina Propria - Deep Layer (DLP)
- Densest layer of lamina propria
- Composed primarily of cross-linked collagen fibers (Type I collagen predominantly)
- Progressively denser toward the thyroarytenoid muscle complex
- Appears deep yellow on Movat stain (greater cross-linking than SLP collagen)
- The ILP + DLP together form the vocal ligament (~1 mm thick)
DIAGRAM 4 - Histological Cross-Section (Movat Stain)
Layer 5: Vocalis Muscle (Thyroarytenoid Muscle, Medial Part)
- The bulk of the vocal fold - forms the "body"
- Collagen fibers from the DLP blend directly into the thyroarytenoid muscle
- Two parts:
- Vocalis (medial TA): runs from vocal process of arytenoid to inner thyroid cartilage; fine-tunes tension
- Thyromuscularis (lateral TA): runs to lateral thyroid cartilage
- Functions in pitch control and register changes
- At low pitches: vocalis is relaxed, body participates in oscillation
- At high pitches: vocalis is tense, vibratory motion is confined to the cover
HIRANO'S BODY-COVER MODEL
| Unit | Layer(s) | Properties |
|---|---|---|
| Cover | Epithelium + SLP (Reinke's space) | Pliable, low stiffness, vibrates freely |
| Transition | ILP + DLP (= Vocal Ligament) | Intermediate stiffness |
| Body | Vocalis muscle | Stiff, relatively static during modal phonation |
VASCULAR SUPPLY OF THE VOCAL FOLD
- Blood vessels enter anteriorly and posteriorly
- Run parallel to the longitudinal axis of the fold
- This arrangement allows the cover to vibrate over the body without placing excessive stretch on the vessels
- Arteriovenous shunts are present (electron microscopy) - allow autoregulation of blood flow
- Clinical relevance: vocal fold hemorrhage occurs from rupture of these longitudinal vessels during forceful phonation
PHONATION - MECHANISM
Prerequisites for Phonation (Box 53.1 - Cummings)
- Adequate breath support (subglottic pressure)
- Vibratory edges aligned with an appropriately small glottic gap
- Vocal fold physical properties conducive to vibration
- Favorable 3D contour of the fold
- Volitional control of length, tension, and shape
Theory of Phonation - Myoelastic-Aerodynamic Theory (van den Berg, 1950s)
"The interaction of aerodynamic forces and the mechanical properties of the laryngeal tissues are responsible for inducing vocal fold vibration." - van den Berg
- Glottic closure - Adductor muscles bring the vocal folds to the midline (LCA, IA, lateral cricoarytenoid muscles)
- Subglottic pressure builds - Expiratory airflow from lungs increases subglottic pressure
- Vocal folds blown apart - Pressure exceeds the elastic resistance of the folds; folds are displaced laterally
- Bernoulli effect - Increased airflow velocity through the narrowing glottis creates negative pressure (Bernoulli suction) that pulls the folds back toward midline
- Elastic recoil - The elastic and muscular forces of the fold assist return to midline
- Cycle repeats - The cycle (open phase + closed phase) generates a series of air puffs = the fundamental frequency
The Mucosal Wave
- Begins at the inferomedial aspect of the vocal fold
- Travels rostrally (upward) across the medial edge and superior surface
- Occurs due to a vertical phase shift - the lower lip opens first, then the upper lip; the lower lip closes first, then the upper lip
- In a healthy system at modal conversational pitch, the wave travels across approximately half the width of the superior surface
- Assessed on videostroboscopy (because the wave frequency exceeds the eye's flicker fusion rate)
| Condition | Effect on Mucosal Wave |
|---|---|
| Increased subglottic pressure (loud voice) | Wave travels farther |
| Increased pitch | Wave decreases |
| Falsetto | Wave absent |
| Polypoid degeneration | Increased (abnormally pliable mucosa) |
| Vocal nodules/polyps | Decreased/absent over lesion |
| Scarring/sulcus vocalis | Decreased/absent |
| Stiffness, malignancy | Decreased/absent |
Pitch Control
- Cricothyroid muscle elongates the vocal fold → increases tension → raises pitch (nerve: external branch of SLN)
- Vocalis (medial TA) shortens the fold → lowers pitch
- At high pitch: vocalis contracts, fold is tense and thin, cover is coupled tightly to body, mucosal wave reduced
- At low pitch: vocalis relaxes, body participates in oscillation, large amplitude mucosal wave
Loudness (Intensity) Control
- Determined by subglottic air pressure
- Controlled by expiratory muscles (abdominal muscles, intercostal muscles, diaphragm)
- At conversational levels: passive expiratory recoil is sufficient
- Louder voice: active contraction of abdominal and intercostal muscles
Voice Quality (Timbre)
- The larynx generates a buzz-like fundamental tone plus harmonics (overtones)
- The mucosal wave produces a fundamental tone accompanied by several non-harmonic overtones (K.J. Lee)
- Sound is modified by: volume of airflow, movements of the vocal tract, and degree of vocal cord tension
- Articulation and resonance in the supraglottic vocal tract (pharynx, oral cavity, nasal cavity) shape sound into recognizable speech
DIAGRAM 5 - Histological Section of Vocal Fold

AGING CHANGES
- Voice fundamental frequency increases in aging men (due to vocal fold atrophy and bowing) but decreases in aging women (due to decreased estrogen and relative androgenic effect)
- SLP loses hyaluronic acid → decreased pliability → decreased mucosal wave
- Vocalis atrophies → vocal fold bowing → incomplete glottal closure → breathy, weak voice (presbylaryngis/presbyphonia)
CLINICAL CORRELATIONS
| Pathology | Layer Affected | Phonatory Effect |
|---|---|---|
| Reinke's edema | SLP (Reinke's space) | Low, rough, husky voice |
| Vocal nodules | BMZ / SLP interface | Decreased mucosal wave, breathy dysphonia |
| Vocal polyp | SLP (hemorrhagic/edematous) | Unilateral decreased mucosal wave |
| Sulcus vocalis | SLP (pit/furrow to ligament) | Very stiff fold, absent mucosal wave |
| Vocal fold scar | All layers of LP | Absent mucosal wave, dysphonia |
| Laryngeal cancer | All layers → muscle | Absent mucosal wave, fixation |
| Vocal fold paralysis | Innervation (RLN) | Absent/reduced closure, breathy voice |
SUMMARY TABLE - Hirano's Five Layers at a Glance
| Layer | Thickness | Composition | Mechanical Property | Clinical Name |
|---|---|---|---|---|
| Epithelium | 0.05 mm | Non-keratinized squamous | Stiff barrier | - |
| SLP | 0.3-0.5 mm | Loose ECM, hyaluronic acid | Very pliable | Reinke's space |
| ILP | - | Elastic fibers | Elastic | Part of Vocal Ligament |
| DLP | - | Collagen fibers | Stiff | Part of Vocal Ligament |
| Vocalis | - | Striated muscle (TA) | Variable (active) | Body |
CLINICAL PEARLS FOR EXAM
- Hirano's 5-layer model (1974-77) is the basis of all vocal fold surgery and voice science
- Reinke's space (SLP) is the most important layer for phonation - its pliability enables the mucosal wave
- Mucosal wave is assessed on videostroboscopy - if absent, think stiffness, scarring, or cancer
- The Bernoulli effect + elastic recoil = myoelastic-aerodynamic theory of phonation
- Vertical phase shift (lower lip opens/closes first) is what generates the mucosal wave
- Cricothyroid muscle = pitch raiser; vocalis = pitch lowerer
- True vocal folds have non-keratinized squamous epithelium; rest of larynx = respiratory (ciliated columnar) epithelium
- Vocal fold has no mucous glands on its free edge - relies on overlying laryngeal secretions
- BMZ is the site of shearing forces - its disruption leads to nodule and polyp formation
- Loudness = subglottic pressure; Pitch = vocal fold tension/length; Quality = supraglottic resonance
Anatomy of oesophagus. Ms ent university exam pattern for 20 marks.
oesophagus anatomy ENT constrictions layers blood supply nerve supply diagram
Anatomy of the Oesophagus
INTRODUCTION
DIAGRAM 1 - Overview of Oesophagus: Segments, Constrictions, and Distances from Incisors

COURSE AND DEVIATIONS
- In the neck: gradually veers left until the root of the neck, then returns to midline
- At T5: veers left again, then reverts to midline
- At T7: veers left once more, continuing in this course through the oesophageal hiatus
SUBDIVISIONS
| Segment | Extent | Vertebral Level |
|---|---|---|
| Cervical | Inferior border of cricoid to thoracic inlet | C6 - T1 |
| Thoracic | Thoracic inlet to oesophageal hiatus | T1 - T10 |
| Abdominal | Oesophageal hiatus to gastroesophageal junction | T10 - T11 (~1.25-2 cm long) |
ANATOMICAL RELATIONS
Cervical Oesophagus
- Anterior: Trachea (adherent via loose connective tissue)
- Posterior: Bodies of C6 and C7 vertebrae, prevertebral fascia, longus colli muscle
- Lateral: Common carotid arteries (bilaterally), lower poles of thyroid gland
- Left lateral: Thoracic duct (ascending briefly)
- In the tracheo-oesophageal grooves bilaterally: Recurrent laryngeal nerves pass superiorly to enter the larynx behind the cricothyroid joint
- Position: Generally slightly to the left of midline at thyroid gland level
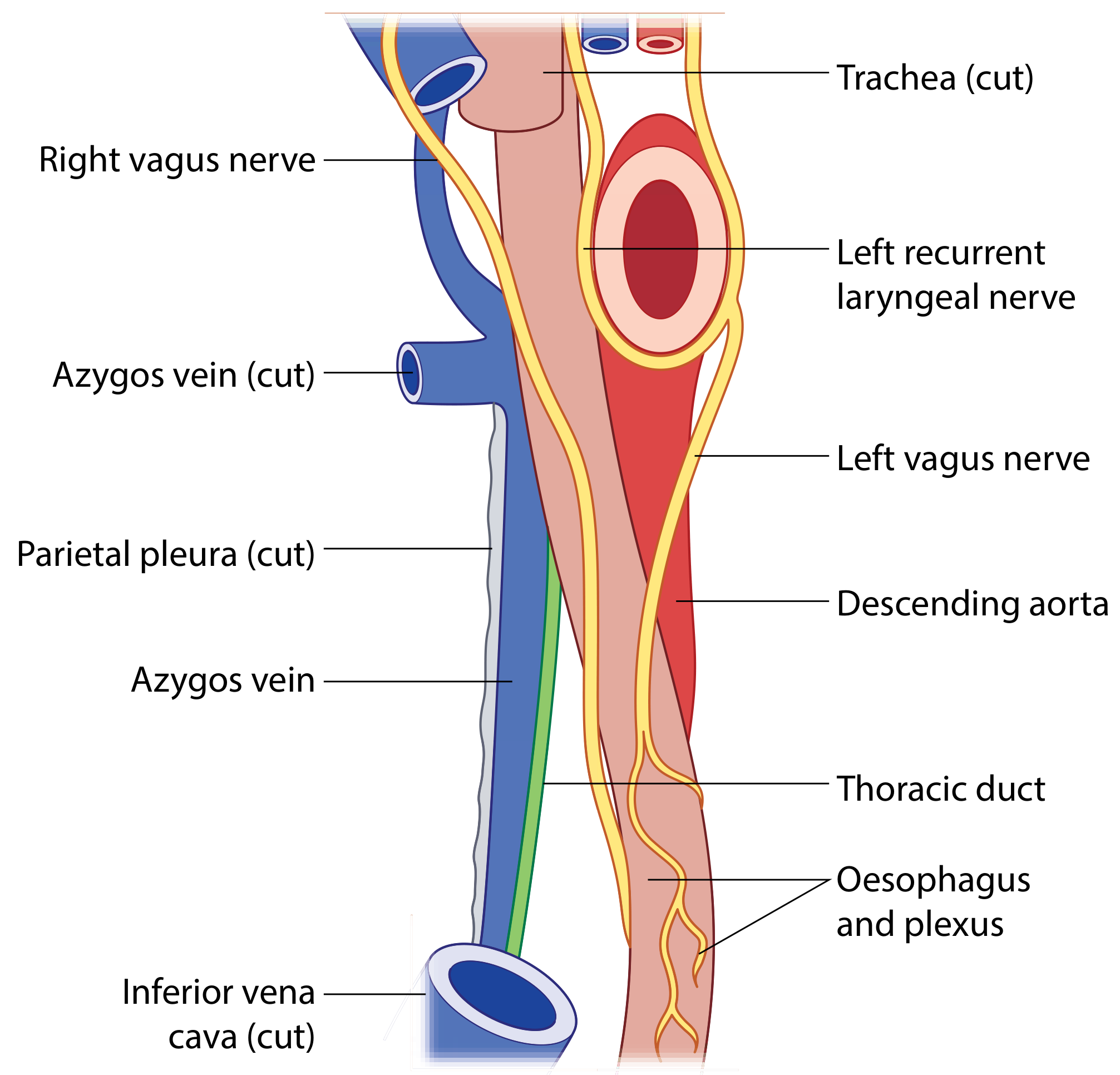
Thoracic Oesophagus
- Trachea
- Left recurrent laryngeal nerve
- Terminal part of aortic arch
- Left subclavian vein
- Thoracic duct
- Left recurrent laryngeal nerve
- Left pleura
- Left main bronchus
- Tracheobronchial lymph nodes
- Pericardium
- Left atrium (important: oesophageal tumours can cause AF by compressing left atrium)
- Vertebral bodies T1-T4
- Thoracic duct (sandwiched between azygos vein and descending aorta)
- Right posterior intercostal arteries
- Hemiazygos and accessory azygos veins
- At terminal thoracic part: descending aorta lies between oesophagus and vertebrae
DIAGRAM 2 - Intrathoracic Relations of the Oesophagus
CONSTRICTIONS OF THE OESOPHAGUS
| Constriction | Cause | Distance from Upper Incisors | Vertebral Level |
|---|---|---|---|
| 1st (Cricopharyngeal/UES) | Cricopharyngeus muscle / inferior border of cricoid | 15 cm | C6 |
| 2nd (Aortic) | Arch of aorta crossing anteriorly | 22-25 cm | T4 |
| 3rd (Bronchial) | Left main bronchus crossing anteriorly | 27 cm | T5 |
| 4th (Diaphragmatic/LES) | Oesophageal hiatus of diaphragm | 38-40 cm | T10 |
Note: The 2nd and 3rd constrictions (aortic and bronchial) are often grouped together as the "bronchoaortic" constriction.
- Foreign bodies most commonly lodge at the cricopharyngeal constriction (15 cm)
- Site of false passage formation during rigid oesophagoscopy if proper technique is not followed
- Site of maximum resistance during food bolus propulsion
LAYERS OF THE OESOPHAGEAL WALL
Diagram 3 - Wall Layers and Innervation
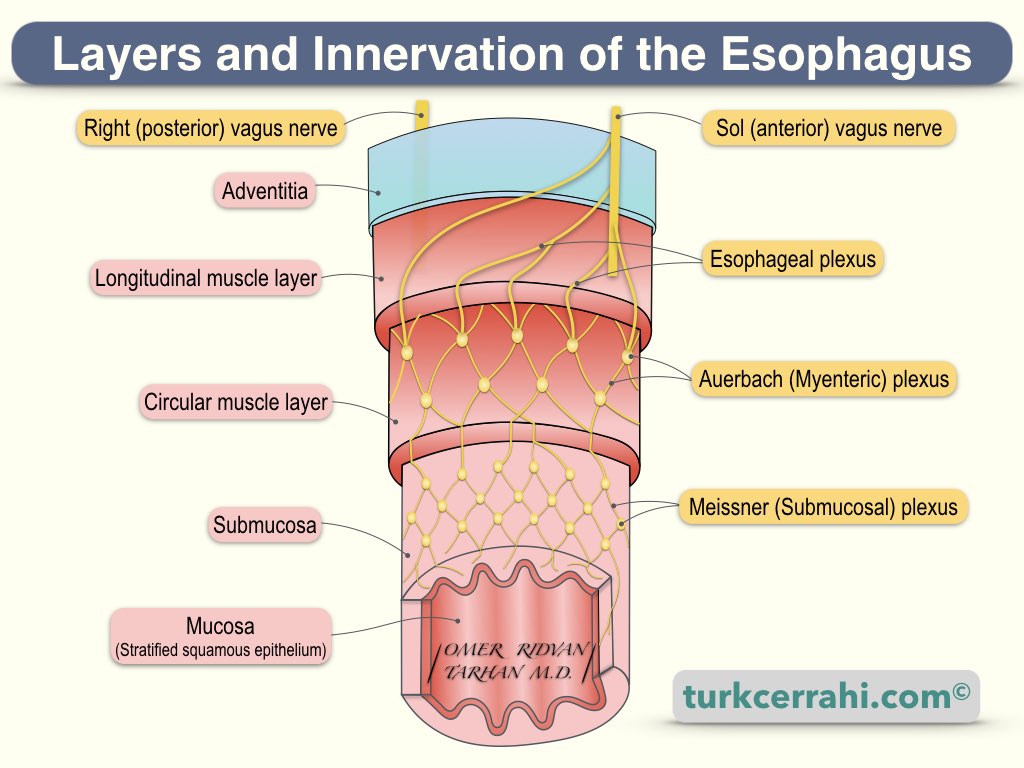
1. Adventitia (Fibrous Coat)
- Outermost layer
- Dense connective tissue
- No serosa - this means oesophageal perforation leads directly to mediastinitis without the protective buffer of serosa, and oesophageal carcinoma can spread directly to mediastinal structures
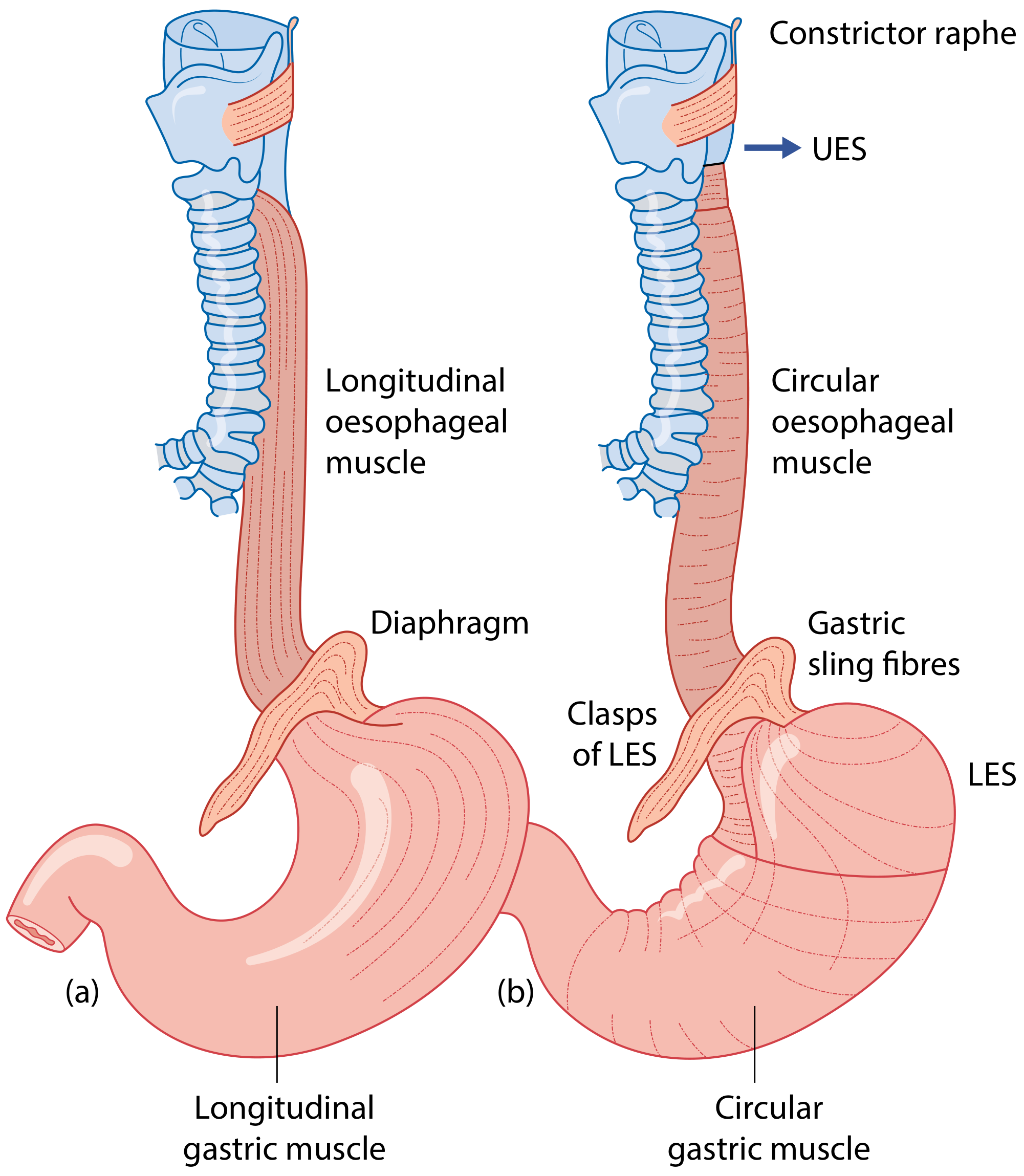
2. Muscularis Externa (Muscle Coat)
- Originates from the posterior surface of the cricoid cartilage via two muscular slips
- The V-shaped gap between these two slips at the back = Laimer's triangle (a weak spot posterior to the oesophagus)
- Pharyngo-oesophageal junction muscle arrangements include Killian's dehiscence (Killian's triangle) - a weak point between the oblique fibres of the thyropharyngeus and the horizontal fibres of cricopharyngeus, where pharyngeal pouch (Zenker's diverticulum) protrudes
- The upper (cricopharyngeal) part = Upper Oesophageal Sphincter (UES) - striated muscle, under voluntary control
- The lower circular fibres at gastroesophageal junction = Lower Oesophageal Sphincter (LES) - smooth muscle, physiological sphincter
| Region | Muscle Type |
|---|---|
| Upper 1/3 | Striated (voluntary) |
| Middle 1/3 | Mixed striated and smooth |
| Lower 1/3 | Smooth (involuntary) |
Diagram 4 - Muscles of the Oesophagus

Diagram 5 - Longitudinal and Circular Muscle Arrangement with Sphincters
3. Submucosa
- Contains:
- Mucous glands (oesophageal glands proper) - provide lubrication
- Rich submucosal venous plexus (important in portal hypertension/varices)
- Extensive submucosal lymphatic channels (accounts for "skip" metastasis in oesophageal cancer)
- Meissner's plexus (submucosal/secretomotor plexus)
4. Mucosa
- Non-keratinized stratified squamous epithelium throughout most of the oesophagus
- Contains a muscularis mucosae (inner smooth muscle of the mucosal layer)
- At the gastro-oesophageal junction, squamous epithelium transitions to columnar gastric epithelium - the Z-line (squamo-columnar junction)
- Barrett's oesophagus: pathological columnar metaplasia of the lower oesophageal mucosa due to chronic acid reflux
BLOOD SUPPLY
Arterial Supply (Segmental Pattern)
| Segment | Arterial Supply |
|---|---|
| Cervical | Inferior thyroid artery (from thyrocervical trunk) |
| Thoracic | ~5 oesophageal branches from descending aorta directly; also bronchial arteries |
| Abdominal | Left gastric artery, left inferior phrenic artery |
- The aortic oesophageal branches form a vascular chain on the oesophagus itself
- This chain anastomoses superiorly with inferior thyroid branches and inferiorly with left gastric/phrenic branches
- This dense anastomotic supply renders the oesophagus virtually immune to ischaemic infarction
Venous Drainage (Porto-Systemic Significance)
| Segment | Venous Drainage | System |
|---|---|---|
| Cervical | Inferior thyroid veins → brachiocephalic veins | Systemic |
| Thoracic | Azygos veins, hemiazygos, intercostal veins, bronchial veins | Systemic |
| Abdominal | Left gastric vein → portal vein | Portal |
- Venous blood first drains into a submucosal venous plexus, then into a perioesophageal venous plexus
- The junction between portal (left gastric vein) and systemic (oesophageal veins) occurs at the level of T8 (central diaphragmatic tendon)
- Portal hypertension → back-pressure → dilated submucosal oesophageal veins = oesophageal varices - prone to life-threatening haemorrhage
NERVE SUPPLY
Extrinsic Innervation
| Component | Supply |
|---|---|
| Upper striated muscle (upper 1/3) | Recurrent laryngeal nerves (small branches); postganglionic sympathetics from middle cervical ganglion via inferior thyroid arteries |
| Lower smooth muscle (lower 2/3) | Oesophageal plexus - formed by left and right vagus nerves and their branches covering the oesophagus |
| Sympathetic (T1-T10) | Regulates smooth muscle activity and glandular secretion |
- Left and right vagus nerves form the oesophageal plexus covering the thoracic oesophagus
- The vagal trunks re-form below the plexus:
- Left vagus → anterior vagal trunk (at oesophageal hiatus)
- Right vagus → posterior vagal trunk (at oesophageal hiatus)
Intrinsic (Enteric) Innervation
| Plexus | Location | Function |
|---|---|---|
| Auerbach's plexus (myenteric) | Between longitudinal and circular muscle layers | Controls peristaltic contraction of outer muscle layers |
| Meissner's plexus (submucosal) | In the submucosa | Controls secretion and peristaltic contractions of muscularis mucosae |
| The two are interconnected by a network of fibres |
- Pain perception in the oesophagus is limited - more from stretching of the external muscular coat than mucosal awareness
- Referred pain is common (explains why oesophageal pain mimics cardiac pain)
LYMPHATIC DRAINAGE
| Segment | Drains To |
|---|---|
| Upper oesophagus | Lower deep cervical nodes, paratracheal nodes, upper mediastinal nodes |
| Thoracic oesophagus | Posterior mediastinal nodes, tracheobronchial nodes |
| Abdominal oesophagus | Left gastric nodes, coeliac nodes |
| Any level | Some lymph may pass directly into the thoracic duct |
- An extensive submucosal lymphatic network runs longitudinally within the oesophageal wall
- Lymph can travel along the length of the oesophagus before exiting to regional nodes
- This explains "skip" metastases in oesophageal cancer, where nodes far from the primary tumour are involved
SPHINCTERS
Upper Oesophageal Sphincter (UES)
- Formed mainly by cricopharyngeus muscle (part of inferior constrictor)
- Striated muscle - under voluntary and reflex control
- Normally closed at rest (prevents air entering oesophagus during respiration)
- Relaxes during swallowing
- Cricopharyngeal dysfunction → pharyngeal pouch (Zenker's diverticulum)
Lower Oesophageal Sphincter (LES)
- Physiological sphincter (no distinct anatomical sphincter, but functionally maintained by circular smooth muscle)
- Located at gastro-oesophageal junction (T10-T11)
- Maintained by: intrinsic smooth muscle tone, right crus of diaphragm (external pinch-cock), intra-abdominal pressure
- Prevents gastric reflux into oesophagus
- LES incompetence → Gastro-oesophageal reflux disease (GORD)
PHARYNGO-OESOPHAGEAL JUNCTION - WEAK AREAS
-
Killian's dehiscence (Killian's triangle) - between oblique thyropharyngeus fibres and horizontal cricopharyngeus fibres. Site of Zenker's (pharyngeal) diverticulum formation
-
Laimer's triangle - V-shaped gap between the two slips of origin of the longitudinal muscle from cricoid. Site of posterior oesophageal perforation risk
SUMMARY TABLE - Key ENT Facts
| Feature | Detail |
|---|---|
| Length | 25 cm |
| Begins | C6 / 15 cm from incisors |
| Ends | T11 |
| Hiatus | T10 |
| Narrowest point | Cricopharyngeal sphincter (15 cm) |
| No serosa | Spreads early; perforation = mediastinitis |
| Porto-systemic junction | T8 - submucosal venous plexus (varices) |
| Foreign body | Usually at 1st constriction (15 cm) |
| Mucosa | Stratified squamous (non-keratinized) |
| Upper 1/3 muscle | Striated (voluntary) |
| Lower 1/3 muscle | Smooth (involuntary) |
| Skip metastasis | Due to submucosal lymphatic channels |
CLINICAL PEARLS FOR EXAM
- No serosa = oesophageal cancer spreads early to adjacent structures and surgery is difficult
- Cricopharyngeal constriction at 15 cm = most common site for foreign body impaction
- Killian's triangle = Zenker's diverticulum; Laimer's triangle = risk of posterior wall perforation
- Left atrium is an anterior relation of thoracic oesophagus - left atrial enlargement causes dysphagia (dysphagia lusoria from posterior compression)
- Portal hypertension → oesophageal varices at T8 porto-systemic anastomosis - life-threatening haemorrhage
- RLN runs in tracheo-oesophageal groove - at risk in oesophageal/thyroid surgery
- Upper 1/3 striated muscle → voluntary deglutition; lower 2/3 smooth muscle → peristalsis via vagus
- Barrett's oesophagus = columnar metaplasia at lower end due to chronic GORD - pre-malignant
- Submucosal lymphatics run longitudinally → "skip" lesions in oesophageal carcinoma
- Distance of constrictions from incisors: 15-25-27-40 cm (or by rule of 15: 15, 25, 40)
Anatomy of pharynx and para pharyngeal space. Ms ent university exam pattern for 20 marks.
pharynx anatomy parapharyngeal space diagram ENT layers muscles
Anatomy of the Pharynx and Parapharyngeal Space
INTRODUCTION
DIAGRAM 1 - Pharynx: Posterior View Showing Three Subdivisions
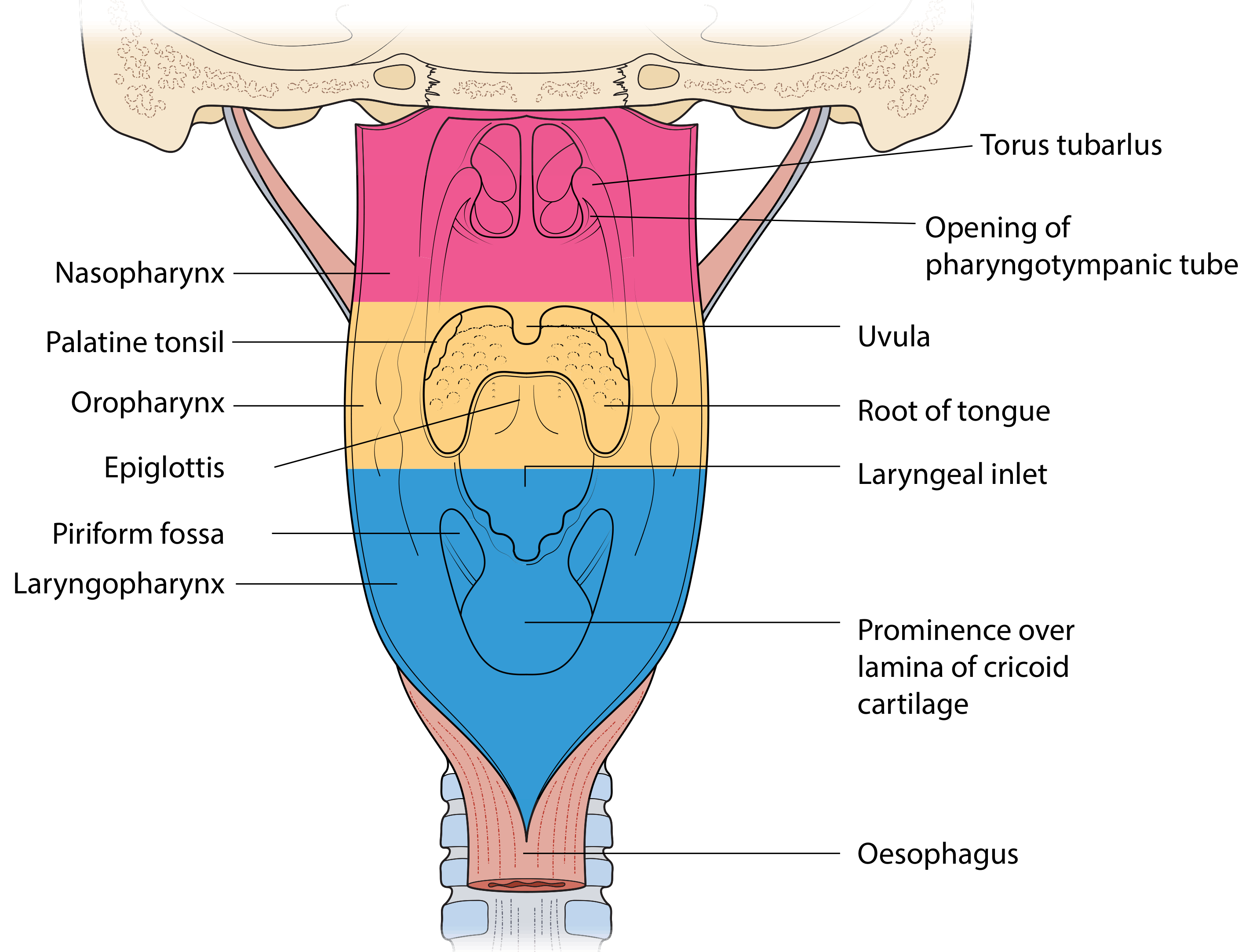
SUBDIVISIONS OF THE PHARYNX
| Subdivision | Superior Limit | Inferior Limit |
|---|---|---|
| Nasopharynx | Skull base / pharyngeal tubercle | Soft palate (level of hard-soft palate junction) |
| Oropharynx | Hard-soft palate junction | Plane of hyoid bone / floor of valleculae |
| Hypopharynx (Laryngopharynx) | Level of hyoid bone (pharyngoepiglottic folds) | Inferior border of cricoid cartilage (C6) |
NASOPHARYNX
- Roof/Posterior wall: Sloping surface of the sphenoid and occipital bones, continues with the posterior wall down to the level of the hard palate (one continuous surface)
- Floor: Upper surface of the soft palate
- Lateral walls: Contain the opening of the auditory (Eustachian) tube - surrounded by a raised cartilaginous rim - the torus tubarius
- Posterior to the torus tubarius: The deep fossa of Rosenmuller (pharyngeal recess) - the most common site of nasopharyngeal carcinoma (NPC)
- Anterior wall: Choanae (posterior nasal apertures)
- Pharyngeal tonsil (Adenoid): Lymphoid tissue in the roof and posterior wall; enlarges in children, involutes after puberty
- Opening of the auditory tube: On the lateral wall, ~1 cm behind the inferior turbinate; allows pressure equalization of the middle ear
- Salpingopharyngeal fold: Fold of mucosa hanging from the torus tubarius containing salpingopharyngeus muscle
- Passavant's ridge: A transverse muscular ridge on the posterior wall formed during deglutition by contraction of upper fibres of the superior constrictor; assists in velopharyngeal closure
OROPHARYNX
- Superior: Soft palate (horizontal plane at hard-soft palate junction)
- Inferior: Plane through the floor of the valleculae (level of hyoid bone)
- Anterior: Oropharyngeal isthmus (between palatoglossal folds) - includes posterior 1/3 of tongue
- Base of tongue (posterior 1/3) and valleculae (anterior wall)
- Lateral walls: Palatine tonsils, tonsillar fossae, tonsillar (faucial) pillars (anterior = palatoglossal fold; posterior = palatopharyngeal fold), glossotonsillar sulci
- Superior wall: Inferior surface of soft palate and uvula
- Posterior wall: Posterior pharyngeal wall
- The soft palate acts as a "flutter valve" - elevation closes the pharyngeal isthmus (preventing food regurgitation into nasopharynx); depression closes the oral isthmus
- The soft palate contains 5 muscles: levator veli palatini, tensor veli palatini, palatoglossus, palatopharyngeus, and musculus uvulae
- Waldeyer's ring: The ring of lymphoid tissue formed by pharyngeal tonsil (adenoids), tubal tonsils, palatine tonsils, and lingual tonsil
HYPOPHARYNX (LARYNGOPHARYNX)
- Superior: Level of hyoid bone (pharyngoepiglottic folds)
- Inferior: Inferior border of cricoid cartilage - becomes the oesophagus
- Anterior: Posterior surface of the larynx
- Pyriform fossa (sinus) - Bilateral recesses on either side of the laryngeal inlet; bounded medially by the aryepiglottic folds, anteriorly/laterally by the thyroid cartilage and thyrohyoid membrane, apex at the level of the cricoid cartilage. Common site for foreign body lodgement and for hypopharyngeal carcinoma (silent expansion before late presentation)
- Posterior pharyngeal wall - From the level of the superior hyoid to the inferior cricoid
- Postcricoid region - Anterior wall of the hypopharynx, inferior to the arytenoids to the inferior margin of the cricoid; contiguous medially with the pyriform sinuses
LAYERS OF THE PHARYNGEAL WALL
| Layer | Details |
|---|---|
| 1. Mucous membrane | Stratified squamous epithelium in oro/hypopharynx; pseudostratified ciliated columnar (respiratory) in nasopharynx |
| 2. Submucosa | Contains mucous glands, lymphatics, blood vessels |
| 3. Pharyngobasilar fascia | Thick fibrous sheet; fills the gap above the superior constrictor muscle, attaches to skull base at pharyngeal tubercle; forms the rigid framework of the nasopharynx |
| 4. Muscular layer | Outer circular constrictors + inner longitudinal dilators |
| 5. Buccopharyngeal fascia | Thin layer of loose areolar tissue on the outer surface (epimysial layer of the constrictors) |
MUSCLES OF THE PHARYNX
Diagram 2 - Pharyngeal Muscles
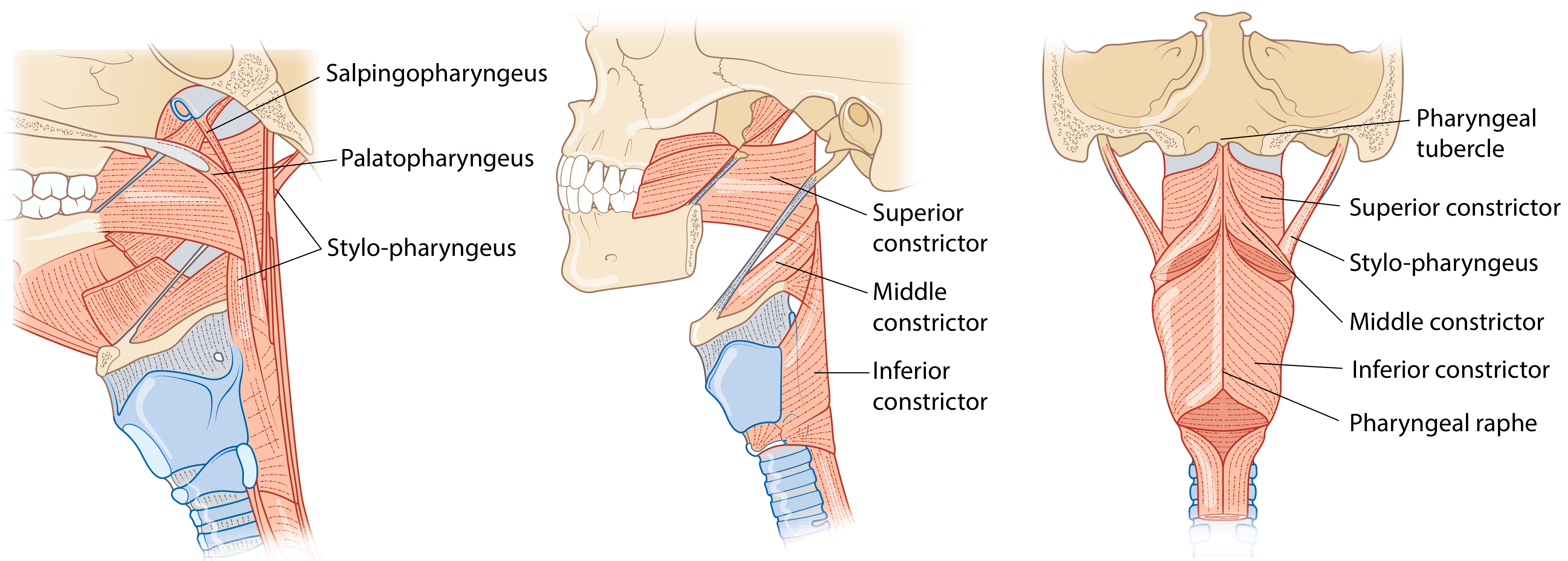
A. OUTER CIRCULAR LAYER - Three Constrictor Muscles
| Muscle | Origin | Key Relations |
|---|---|---|
| Superior constrictor | 4-part origin: pterygoid hamulus (pterygopharyngeal), pterygomandibular raphe (buccopharyngeal), posterior alveolar process of mandible (mylopharyngeal), lateral tongue (glossopharyngeal) | Gap above = nasopharynx (pharyngobasilar fascia fills it); gap between superior and middle = stylopharyngeus, glossopharyngeal nerve, styloglossus, lingual nerve pass through |
| Middle constrictor | Fan-shaped; greater and lesser horns of hyoid, lower end of stylohyoid ligament | Overlaps superior constrictor above; gap with inferior constrictor covered by thyrohyoid membrane (through which internal laryngeal nerve and superior laryngeal vessels pass) |
| Inferior constrictor | Two parts: thyropharyngeus (oblique line of thyroid lamina) + cricopharyngeus (cricoid cartilage = UES) | Cricopharyngeus = upper oesophageal sphincter; horizontal fibres do not overlap - this creates Killian's dehiscence posteriorly |
B. INNER LONGITUDINAL LAYER - Three Dilator/Elevator Muscles
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Stylopharyngeus | Medial base of styloid process | Posterosuperior border of thyroid cartilage; merges with palatopharyngeus | Elevates pharynx and larynx; assists peristaltic bolus movement | Glossopharyngeal (CN IX) - the only pharyngeal muscle supplied by CN IX |
| Palatopharyngeus | Hard palate, palatine aponeurosis (2 heads, separated by levator veli palatini) | Posterior border of thyroid cartilage; blends with superior constrictor | Elevates larynx; closes nasopharynx; forms posterior tonsillar pillar | Pharyngeal plexus |
| Salpingopharyngeus | Inferior end of the cartilaginous Eustachian tube (torus tubarius) | Blends with palatopharyngeus | Elevates pharynx; opens Eustachian tube during swallowing | Pharyngeal plexus |
BLOOD SUPPLY
| Segment | Arterial Supply |
|---|---|
| Nasopharynx | Ascending pharyngeal artery (branch of external carotid), maxillary artery branches |
| Oropharynx | Ascending pharyngeal artery, tonsillar branch of facial artery, ascending palatine artery |
| Hypopharynx | Superior and inferior thyroid arteries, ascending pharyngeal artery |
NERVE SUPPLY
Pharyngeal Plexus (the key concept)
- Glossopharyngeal nerve (CN IX) - sensory to pharyngeal mucosa
- Vagus nerve (CN X) - motor to all pharyngeal muscles (via pharyngeal branch)
- Sympathetic fibres from superior cervical ganglion (via external carotid artery)
| Function | Nerve |
|---|---|
| Motor to all constrictors | Vagus (CN X) via pharyngeal plexus |
| Motor to stylopharyngeus only | Glossopharyngeal (CN IX) |
| Sensory to nasopharynx | Maxillary nerve (CN V2) |
| Sensory to oropharynx + tonsil | Glossopharyngeal (CN IX) |
| Sensory to hypopharynx/laryngopharynx | Internal branch of superior laryngeal nerve (CN X) |
LYMPHATICS
- Nasopharynx → Retropharyngeal nodes → then to upper deep cervical nodes (Level II); also direct drainage to the jugulodigastric (Rouviere's) node - important in NPC
- Oropharynx (tonsil, base of tongue) → Jugulodigastric and upper/mid deep cervical nodes
- Hypopharynx → Mid and lower deep cervical nodes, paratracheal nodes
PARAPHARYNGEAL SPACE
Introduction and Importance
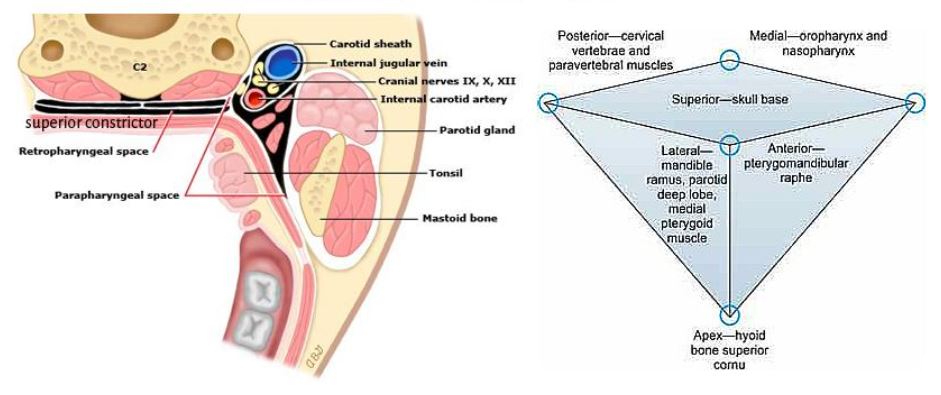
DIAGRAM 3 - Parapharyngeal Space: Axial Section
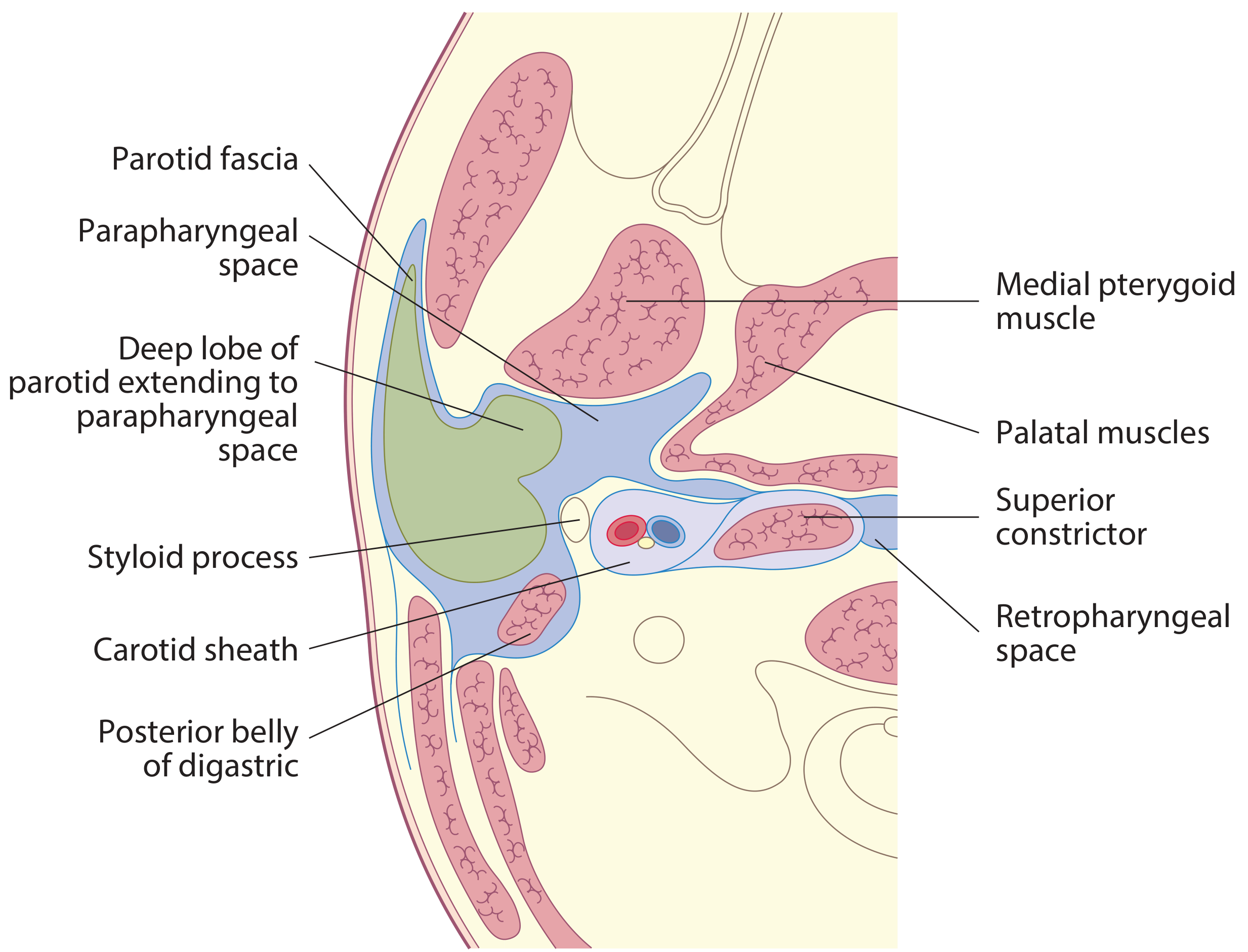
DIAGRAM 4 - Parapharyngeal Space: 3D Shape, Boundaries and Contents
SHAPE AND EXTENT
- Shape: Inverted pyramid (inverted cone)
- Apex: Level of the hyoid bone (greater cornu)
- Base: Petrous temporal bone (skull base)
- Length: Skull base to hyoid bone (~6 cm)
BOUNDARIES
| Wall | Boundary |
|---|---|
| Medial | Superior constrictor muscle (+ buccopharyngeal fascia); separates PPS from the pharynx and tonsil |
| Lateral | Mandibular ramus, medial pterygoid muscle, parotid gland (deep lobe), parotid fascia |
| Anterior | Pterygomandibular raphe; medial pterygoid muscle |
| Posterior | Cervical vertebrae (C1-C3), paravertebral muscles, prevertebral fascia |
| Superior (base) | Petrous temporal bone, tensor veli palatini, levator veli palatini muscles |
| Apex | Greater cornu of hyoid bone |
DIVISION BY STYLOID PROCESS
PRE-STYLOID COMPARTMENT (Anterior Compartment)
- Fat and loose connective tissue (the parapharyngeal fat pad - key radiological landmark)
- Deep lobe of the parotid gland (connected to superficial lobe through stylomandibular tunnel)
- Maxillary artery (internal maxillary artery)
- Branches of CN V3: Inferior alveolar nerve, lingual nerve, auriculotemporal nerve
- Ascending pharyngeal artery (variable)
- Lymph nodes
POST-STYLOID COMPARTMENT (Posterior Compartment = Carotid Space)
- Carotid sheath and its contents:
- Internal carotid artery
- Internal jugular vein
- Vagus nerve (CN X)
- Cranial nerves IX (glossopharyngeal), XI (accessory), XII (hypoglossal)
- Sympathetic chain (cervical sympathetic trunk)
- Lymph nodes
- CN X (vagus) - within carotid sheath
DIAGRAM 5 - Deep Neck Spaces in Relation to Pharynx

COMMUNICATIONS OF THE PARAPHARYNGEAL SPACE
| Space | Communication |
|---|---|
| Retropharyngeal space | Posteriorly (the two PPS spaces communicate via the retropharyngeal space) |
| Submandibular space | Anteroinferiorly (around the stylomandibular ligament) |
| Masticator space | Anteriorly (around pterygomandibular raphe) |
| Parotid space | Laterally (via stylomandibular tunnel, through which deep parotid lobe extends) |
| Posterior cervical space | Posteriorly |
| Carotid space | Is the post-styloid compartment itself |
CLINICAL SIGNIFICANCE
1. Parapharyngeal Neoplasms
- 80% are benign, 20% malignant
- Pre-styloid lesions: Most commonly arise from the deep lobe of the parotid (pleomorphic adenoma)
- Displace the carotid sheath and fat pad posteriorly and medially
- Post-styloid lesions: Commonly of neuroendocrine origin:
- Carotid body paraganglioma, vagal schwannoma, sympathetic chain neuromas
- Displace the parapharyngeal fat pad anteriorly
- Radiological displacement of the parapharyngeal fat pad is key to localizing the lesion to pre- or post-styloid compartment
- Surgical access may require: transcervical approach, transoral approach, or mandibulotomy (lip-split)
2. Parapharyngeal Space Abscess
- Sources: Peritonsillar abscess (most common), submandibular space infection (dental causes), parotid suppuration, retropharyngeal abscess
- Features:
- Medial displacement of the tonsil and lateral oropharyngeal wall
- Bulge of lateral pharyngeal wall visible on examination
- Trismus (due to medial pterygoid muscle inflammation)
- Neck swelling may be absent
- Airway compromise - can be life-threatening
- Danger: Direct spread into retropharyngeal space → posterior mediastinitis; erosion of carotid artery → life-threatening haemorrhage; jugular vein thrombosis (Lemierre's syndrome)
RETROPHARYNGEAL SPACE (Adjacent Important Space)
- Location: Between the pharynx (middle layer of deep cervical fascia anteriorly) and the alar fascia posteriorly
- Extent: Skull base → tracheal bifurcation (T4)
- Contents: Retropharyngeal lymph nodes (most prominent in children - Rouviere's nodes)
- Infection spreads here from the parapharyngeal space, and can descend to the posterior mediastinum
- A midline raphe divides it into two lateral halves (preventing purely lateral spread)
"DANGER SPACE" (Space 4)
- Location: Between the alar fascia anteriorly and the prevertebral fascia posteriorly
- Extent: Skull base → posterior mediastinum down to the diaphragm - the longest potential space
- Significance: Infection in this space can spread rapidly to the posterior mediastinum (descending necrotizing mediastinitis)
SUMMARY TABLE - Parapharyngeal Space Contents
| Compartment | Contents | Lesions |
|---|---|---|
| Pre-styloid | Fat, deep lobe parotid, maxillary artery, CN V3 branches (inferior alveolar, lingual, auriculotemporal) | Pleomorphic adenoma (deep parotid), lipoma |
| Post-styloid | Internal carotid artery, internal jugular vein, CN IX, X, XI, XII, sympathetic chain, lymph nodes | Paraganglioma, vagal schwannoma, sympathetic neuromas, NPC nodal spread |
CLINICAL PEARLS FOR EXAM
- Pharynx = 12-14 cm; Oesophagus = 25 cm; begins at C6 (lower border of cricoid)
- Fossa of Rosenmuller (pharyngeal recess) = most common site of NPC
- Killian's dehiscence = gap between thyropharyngeus and cricopharyngeus = site of Zenker's diverticulum
- Only pharyngeal muscle supplied by CN IX = stylopharyngeus (all others by pharyngeal plexus via CN X)
- Sensory: nasopharynx = V2; oropharynx/tonsil = CN IX; hypopharynx = internal laryngeal nerve (CN X)
- PPS is an inverted pyramid: base = skull, apex = hyoid
- Styloid complex divides PPS into pre-styloid (parotid, fat, V3 branches) and post-styloid (carotid sheath, CN IX/X/XI/XII, sympathetic chain)
- Pre-styloid mass pushes carotid posteromedially; post-styloid mass pushes fat pad anteriorly
- PPS abscess = trismus + medial tonsillar displacement + no neck swelling (can be masked)
- Danger space extends to the diaphragm - explains why PPS infections can cause descending necrotizing mediastinitis
Anatomy of parotid and its applied anatomy. Ms ent university exam pattern for 20 marks.
parotid gland anatomy facial nerve relations diagram ENT applied anatomy
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.7.content.31.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.
Anatomy of parotid and its applied anatomy. Ms ent university exam pattern for 20 marks.
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.1.content.29.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.