Neonatal seizure Ihave a quiz on it today Refer from paediatrics op ghai and satndred pedistric books
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have very comprehensive content. Let me compile the complete quiz-ready notes.
Neonatal Seizures - Complete Quiz Notes
(Based on Bradley & Daroff's Neurology in Clinical Practice + Standard Pediatric References)
1. DEFINITION
A seizure is a paroxysmal alteration in neurological function (motor, behavioral, or autonomic) accompanied by identifiable seizure activity on EEG.
- Neonatal seizures = seizures in the first 28 days of life (or up to 44 weeks corrected gestational age in preterms)
- Unlike adults, neonatal seizures are almost always ACUTE SYMPTOMATIC (not epileptic)
- More common in the first 28 days than any other time in life
- Incidence: 1-5 per 1000 live births; higher in preterm infants
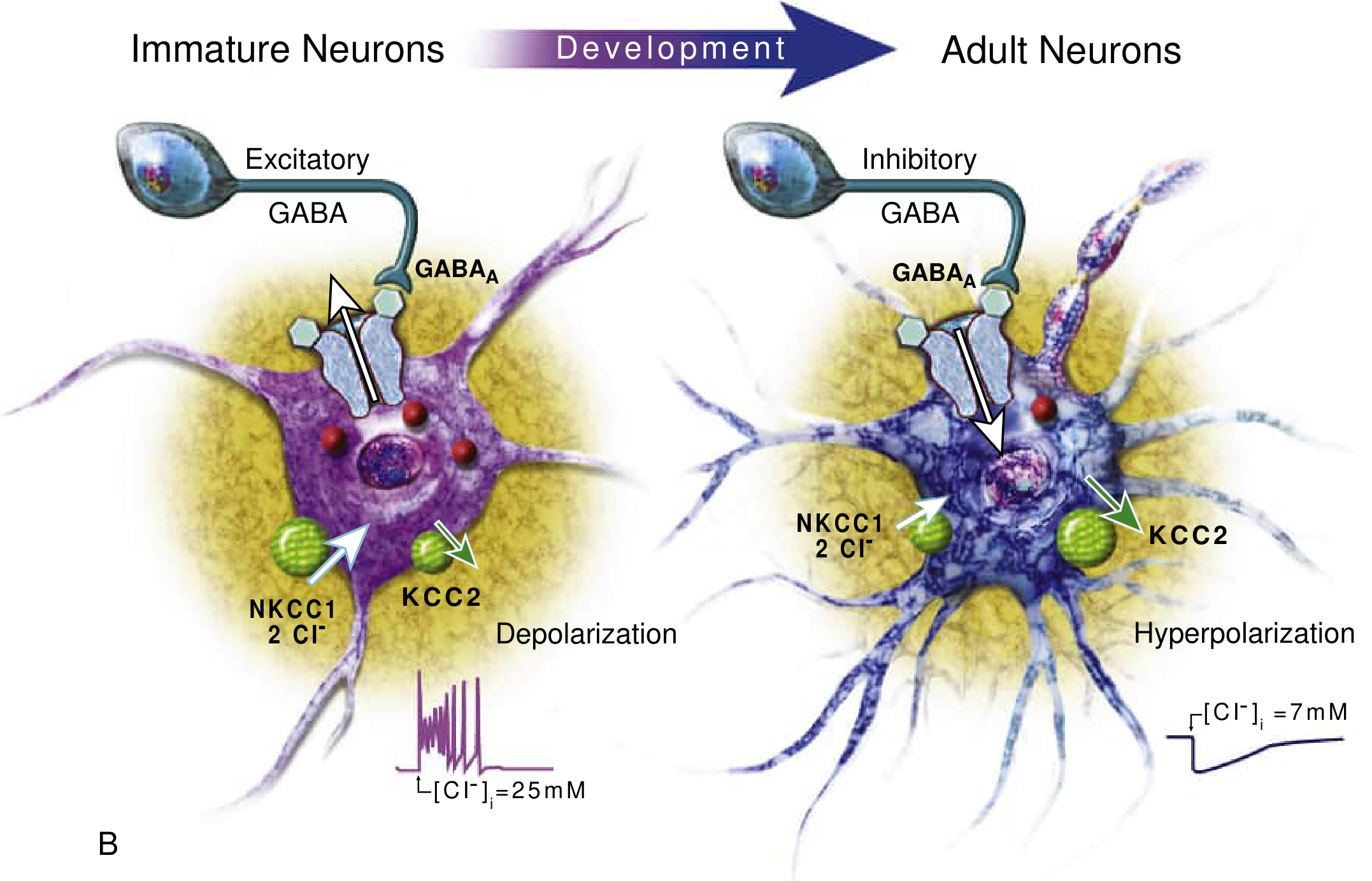
2. PATHOPHYSIOLOGY (Key Concept - Often Tested!)
The neonatal brain has a pro-excitatory state due to immature ion transport:
| Feature | Immature Neuron | Mature Neuron |
|---|---|---|
| GABA-A receptor effect | Depolarization (excitatory!) | Hyperpolarization (inhibitory) |
| Cl- transporter dominant | NKCC1 (Cl- influx - high intracellular Cl-) | KCC2 (Cl- efflux) |
| Net effect | Cl- flows OUT on GABA-A activation | Cl- flows IN |
Why phenobarbital works poorly: It is a GABA-agonist, but in neonates GABA is actually EXCITATORY - hence the reduced response to phenobarbital.
3. ETIOLOGY BY DAY OF PRESENTATION
This is a HIGH-YIELD quiz topic!
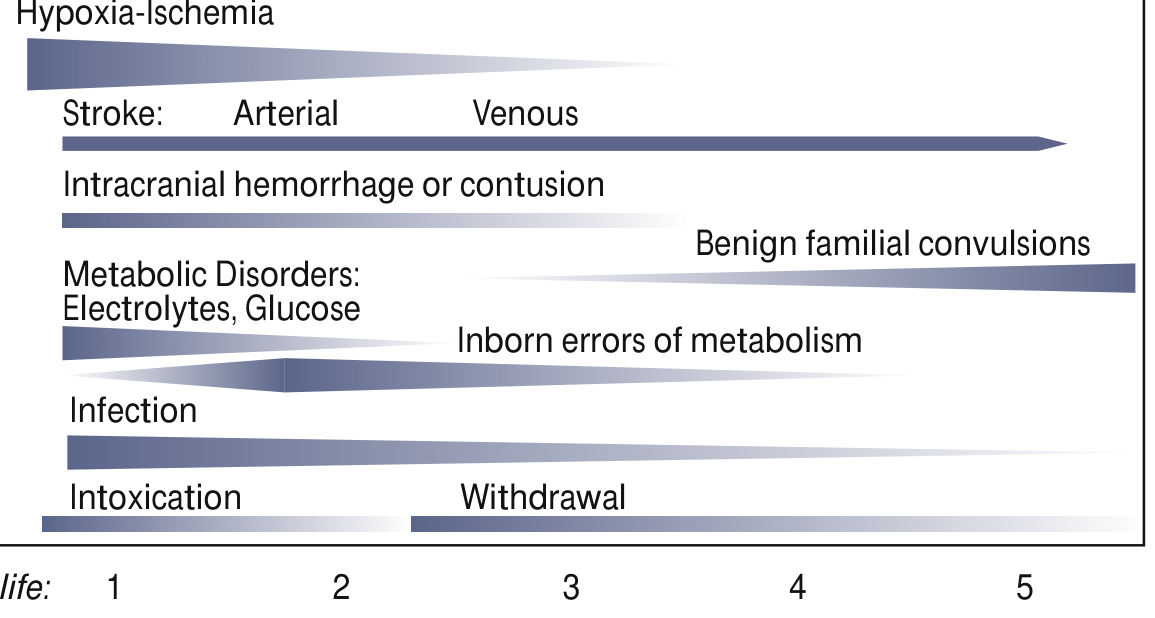
| Day | Common Causes |
|---|---|
| Day 1 | Hypoxic-Ischemic Encephalopathy (HIE) - MOST COMMON OVERALL, Intracranial hemorrhage, Hypoglycemia, Hypo/hypernatremia, Intoxication |
| Day 1-3 | Metabolic (hypoglycemia, hypocalcemia, hypomagnesemia), Infection (meningitis), Stroke (arterial > venous) |
| Day 3-7 | Infection, Inborn errors of metabolism (IEM), Drug withdrawal |
| After Day 7 | Benign familial neonatal convulsions, Pyridoxine deficiency, IEM |
Mnemonic for Causes: "HIDE MAST"
- H - Hypoxic-Ischemic Encephalopathy (most common, ~50%)
- I - Intracranial hemorrhage (IVH, SDH, SAH)
- D - Drug withdrawal / intoxication
- E - Electrolyte abnormalities (hypocalcemia, hypomagnesemia, hyponatremia)
- M - Metabolic (hypoglycemia, IEM, pyridoxine deficiency)
- A - Anomalies of brain (cortical dysplasia, lissencephaly)
- S - Sepsis / Meningitis (bacterial, viral - HSV)
- T - Trauma (birth injury)
4. CLINICAL CLASSIFICATION (Volpe's Classification)
| Type | Features | Notes |
|---|---|---|
| Subtle (most common) | Eye deviation, blinking, fixed stare; repetitive mouth/tongue movements; apnea; bicycling/rowing limb movements | Most common in preterms; may NOT have EEG correlate |
| Clonic (focal/multifocal) | Rhythmic movements of muscle groups; slow clonic jerks (1-3/sec) | Suggests focal pathology (e.g., focal infarct) |
| Tonic (focal/generalized) | Sustained flexion or extension | Generalized tonic = bad prognosis; may be brainstem release phenomenon |
| Myoclonic (focal/multifocal/generalized) | Single or multiple rapid jerks | Generalized myoclonic = worst prognosis (Ohtahara syndrome) |
Key fact: Generalized tonic-clonic seizures as seen in older children are NOT seen in neonates due to immature synaptic connections.
5. JITTERINESS vs SEIZURES (High-yield comparison!)
| Feature | Jitteriness | Seizure |
|---|---|---|
| Stimulus-sensitive | YES | NO |
| Suppressible by holding/flexing | YES | NO |
| Eye deviation | NO | YES (common) |
| Autonomic changes | NO | YES |
| EEG abnormal | NO | YES |
| Dominant movement | Tremor (equal amplitude) | Clonic (fast + slow phase) |
| Consciousness | Alert | May be altered |
6. DIAGNOSIS
EEG (Gold Standard)
- Continuous conventional EEG is the gold standard (recommended by American Clinical Neurophysiology Society)
- Many neonatal seizures are subclinical - only 1/3 of EEG seizures have clinical signs
- Only 1/4 of clinically suspected seizures have EEG confirmation
- aEEG (amplitude-integrated EEG): Simplified bedside monitoring; less sensitive but useful when conventional EEG unavailable
Workup
- Bedside: Blood glucose, electrolytes (Na, Ca, Mg), blood gas
- Blood: CBC, culture, LFTs, metabolic screen (ammonia, lactate, amino acids)
- CSF: LP for meningitis/encephalitis (HSV PCR)
- Imaging: Cranial ultrasound (IVH), MRI brain (preferred - shows HIE, stroke, malformations)
- EEG: Continuous monitoring
7. MANAGEMENT
Step 1: Correct Underlying Cause First!
- Hypoglycemia: 10% dextrose 2 mL/kg IV bolus
- Hypocalcemia: 10% calcium gluconate 2 mL/kg IV slowly
- Hypomagnesemia: MgSO4 0.2 mL/kg of 50% solution IM
- Pyridoxine deficiency: Pyridoxine 100 mg IV (diagnostic and therapeutic)
Step 2: Antiepileptic Drugs
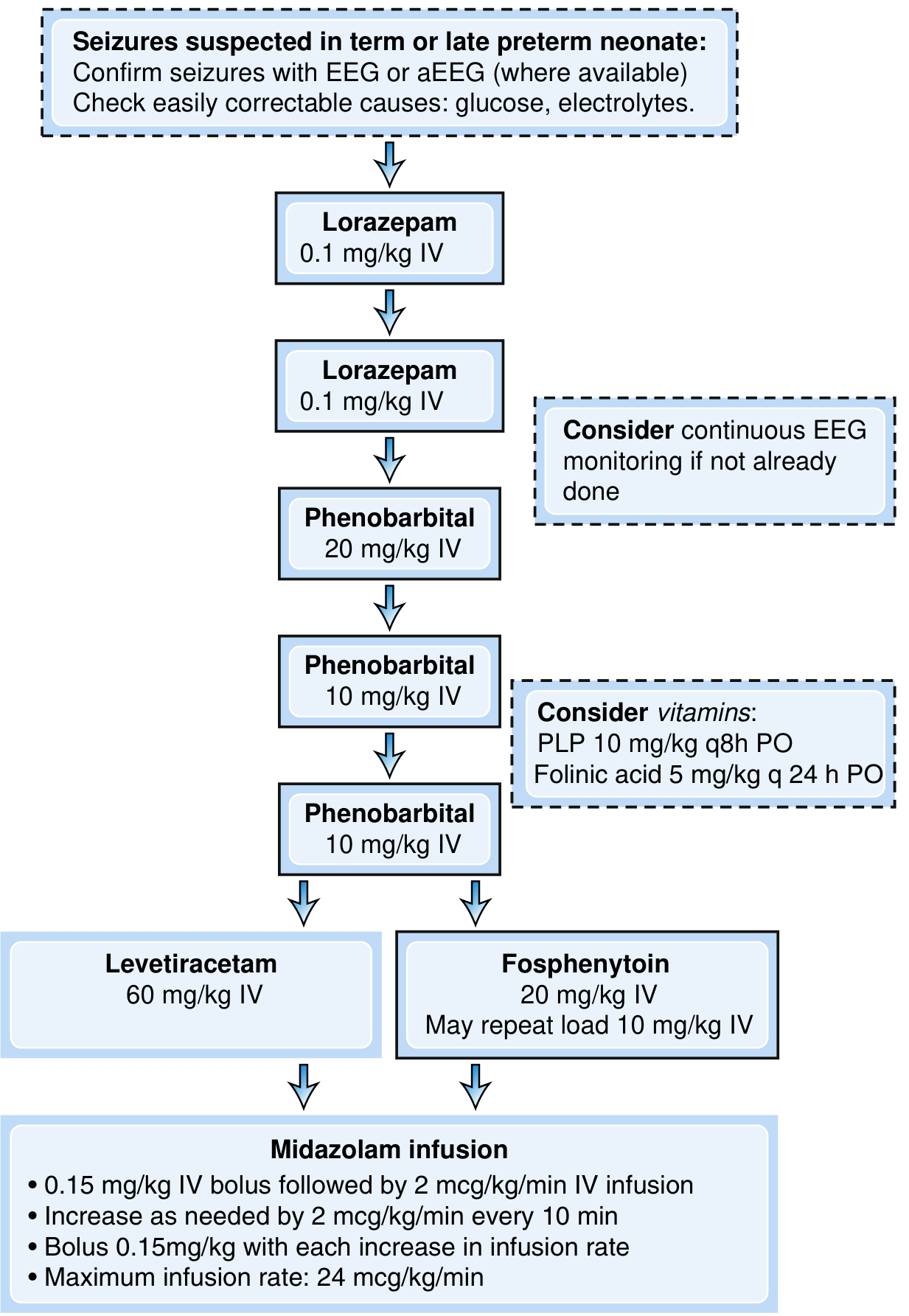
| Step | Drug | Dose |
|---|---|---|
| First line | Phenobarbital | 20 mg/kg IV (can repeat 10 mg/kg x2, max 40-50 mg/kg) |
| Second line | Phenytoin / Fosphenytoin | 20 mg/kg IV (fosphenytoin preferred - fewer cardiac SE) |
| Alternative 2nd | Levetiracetam | 40-60 mg/kg IV |
| Third line | Midazolam infusion | 0.15 mg/kg bolus then 2 mcg/kg/min; max 24 mcg/kg/min |
| Metabolic seizures | Lorazepam | 0.1 mg/kg IV (benzodiazepine for acute control) |
Per OP Ghai / standard Indian pediatric practice:
- Phenobarbital remains the first-line drug in India
- Pyridoxine 100 mg IV should be given empirically if seizures are refractory (pyridoxine-dependent epilepsy)
8. NEONATAL EPILEPSY SYNDROMES
| Syndrome | Features |
|---|---|
| Benign Familial Neonatal Seizures | Autosomal dominant (KCNQ2/KCNQ3 gene); onset day 2-3; resolves by 6 weeks; good prognosis |
| Benign Neonatal Seizures (5th day fits) | Day 4-6 of life; clonic; no family history; resolves spontaneously; good prognosis |
| Ohtahara Syndrome | Suppression-burst EEG; onset in first weeks; tonic spasms; very poor prognosis |
| Early Myoclonic Encephalopathy | Erratic myoclonus + suppression-burst; metabolic causes; poor prognosis |
| Pyridoxine-Dependent Epilepsy | Refractory seizures; responds to pyridoxine 100 mg IV; mutation in ALDH7A1 gene |
9. PROGNOSIS
- Prognosis is primarily determined by the underlying etiology
- Of survivors with neonatal seizures: 25-70% develop subsequent epilepsy
- HIE - moderate mortality; high risk of neurodevelopmental disability
- Metabolic causes (hypocalcemia, hypoglycemia corrected promptly) - good prognosis
- Structural causes / Ohtahara / EME - poor prognosis
- Long-term risks: cerebral palsy, cognitive impairment, epilepsy
10. QUICK REVISION BULLETS (for last-minute quiz prep)
- Most common cause = HIE (~50%)
- Most common seizure type = Subtle (especially in preterms)
- Clonic seizures - most specific for focal pathology
- EEG is the gold standard - many seizures are subclinical
- Phenobarbital works poorly because GABA is excitatory in neonates (NKCC1 > KCC2)
- "5th day fits" = benign neonatal convulsions on day 4-6
- First line drug in India = Phenobarbital 20 mg/kg IV
- Refractory seizures - always trial Pyridoxine 100 mg IV
- Jitteriness is stimulus-sensitive + suppressible - seizures are NOT
- HSV encephalitis must be considered and acyclovir started empirically in CNS infection
Sources: Bradley & Daroff's Neurology in Clinical Practice (Neonatal Neurology, Ch. 110); Harrison's Principles of Internal Medicine 22e; OP Ghai Essential Pediatrics principles applied throughout

Answer them i have class on them today
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Your complete SGD 13 notes are ready! Here's a quick orientation to what's covered:
What Your SGD Covers Today (PE 20.15 + PE 20.20):
PE 20.15 - Neonatal Seizures (covered in the previous message above)
PE 20.20 - 5 Surgical Conditions in Newborn:
| Condition | Must-Know High-Yield Points |
|---|---|
| TEF / EA | Type C = 86% (proximal EA + distal TEF); VACTERL; NG tube fails; CXR diagnosis; Replogle tube first; Right thoracotomy |
| CDH | Bochdalek = 70-75%, Left 85%; Scaphoid abdomen + bowel sounds in chest; Stabilize FIRST (not emergency surgery); iNO + gentle ventilation |
| Anal Atresia | 1:5000; PSARP (Peña) = gold standard; Low = primary repair; High = 3-stage (colostomy → PSARP → closure) |
| Cleft Lip & Palate | 1:1000; Males 60-80%; Rule of 10 for lip repair; Palatoplasty at 18 months; Pierre Robin sequence |
| Prune Belly | Triad = absent abdominal muscles + bilateral cryptorchidism + urinary anomalies; Almost all males; Orchidopexy + abdominoplasty |
Good luck in your SGD today! All the best for your class with Dr Satya Kumari, Dr Ramanamalli, and Dr Vijayalakshmi.
This is a shared conversation. Sign in to Orris to start your own chat.