Testicular atrophy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"testicular atrophy" causes pathology
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Testicular Atrophy
Testicular atrophy refers to a reduction in testicular size and function, affecting the seminiferous tubules and/or Leydig cells, leading to varying degrees of impaired spermatogenesis and androgen production.
Definition and Normal Background
The adult testis normally measures approximately 4 x 3 x 2.5 cm. Atrophy is defined as a significant reduction below this volume. On ultrasound, atrophic testes may appear iso- or hyporeflective compared to the normal side, with homogeneous or mixed-reflectivity parenchyma that can hint at the underlying cause. - Grainger & Allison's Diagnostic Radiology, p. 4080
Causes
Robbins Pathologic Basis of Disease provides the most widely cited classification of causes:
1. Vascular / Ischemic
- Testicular torsion - twisting of the spermatic cord obstructs venous drainage while arteries remain patent, causing hemorrhagic infarction. Even after successful orchiopexy, atrophy occurs in ~27% of patients who had torsion, especially those presenting >10 hours after onset or whose testis did not bleed on deep medullary incision. - Hinman's Atlas of Urologic Surgery, p. 2269
- Progressive atherosclerosis in old age - gradual reduction in blood supply
- Trauma - even without testicular rupture, late-onset atrophy has been documented. Blunt scrotal trauma can cause unilateral atrophy appearing months later. - Grainger & Allison, p. 4080
Ultrasound image: unilateral testicular atrophy 3 months after blunt scrotal trauma:

2. Cryptorchidism (Undescended Testis)
Histologic changes begin as early as 2 years of age in maldescended testes: thickening of the basement membrane, loss of spermatogonia, increased interstitial stroma, and relative Leydig cell prominence. Bilateral cryptorchidism results in sterility. Even unilateral cryptorchidism may cause atrophy of the contralateral, normally descended testis, suggesting an underlying intrinsic gonadal abnormality. Orchiopexy is recommended at 6-12 months of age. - Robbins & Kumar Basic Pathology, p. 583
3. Inflammatory / Infectious
- Epididymo-orchitis (bacterial, most common): infection reaches the testis via the vas deferens or spermatic cord lymphatics. Fibrous scarring after resolution can cause atrophy. Leydig cells are usually spared, so androgen production is relatively preserved. - Robbins Pathologic Basis of Disease
- Mumps orchitis: occurs in 20-30% of postpubertal males with mumps (rare in children); acute interstitial orchitis develops ~1 week after parotitis. Sterility is a rare but recognized complication.
- Tuberculosis: the most common cause of testicular granulomatous inflammation; typically begins as epididymitis with secondary testicular involvement
- HIV/AIDS: testicular atrophy is a frequent autopsy finding. The etiology is multifactorial - fever, chronic illness, cachexia, cytokine activation, and direct cytotoxic effects of HIV. Patients with BMI <20 are 3.5x more likely to develop atrophy. Disseminated CMV infection is associated with a fivefold increased incidence. - Campbell-Walsh Urology, p. 2891
4. Endocrine / Genetic
- Klinefelter syndrome (47,XXY): the prototype primary testicular failure. Testicular atrophy with hyalinisation of seminiferous tubules and hypergonadotropic hypogonadism are the hallmarks. - Forensic Medicine & Toxicology; Robbins & Kumar Basic Pathology
- Hypopituitarism: loss of LH/FSH support leads to secondary atrophy
- Exhaustion atrophy: paradoxically, persistent stimulation by high levels of FSH can exhaust the tubular epithelium
5. Toxic / Iatrogenic
- Irradiation: highly toxic to spermatogonia; dose-dependent
- Antiandrogen therapy (e.g., for prostate carcinoma): suppression of testosterone leads to atrophy
- Cirrhosis and alcohol:
- Cirrhosis elevates sex hormone-binding globulin, shifting the hormone balance toward estrogens ("feminization syndrome")
- Alcohol has direct toxic effects on Leydig cells and suppresses the hypothalamic-pituitary-gonadal axis (decreased LH, decreased responsiveness to GnRH)
- Spironolactone (commonly used in cirrhosis) displaces androgen from receptors and increases estradiol production
- Sleisenger & Fordtran's GI & Liver Disease, p. 1825
6. Varicocele
A varicocele (dilation of the pampiniform plexus veins) causes elevated scrotal temperature and altered testicular blood flow. Varicocele-related testicular atrophy is well-documented, particularly in adolescents and young adults. - Campbell-Walsh Urology
7. Surgical Injury
- Inguinal herniorrhaphy: ischemic orchitis occurs in ~1% of primary hernioplasties but is significantly more common after re-do repairs. Damage to the pampiniform plexus (rather than the testicular artery itself) is the most common mechanism. Deliberate testicular artery ligation carries a ~14% risk of frank atrophy. - Schwartz's Principles of Surgery; Mulholland & Greenfield's Surgery
8. General / Systemic
- Generalized malnutrition or cachexia - any cause
- Aging - part of the normal aging process (physiological atrophy)
Concise Summary of Causes (Robbins Classification)
| Category | Key Examples |
|---|---|
| Vascular | Atherosclerosis, torsion, trauma |
| Developmental | Cryptorchidism |
| Infectious/Inflammatory | Orchitis (bacterial, mumps, TB), HIV/CMV |
| Genetic | Klinefelter syndrome |
| Endocrine | Hypopituitarism, exhaustion atrophy |
| Toxic/Iatrogenic | Irradiation, antiandrogens, varicocele |
| Metabolic/Systemic | Cirrhosis, alcohol, malnutrition/cachexia |
Histopathology
The histologic changes of testicular atrophy, regardless of cause, follow a common pattern mirroring that of cryptorchidism:
-
Thickening and hyalinisation of the tubular basement membrane
-
Loss of spermatogonia and other germ cells
-
Increased interstitial (peritubular) fibrosis and stroma
-
Relative prominence of Leydig cells (which are usually spared unless severe)
-
In extreme cases: complete "vanishing testis" syndrome
-
Robbins Pathologic Basis of Disease
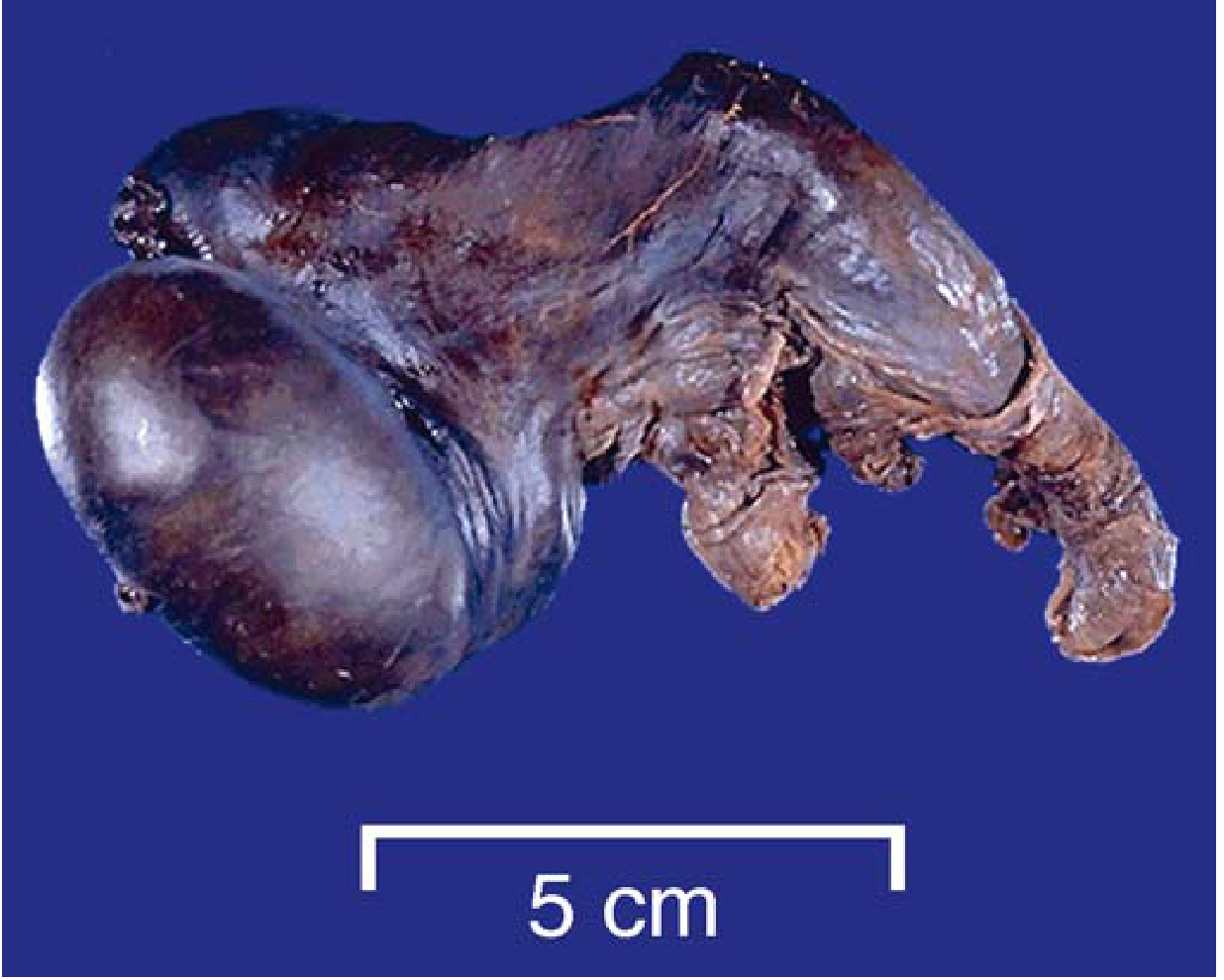
Gross pathology - testicular torsion with hemorrhagic infarction (atrophy precursor):
Clinical Consequences
- Infertility - loss of spermatogonia impairs or eliminates spermatogenesis
- Hypogonadism - if Leydig cells are also affected, testosterone deficiency leads to decreased libido, erectile dysfunction, fatigue, loss of muscle mass, and osteoporosis
- Increased cancer risk - atrophic and cryptorchid testes carry a significantly elevated risk of germ cell tumors (seminoma is the most common); this risk persists even in the contralateral testis and is not fully reversed by orchiopexy
- Psychological impact - body image concerns
Imaging
Scrotal ultrasound (US) is the primary modality. Atrophic testes typically appear smaller than the contralateral side, with variable echogenicity. The pattern of echogenicity may correlate with the underlying cause. US is also the first-line tool for excluding concurrent neoplasia, which is an important concern in atrophic testes. - Grainger & Allison's Diagnostic Radiology
Management Principles
- Treat the underlying cause where possible (e.g., early orchiopexy for cryptorchidism, prompt detorsion within 6 hours, varicocelectomy in adolescents with volume loss)
- Monitor for malignancy - regular self-examination; ultrasound surveillance in high-risk atrophic testes
- Hormone replacement - testosterone replacement therapy for symptomatic hypogonadism
- Fertility preservation - sperm banking before gonadotoxic therapy; microdissection testicular sperm extraction (micro-TESE) for azoospermia (notably, severe testicular atrophy does not preclude successful micro-TESE) - Campbell-Walsh Urology
- Post-torsion follow-up - close surveillance for atrophy after orchiopexy, especially with long duration of symptoms
This is a shared conversation. Sign in to Orris to start your own chat.