Achlasia Cardia
Reading File
Finding Sources
Searching PubMed
achalasia cardia treatment management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive overview of Achalasia Cardia drawn from multiple authoritative surgical and gastroenterology textbooks.
Achalasia Cardia
Definition
Achalasia is a primary esophageal motility disorder characterized by impaired lower esophageal sphincter (LES) relaxation with swallowing and aperistalsis in the smooth muscle segment of the esophagus. When premature, spastic contractions occur in the esophageal body, the condition is termed spastic (Type III) achalasia. - Sleisenger and Fordtran's GI and Liver Disease, p. 729
Pathophysiology
The physiologic abnormalities stem from damage to the myenteric (Auerbach) plexus in the smooth muscle esophagus, with loss of ganglion cells. Key points:
- The degree of ganglion cell loss parallels disease duration, likely progressing from EGJ outflow obstruction → Type II → Type I → end-stage achalasia
- Both excitatory (cholinergic) and inhibitory (NO/VIP-mediated) ganglion neurons are affected, but inhibitory neuron dysfunction is an early manifestation
- Loss of inhibitory neurons explains the two core abnormalities: impaired LES relaxation and aperistalsis
- Muscle strips from the LES fail to relax on ganglionic stimulation; paradoxically, CCK (which normally relaxes the LES via inhibitory neurons) increases LES pressure in achalasia
- The root cause is increasingly understood as an autoimmune process in genetically susceptible individuals - cytotoxic T-cell infiltration in the myenteric plexus, antibodies against myenteric neurons, and an association with specific HLA alleles
- A latent HSV-1 infection is the suspected trigger for the autoimmune response
Classification (Chicago Classification - HRM Subtypes)
| Type | Description | Treatment Response |
|---|---|---|
| Type I (Classic) | Aperistalsis, minimal esophageal pressurization, advanced disease with dilated esophagus | Moderate |
| Type II (Achalasia with Compression) | Aperistalsis + pan-esophageal pressurization; likely early/intermediate disease | Best - ~100% with pneumatic dilation |
| Type III (Spastic) | Premature/spastic contractions of distal esophagus; unique pathogenesis with plexus inflammation but not destruction | 40% with PD vs 86% with LHM; POEM preferred |
Clinical Features
All patients have solid food dysphagia; the majority also have liquid dysphagia (hallmark: dysphagia for both solids and liquids). - Sleisenger and Fordtran's, p. 729
| Symptom | Frequency |
|---|---|
| Dysphagia (solids) | 100% |
| Regurgitation | ~70% |
| Chest pain | 40-67% (early disease) |
| Heartburn (pseudoreflux) | 40-50% |
| Weight loss | Variable |
| Halitosis / hiccups | Less common |
Key clinical points:
- Onset is typically gradual, often present for years before diagnosis
- Regurgitant is non-bilious, non-acid, mixed with saliva, and may contain food eaten hours or days earlier
- "Heartburn" is caused by bacterial fermentation of retained food - not true GERD; this leads to misdiagnosis and inappropriate PPI therapy (average 29-month delay in one study)
- With advanced disease: bronchopulmonary complications from aspiration occur in up to 10%
- Rare: stridor/airway compromise from esophageal dilatation compressing the membranous trachea
Eckardt Score - used to assess severity and treatment response (scores 4 symptoms - dysphagia, regurgitation, weight loss, chest pain; each 0-3 points; total 0-12; score ≤3 = successful treatment). - Sabiston Textbook of Surgery
Diagnosis
A thorough work-up includes EGD + barium swallow + esophageal manometry as the standard triad.
1. Endoscopy (EGD)
- First test usually done for dysphagia
- Normal in ~40% of patients
- May show: retained food/saliva, stasis esophagitis, Candida infection
- Mandatory to exclude pseudoachalasia (malignancy at the GEJ)
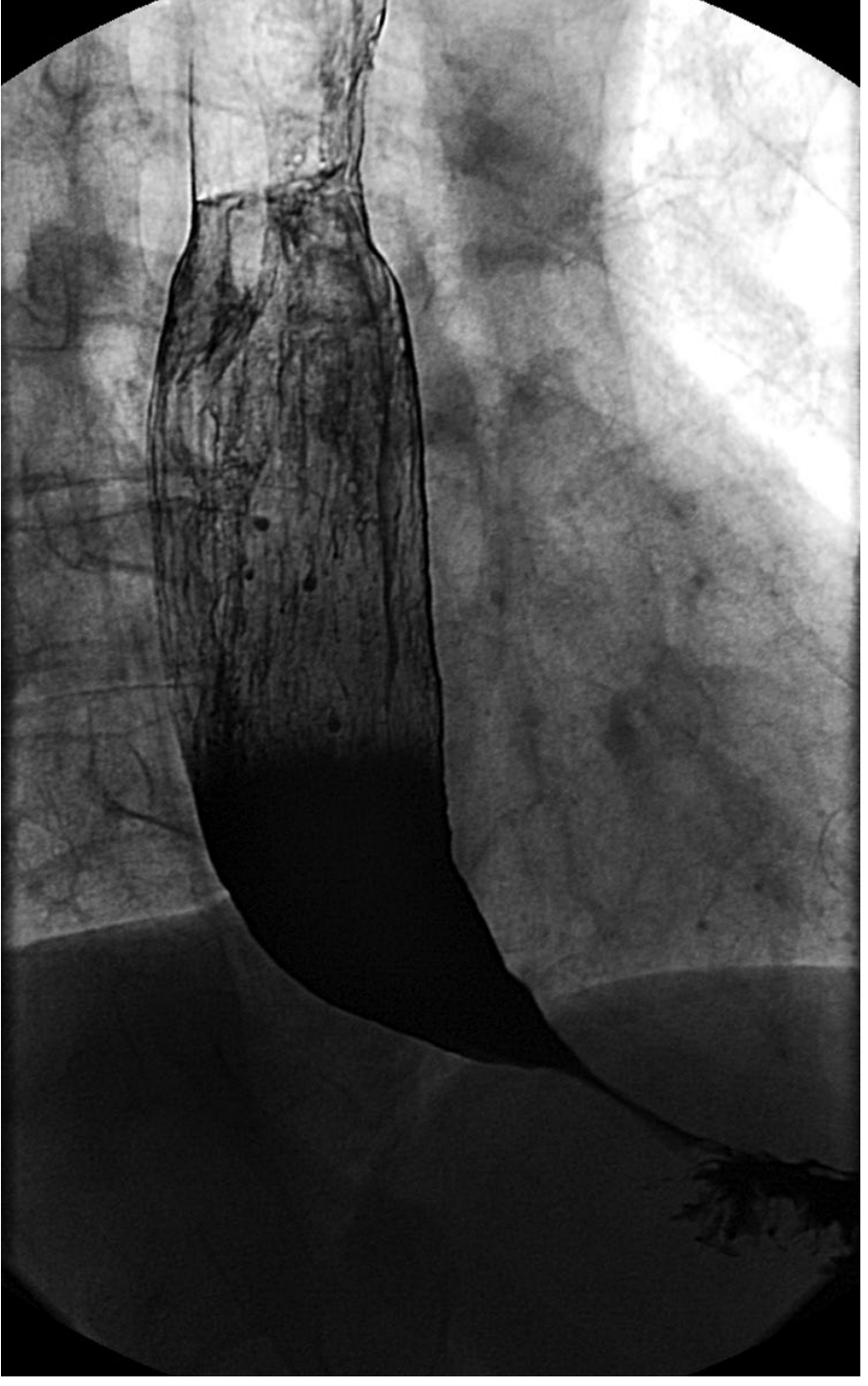
2. Barium Swallow (Esophagram)
- Classic appearance: "bird's beak" or rat-tail tapering at the distal esophagus
- Dilated, tortuous esophagus with stasis of contrast
- Air-fluid level, tertiary contractions
- Can reveal additional pathology (diverticulum, sigmoid deformity)
- Normal in ~30% of early cases
- Important for planning treatment (degree of dilatation, axis of esophagus)
3. High-Resolution Esophageal Manometry (HRM)
- Gold standard for diagnosis
- Classic findings: elevated integrated relaxation pressure (IRP), aperistalsis
- Allows subtyping into Types I, II, III (Chicago Classification)
- Critical for treatment planning
4. Additional Tests
- Ambulatory pH monitoring: for patients with heartburn - differentiates true GERD from fermentation-induced pseudo-reflux (look for slow pH drift vs. discrete reflux events)
- FLIP (Functional Lumen Imaging Probe): assesses esophageal compliance and distensibility using impedance planimetry; corroborates HRM findings; useful to assess effect of treatment
Treatment
Treatment is palliative - the underlying neuropathology cannot be reversed. The goal is to reduce LES pressure and improve esophageal emptying. - Sabiston Textbook of Surgery
1. Pharmacologic Therapy (temporizing only)
- Calcium channel blockers (nifedipine 30-40 mg/day sublingually before meals): modest benefit, side effects common (flushing, dizziness, edema)
- Nitrates (isosorbide dinitrate sublingually): reduce LES pressure; limited efficacy, headaches common
- Sildenafil (50 mg): blocks PDE-5, reduces LES pressure; peaks at 15-20 min, lasts <1 hour; limited practical use
- Overall: minimal/temporary benefit; best for bridging or non-surgical candidates
2. Botulinum Toxin Injection
- Injected into 4 quadrants of the LES (standard dose 80-100 units)
- Inhibits ACh release from cholinergic terminals, reducing LES pressure
- 66% improvement in dysphagia at 6 months; minimal efficacy at 1 year
- Repeat injections cause fibrosis, complicating future surgery
- Best reserved for elderly or frail patients who are poor surgical/endoscopic candidates
3. Pneumatic Dilation (PD)
- Requires LES distension to at least 3 cm (Rigiflex balloons: 3.0, 3.5, 4.0 cm)
- Disrupts circular muscle of the sphincter
- Done over a guidewire under fluoroscopy with conscious sedation
- ~90% effective; risk of esophageal perforation ~1%
- Preferred initial treatment for Type II achalasia (100% efficacy in European RCT vs 93% for LHM)
- Less effective for Type III (only 40% success)
4. POEM (Per-Oral Endoscopic Myotomy)
Introduced ~2010; now a major therapeutic option:
- 4 steps: submucosal injection + mucosal incision (10-12 cm above GEJ) → submucosal tunneling past GEJ by 2-3 cm → myotomy of circular fibers (preserving longitudinal) → mucosal closure with clips/sutures
- Symptom relief >90% of patients at 1-2 years
- Achilles heel: very high rate of postoperative GERD (~47-57%) because no fundoplication is added
- Preferred for Type III achalasia because a longer myotomy onto the esophageal wall is possible
- Equivalent efficacy to LHM for Types I and II
5. Laparoscopic Heller Myotomy (LHM) + Partial Fundoplication
- Long-standing gold standard surgical treatment
- Done laparoscopically; myotomy of LES muscle with partial fundoplication (Dor or Toupet) added
- Clinical success ~90% at 2 years
- Much lower GERD rate than POEM: ~11-20% vs 47-57%
- The addition of fundoplication reduces postoperative reflux from 48% to 9%
- Preferred over POEM for young patients where lifelong GERD exposure (Barrett esophagus, adenocarcinoma risk) is a concern
Treatment Summary by Subtype
| Achalasia Type | Preferred Treatment |
|---|---|
| Type I | LHM or Pneumatic Dilation |
| Type II | Pneumatic Dilation (100% efficacy) or LHM/POEM |
| Type III | POEM (superior due to longer myotomy) |
| Elderly/frail | Botulinum toxin injection |
| End-stage/refractory | Esophagectomy with gastric pull-up (~4% mortality) |
Complications and Long-term Issues
Post-treatment GERD
- After POEM: ~50-57% develop pathologic reflux
- After LHM without fundoplication: ~48%
- After LHM + Dor fundoplication: ~9%
- Long-term GERD can cause esophagitis, Barrett's esophagus, and adenocarcinoma
Squamous Cell Carcinoma Risk
- 17-fold increased risk compared to age-matched controls; however, the absolute annual incidence remains very low (~0.15%)
- Tumors develop many years after diagnosis in massively dilated esophagus with stasis esophagitis
- Latest ASGE guidelines: do not advocate routine endoscopic surveillance; however, if considered, begin 15 years after symptom onset
Treatment Failure
Evaluation should include: endoscopy, HRM, FLIP study, timed barium swallow
- Options: repeat dilation, POEM, Heller myotomy, or reoperation
- Reoperation is less effective than the initial procedure
- In extreme cases: esophagectomy
Pseudoachalasia
Always consider pseudoachalasia (malignancy at the GEJ mimicking achalasia), especially in:
- Rapid onset of dysphagia (< 1 year)
- Age > 60
- Significant weight loss
- Incomplete LES relaxation without aperistalsis on manometry
EGD with biopsies, CT scan, and endoscopic ultrasound are required to exclude malignancy.
Recent Evidence (2024-2026)
Recent systematic reviews and meta-analyses confirm:
- FLIP-guided assessment is increasingly used to compare outcomes after POEM vs. Heller myotomy (PMID 40399616)
- Same-day discharge after POEM is safe and feasible based on a 2026 meta-analysis (PMID 42377530)
These do not contradict the above textbook guidance but show the field moving toward optimizing peri-procedural POEM management.
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Sabiston Textbook of Surgery | Clinical Gastrointestinal Endoscopy (3e) | Current Surgical Therapy 14e | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.