Fever in children when to actually worry?
Reading File
Searching the Web
fever in children when to worry red flags 2024 pediatric guidelines
Finding Sources
Searching PubMed
"fever" AND "children" AND "management"
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
I now have comprehensive information from Rosen's Emergency Medicine. Here is the full, evidence-based answer:
Fever in Children: When to Actually Worry
Fever is defined as a rectal temperature ≥38°C (100.4°F). It is one of the most common reasons children are brought to the ED or clinic, and the vast majority of cases are self-limited viral illnesses. The key question is not "what is the temperature?" but "how does the child look and act?"
Age Is the Most Important Factor
Under 28 Days Old (Neonates) - Always High Alert
Any fever ≥38°C in a neonate is a medical emergency. Go to the ER immediately. Neonates have immature immune systems and cannot localize infections. The source is often bacterial - group B Streptococcus, E. coli, Listeria, herpes - all potentially fatal without rapid treatment. The clinical picture can be deceptively normal early on, which is why all neonates with fever receive a full sepsis workup (blood, urine, CSF cultures) and are admitted.
28 to 90 Days Old - Urgent Evaluation Required
These infants need a sepsis evaluation even if they appear well. The algorithm below, from Rosen's Emergency Medicine, shows exactly how this age group is triaged:
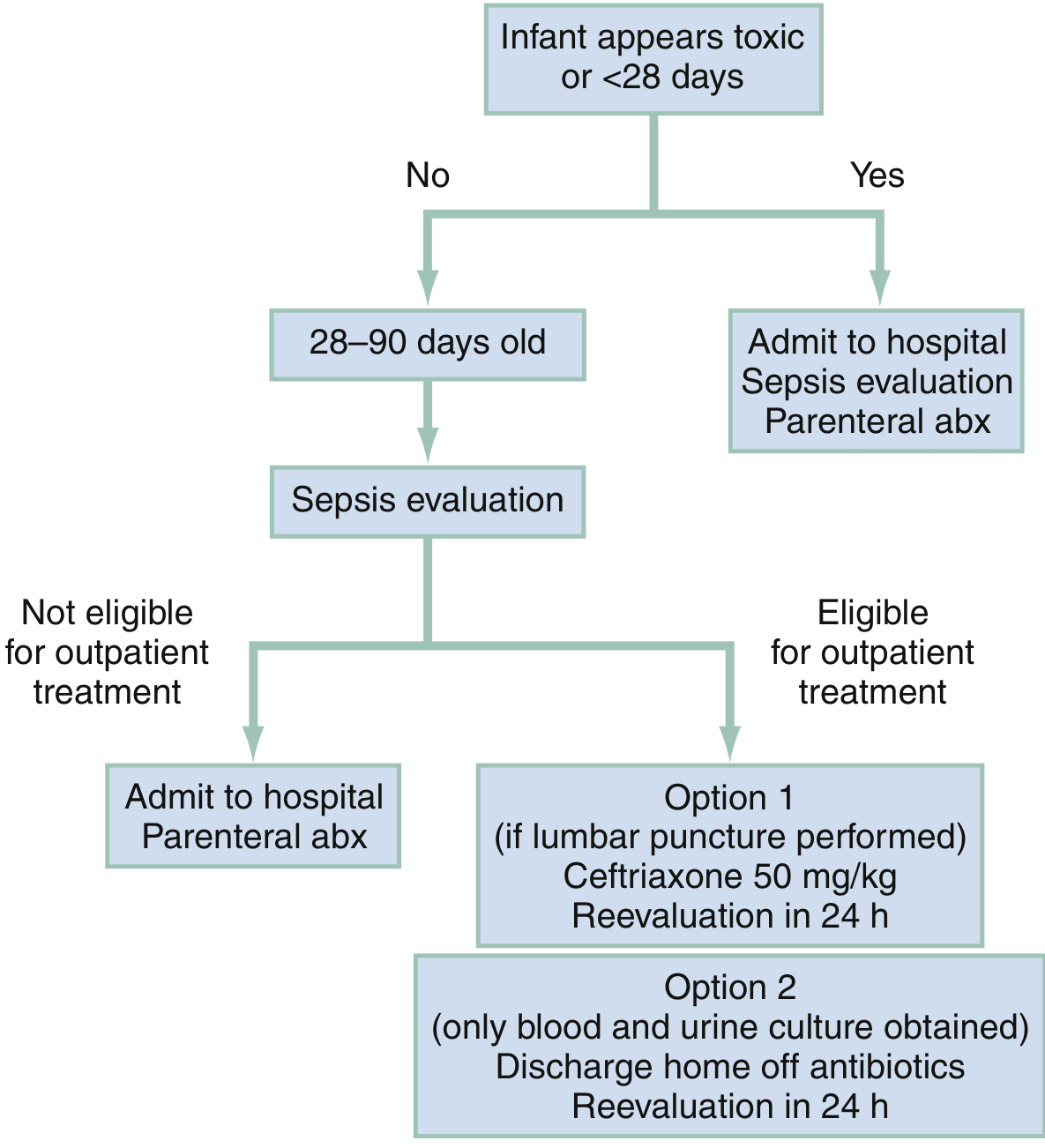
Low-risk infants (normal WBC 5,000-15,000 cells/mm³, negative urinalysis, no focal infection, reliable follow-up) may be discharged, but only after this workup is completed.
3 to 36 Months - Assess Appearance
Most fevers at this age are from viral URIs, roseola, croup, bronchiolitis, gastroenteritis, or fifth disease. History, immunization status (especially Hib and pneumococcus), and the physical exam guide decisions. A well-appearing child without a focus of infection can usually be managed as outpatient. - Rosen's Emergency Medicine, Chapter 161
Universal Red Flags - Go to ER Regardless of Age
These signs mean something serious may be happening and should not be watched at home:
| Red Flag | Why It Matters |
|---|---|
| Any fever in a baby under 28 days | Cannot distinguish benign from sepsis clinically |
| Petechial or purpuric (non-blanching) rash | Meningococcemia until proven otherwise |
| Altered consciousness, limp, won't wake | Possible meningitis, encephalitis, septic shock |
| Seizure (especially first one) | Must rule out CNS infection; febrile seizures need evaluation |
| Stiff neck | Classic meningitis sign |
| Bulging fontanelle (infant) | Raised intracranial pressure |
| Breathing difficulty / grunting | Pneumonia, bronchiolitis severity |
| Persistent vomiting / not drinking | Dehydration risk; also may suggest meningitis |
| Temp >40°C (104°F) in any child | Hyperpyrexia; higher risk of serious bacterial illness |
| Fever persists >5 days | Requires investigation for Kawasaki disease, occult infection |
| Immunocompromised child | Any fever is high-risk; normal immune thresholds don't apply |
The Non-Blanching Rash: A Special Warning
A rash that does NOT fade when you press a glass against it (petechiae or purpura) with fever can mean meningococcal septicemia. This is a life-threatening emergency - the child can deteriorate within hours. This is always an immediate 999/911 situation.
Febrile Seizures: Scary but Usually Benign
About 2-5% of children between 6 months and 5 years have at least one febrile seizure. Simple febrile seizures (generalized, <15 min, full recovery) are not dangerous in themselves, but they require ED evaluation to rule out bacterial meningitis - because clinically distinguishing a benign febrile seizure from one that signals CNS infection is difficult. The AAP has published consensus guidelines for this evaluation.
Roughly 1 in 3 children who have one febrile seizure will have another at some point. - Rosen's Emergency Medicine; Textbook of Family Medicine 9e
When You Can Safely Monitor at Home
A child is generally safe to watch at home if ALL of the following apply:
- Over 3 months old
- Temp under 40°C (104°F)
- Looks and acts reasonably well - making eye contact, can be consoled, interested in surroundings
- Drinking fluids (wet diapers in infants, urinating regularly in older children)
- No red flags from the list above
- Fever responds to antipyretics (paracetamol/ibuprofen)
Treating Fever at Home
- Paracetamol (acetaminophen) or ibuprofen (ibuprofen only for >3 months and >6 kg): both work well
- A 2024 network meta-analysis in Pediatrics (PMID: 39318339) found short-term alternating/combination therapy with both drugs reduces fever slightly more effectively than mono-therapy, but either alone is appropriate for most children
- Do not give aspirin to children (Reye syndrome risk)
- Keep child hydrated; fever increases fluid needs
- Tepid sponging is no longer recommended as standard practice
- The goal of treating fever is comfort, not necessarily normalizing the temperature
Fever of Unknown Origin (FUO) in Children
FUO is defined as fever >38°C on most days for >1 week (pediatric definition varies) with no diagnosis after initial evaluation. The most common cause in children is infectious disease, followed by rheumatologic conditions and, less commonly, malignancy. A detailed history and physical exam, CBC, and urinalysis are the first-line evaluation steps. - Swanson's Family Medicine Review
The Bottom Line
The number on the thermometer matters less than how your child looks. A well-appearing 2-year-old with 39.5°C from a viral cold is far less worrying than a lethargic 6-week-old with 38.2°C. Age under 3 months, toxic appearance, non-blanching rash, and altered consciousness are the four things that should prompt immediate emergency care every time.
Disclaimer: This is educational information. For any specific concern about a child's health, consult a doctor or go to the nearest emergency department.
This is a shared conversation. Sign in to Orris to start your own chat.