Nsaids
Reading File
Finding Sources
Finding Sources
Searching PubMed
NSAIDs pharmacology safety
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive, well-sourced information to deliver a thorough answer on NSAIDs.
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
Overview
NSAIDs are a chemically diverse group of drugs sharing three main therapeutic effects: analgesic, anti-inflammatory, and antipyretic. They are among the most widely used drugs worldwide and act primarily by inhibiting cyclooxygenase (COX) enzymes, thereby blocking prostaglandin synthesis.
Mechanism of Action
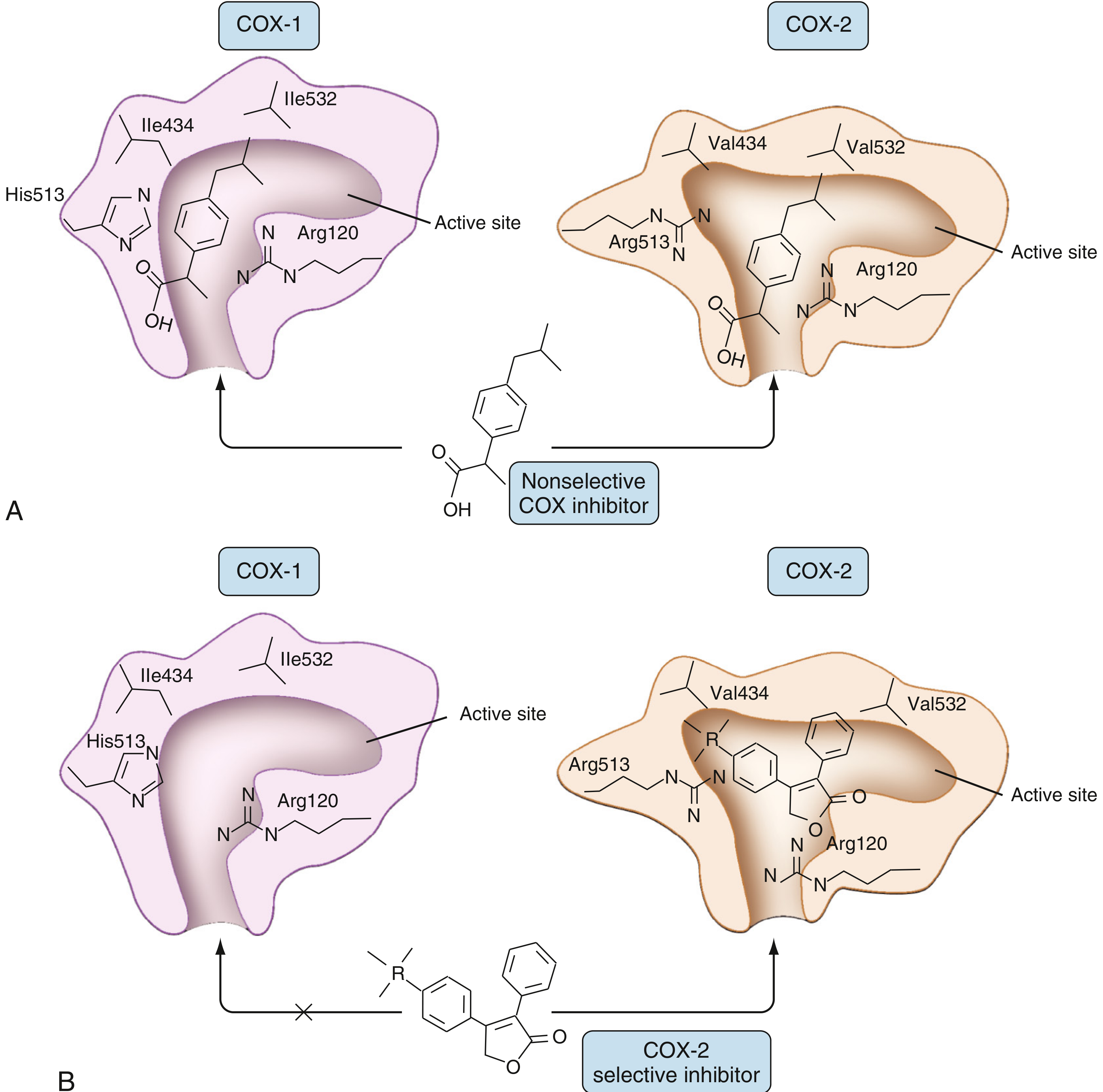
NSAIDs inhibit the COX active site to prevent conversion of arachidonic acid (AA) into prostaglandins, prostacyclins, and thromboxanes. The COX enzymes are heterobifunctional - they first incorporate oxygen into AA to produce PGG2, then reduce PGG2 to PGH2. PGH2 is then converted by terminal synthases into the stable prostanoids.
Binding mechanisms differ by drug:
| Drug | Mechanism |
|---|---|
| Aspirin | Irreversible covalent inhibitor - acetylates Ser530 on both COX-1 and COX-2 |
| Ibuprofen | Rapid, reversible, time-independent competitive inhibitor - both COX monomers must be blocked |
| Indomethacin, Diclofenac | Time-dependent allosteric inhibitors - slow to bind (seconds to minutes), slow to leave (hours), need only block one monomer |
| Celecoxib, Rofecoxib | Time-dependent, strong COX-2 selective inhibitors - bind the hydrophobic side pocket unique to COX-2 |
The COX-2 active site channel is slightly larger than COX-1, which is the structural basis for developing selective inhibitors.
COX Isoforms: COX-1 vs COX-2
| Feature | COX-1 | COX-2 |
|---|---|---|
| Expression | Constitutive - most tissues (platelets, gastric mucosa, renal collecting tubules, endothelium) | Inducible - upregulated by IL-1β, TNF, PDGF, EGF in inflammatory cells |
| Role | Homeostasis: gastric mucosal protection, platelet aggregation, renal function | Inflammation; also elevated in colon/prostate neoplasms |
| Inhibition consequences | GI ulceration, platelet dysfunction, renal effects | Reduced inflammation; cardiovascular risk with selective inhibition |
COX-2 is also expressed constitutively in the kidney, brain, and vasculature - this is why COX-2 inhibitors are not without systemic effects.
Classification
1. Non-selective COX inhibitors (COX-1 + COX-2)
Salicylates
- Aspirin (acetylsalicylic acid) - irreversible
Propionic acid derivatives
- Ibuprofen, Naproxen, Ketoprofen, Flurbiprofen, Fenoprofen
Acetic acid derivatives
- Indomethacin, Diclofenac, Ketorolac, Sulindac, Etodolac
Oxicams
- Piroxicam, Meloxicam (meloxicam has some COX-2 preference)
Fenamates
- Mefenamic acid
Naphthylalkanone
- Nabumetone
2. Preferential COX-2 inhibitors
- Meloxicam, Nimesulide, Etodolac
3. Selective COX-2 inhibitors (Coxibs)
- Celecoxib, Etoricoxib, Parecoxib
- Rofecoxib and valdecoxib were withdrawn due to cardiovascular risk
Therapeutic Uses
- Acute and chronic pain management (step 1-2 of WHO analgesic ladder)
- Osteoarthritis and rheumatoid arthritis
- Acute gout
- Dysmenorrhoea
- Fever
- Perioperative multimodal analgesia (opioid-sparing)
- Pericarditis
- Aspirin: antiplatelet therapy, secondary cardiovascular prevention
- Topical NSAIDs: local musculoskeletal pain with reduced systemic effects
Adverse Effects
Gastrointestinal
Inhibition of COX-1 removes the protective prostaglandin (PGE2/PGI2) layer from gastric mucosa. Effects range from dyspepsia to ulceration, bleeding, and perforation. NSAID enteropathy of the small bowel (increased permeability, silent mucosal damage, anaemia, hypoalbuminaemia, diaphragm-like strictures) is seen in up to 70% of NSAID users on capsule endoscopy.
"Ulcerations of the small intestine distal to the duodenum are prevalent. Of 713 consecutive autopsy patients, 8.4% of NSAID users had ulcerations compared with only 0.6% of non-users." - Sleisenger & Fordtran's GI Disease
Mitigation: Use lowest effective dose, co-prescribe PPI, prefer COX-2 selective agents in high GI-risk patients.
Renal
Prostaglandins dilate afferent arterioles to maintain renal perfusion, particularly in states of low effective circulating volume. NSAIDs cause:
- Reduced GFR and acute kidney injury (in at-risk patients)
- Sodium and water retention
- Hyperkalaemia
- Papillary necrosis with chronic use
Contraindicated in acute or chronic renal failure.
Cardiovascular
- Selective COX-2 inhibitors (and some non-selective NSAIDs) disturb the prostacyclin (PGI2)/thromboxane A2 (TXA2) balance, favouring a prothrombotic state
- Increased risk of MI and stroke
- Celecoxib: contraindicated perioperatively in CABG patients
- Fluid retention can worsen hypertension and heart failure
Platelet Effects
- Non-selective NSAIDs reversibly inhibit platelet COX-1 (impaired TXA2-dependent aggregation) - increased perioperative bleeding risk
- Aspirin's inhibition is irreversible - platelet function does not recover until new platelets are produced (~7-10 days)
- COX-2 selective agents have minimal antiplatelet effect
Respiratory
- NSAID-exacerbated respiratory disease (aspirin-exacerbated asthma / Samter's triad): shunting AA toward leukotriene synthesis causes bronchoconstriction
- Seen in ~10-20% of asthmatics; COX-2 selective agents may be safer
Other
- Hypersensitivity reactions
- Hepatotoxicity (rare)
- Delayed closure of patent ductus arteriosus (used therapeutically in neonates with indomethacin)
Drug Interactions
| Interacting Drug | Effect |
|---|---|
| Lithium | NSAIDs reduce renal prostaglandins → decreased renal lithium clearance → lithium toxicity (10% to >400% rise, unpredictable) |
| Anticoagulants (warfarin) | Additive bleeding risk |
| Antihypertensives (ACEi, ARB, diuretics) | Attenuated antihypertensive effect; increased AKI risk with ACEi/ARB combination ("triple whammy") |
| SSRIs | Increased GI bleeding risk |
| Methotrexate | Reduced MTX clearance → toxicity |
| Ciclosporin | Increased nephrotoxicity |
- Maudsley Prescribing Guidelines note that NSAIDs can be bought OTC, making the lithium interaction particularly dangerous - patients must be counselled.
Special Populations
| Population | Considerations |
|---|---|
| Elderly | Increased GI, renal, and CV risk; use lowest dose for shortest time |
| Pregnancy | Avoid in 3rd trimester (premature closure of ductus arteriosus, oligohydramnios) |
| Renal impairment | Contraindicated in AKI/CKD |
| Post-CABG | COX-2 selective agents contraindicated |
| Peptic ulcer disease | Avoid or co-prescribe PPI |
| Asthmatics | Use with caution; COX-2 selective may be preferred |
COX-2 Selective Inhibitors vs Traditional NSAIDs
| Feature | Traditional NSAIDs | COX-2 Selective (Coxibs) |
|---|---|---|
| GI toxicity | Higher | Lower (less mucosal COX-1 suppression) |
| Platelet effect | Yes (reversible; irreversible for aspirin) | Minimal |
| CV risk | Moderate (varies by drug) | Higher (particularly with rofecoxib, withdrawn 2004) |
| Renal effects | Yes | Yes (similar) |
| Cost | Lower | Higher |
Sources:
- Firestein & Kelley's Textbook of Rheumatology (Cyclooxygenase Inhibition, Ch. 59)
- Rheumatology 2-Volume Set (Cyclooxygenase Products)
- Fischer's Mastery of Surgery, 8th ed. (NSAIDs in perioperative analgesia)
- Sleisenger & Fordtran's GI and Liver Disease (NSAID enteropathy)
- Bailey & Love's Short Practice of Surgery, 28th ed. (Paracetamol and NSAIDs)
- Maudsley Prescribing Guidelines in Psychiatry, 15th ed. (Lithium-NSAID interaction)
This is a shared conversation. Sign in to Orris to start your own chat.