Neurodegenerative disease drugs in deep details also speak a little about disease too
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching PubMed
neurodegenerative disease drug therapy Alzheimer Parkinson
Reading File
Reading File
I now have very rich data from multiple authoritative textbooks. Let me compile the comprehensive response.
Neurodegenerative Diseases - Complete Drug Reference
What Are Neurodegenerative Diseases?
Neurodegenerative diseases are conditions characterized by progressive, irreversible loss of neurons in the brain and/or spinal cord. The hallmarks include:
- Abnormal protein aggregation (amyloid plaques, tau tangles, alpha-synuclein, huntingtin)
- Mitochondrial dysfunction
- Excitotoxicity (overactivation of glutamate/NMDA receptors)
- Oxidative stress
- Neuroinflammation
The five major diseases covered here are: Alzheimer's (AD), Parkinson's (PD), Amyotrophic Lateral Sclerosis (ALS), Huntington's (HD), and Multiple Sclerosis (MS).
1. ALZHEIMER'S DISEASE (AD)
The Disease
AD has three defining pathological features:
- Amyloid beta (Aβ) plaques - deposited extracellularly, beginning ~15 years before symptoms appear
- Neurofibrillary tangles (NFTs) - intracellular tau protein hyperphosphorylation
- Loss of cholinergic neurons from the nucleus basalis of Meynert (basal forebrain)
The loss of cholinergic innervation from the basal forebrain to the prefrontal cortex, amygdala, and hippocampus is directly responsible for the memory loss and cognitive decline. This is the basis for the "cholinergic hypothesis" and the rationale for AChE inhibitors.
Stages: Mild Cognitive Impairment (MCI) → Mild → Moderate → Severe dementia. At early stages, cholinergic postsynaptic targets remain intact (AChE inhibitors work). At later stages, targets are lost (drugs become less effective).
AD Drugs
A. Acetylcholinesterase (AChE) Inhibitors
These are the first-line drugs for mild-to-moderate AD. They prevent breakdown of acetylcholine, boosting residual cholinergic tone.
| Drug | Mechanism | Dose | Indication | Metabolism |
|---|---|---|---|---|
| Donepezil | Noncompetitive AChE inhibitor | 10 mg once daily | Mild-to-severe AD | CYP2D6, CYP3A4 |
| Rivastigmine | Noncompetitive AChE + BuChE inhibitor | 9.5 mg/24h (transdermal) or 3-6 mg BID | Mild-moderate AD; also PD dementia (only drug approved for both) | Esterases |
| Galantamine | Competitive AChE inhibitor; also allosterically potentiates nicotinic receptors | 8-12 mg BID (IR) or 16-24 mg/day (ER) | Mild-moderate AD | CYP2D6, CYP3A4 |
Key points:
- Starting doses are half the maintenance dose for the first month
- BuChE (butyrylcholinesterase) is upregulated in AD brain; rivastigmine inhibits both enzymes
- Donepezil preferred for once-daily dosing; rivastigmine preferred in PD dementia
- Common adverse effects: nausea, diarrhea, bradycardia, increased gastric acid
- Galantamine's nicotinic receptor potentiation may provide additional cognitive benefit
B. NMDA Receptor Antagonist - Memantine
Mechanism: Uncompetitive (voltage-dependent) antagonist of NMDA-type glutamate receptors. Blocks pathological, sustained NMDA activation (excitotoxicity) while still permitting physiological, transient NMDA activation needed for learning and memory.
Indication: Moderate-to-severe AD (insufficient evidence in mild stages)
Key points:
- Temporarily delays deterioration but does not cure
- Mild adverse effects: headache, dizziness
- Renal excretion - reduce dose in severe renal impairment
- Can be combined with AChE inhibitors for additive benefit
C. Amyloid Immunotherapy (Disease-Modifying Therapy)
This represents a paradigm shift - these drugs actually target the underlying pathology (Aβ plaques), not just symptoms.
| Drug | Type | Mechanism | Notes |
|---|---|---|---|
| Lecanemab (Leqembi) | Anti-Aβ monoclonal antibody | Targets soluble Aβ protofibrils; reduces plaque burden | Approved 2023; given for MCI or mild dementia confirmed by positive amyloid PET or CSF biomarkers |
| Donanemab | Anti-Aβ monoclonal antibody | Targets insoluble amyloid plaques | Phase III showed slowed cognitive decline |
| Aducanumab (Aduhelm) | Anti-Aβ monoclonal antibody | Reduces amyloid plaques | Controversial FDA accelerated approval 2021; limited commercial use due to inconclusive efficacy |
Critical safety concern - ARIA (Amyloid-Related Imaging Abnormalities):
- ARIA-E: cerebral edema
- ARIA-H: microhemorrhages
- Monitoring with serial MRI is mandatory during therapy
- Higher risk in APOE ε4 carriers
Pivotal trial requirement: Patients must have confirmed amyloid positivity (via PET scan OR CSF biomarkers - low Aβ42, elevated total tau/phospho-tau) before starting these drugs.
D. Treatment of Non-Cognitive Symptoms in AD
- Depression: SSRIs preferred (avoid tricyclics - anticholinergic effects worsen cognition)
- Agitation/Psychosis: Atypical antipsychotics (risperidone, quetiapine, olanzapine) used cautiously - FDA black box warning for increased mortality in elderly with dementia. Use lowest effective dose for shortest time.
- Citalopram: 30 mg/day improved agitation vs. placebo but causes QTc prolongation - not routinely recommended
- Brexpiprazole (Rexulti): Newer agent specifically approved for agitation in AD
- Dextromethorphan/quinidine (Nuedexta): Approved for pseudobulbar affect; also used for agitation
- Sun-downing: Maximize daytime light exposure, regular activity, limit daytime napping
2. PARKINSON'S DISEASE (PD)
The Disease
PD is caused by progressive loss of dopaminergic neurons in the substantia nigra pars compacta (SNc), leading to dopamine deficiency in the nigrostriatal pathway. The basal ganglia circuit depends on dopamine to facilitate voluntary movement; its absence produces the cardinal symptoms:
- Tremor (resting, "pill-rolling")
- Rigidity (cogwheel)
- Bradykinesia/Akinesia (slowness of movement)
- Postural instability
Pathologically, Lewy bodies (alpha-synuclein aggregates) accumulate in surviving neurons. The dopamine/acetylcholine imbalance in the striatum explains why anticholinergics can provide symptom relief.
PD Drugs
A. Levodopa/Carbidopa - The Gold Standard
Levodopa is a dopamine precursor that crosses the blood-brain barrier (dopamine cannot). Carbidopa is a peripheral DOPA decarboxylase inhibitor that cannot cross the BBB - it blocks peripheral conversion of levodopa to dopamine, reducing side effects and increasing CNS bioavailability.
Formulations:
| Form | Use Case |
|---|---|
| Carbidopa/levodopa (IR) | Standard initial therapy |
| Carbidopa/levodopa (SR) | Motor fluctuations ("wearing off") |
| Carbidopa/levodopa (ER capsules - Rytary) | Motor fluctuations; immediate + extended-release beads combined |
| Carbidopa/levodopa intestinal gel (Duopa) | Advanced PD; requires gastrostomy tube with jejunal extension |
| Levodopa inhalation (Inbrija) | "Wearing off" episodes; can be co-administered with carbidopa |
Motor complications over time:
- Wearing off - benefit fades before next dose
- Dyskinesias - involuntary movements at peak dose
- On/off phenomenon - unpredictable switching between mobile ("on") and immobile ("off") states
- Therapeutic window narrows after several years of treatment
B. Dopamine Receptor Agonists (DAs)
Longer-acting than levodopa; can reduce psychosis, impulse control disorders, and excessive daytime sleepiness risks. Often used as initial monotherapy in younger patients to delay levodopa.
| Drug | Receptor | Formulation | Special Notes |
|---|---|---|---|
| Ropinirole | Selective D2-class agonist | IR (TID) or SR (once daily) | Also for restless legs syndrome |
| Pramipexole | Selective D2-class agonist | IR (TID) or SR (once daily) | Also for restless legs syndrome |
| Rotigotine | D2 + D1 agonist | Transdermal patch | Once-daily application; good for dysphagia patients |
| Apomorphine | D1/D2 agonist | Sublingual film or subcutaneous injection | Rescue therapy for acute "off" episodes; strongly emetogenic - requires concurrent antiemetic; contraindicated with 5HT3 antagonists (risk of hypotension) |
C. COMT Inhibitors
Catechol-O-methyltransferase (COMT) inhibitors block peripheral breakdown of levodopa, increasing its bioavailability and extending its effect. Given with each levodopa dose to reduce "wearing off."
| Drug | Half-life | Notes |
|---|---|---|
| Entacapone | Short | Inhibits peripheral COMT only; given with each levodopa dose |
| Tolcapone | Long | Inhibits central AND peripheral COMT; hepatotoxic - monitor LFTs; only if not responding to other treatments |
| Carbidopa/levodopa/entacapone (Stalevo) | - | Fixed-dose triple combination |
| Opicapone | Long (once daily) | Once-daily peripheral COMT inhibitor; newer option |
D. MAO-B Inhibitors
Block monoamine oxidase type B in the CNS, reducing oxidative metabolism of dopamine and extending dopamine's effect. Can be used as monotherapy early or as adjuncts.
| Drug | Notes |
|---|---|
| Rasagiline | Monotherapy or adjunct; many drug interactions (avoid meperidine, risk of serotonin syndrome); CYP1A2 inhibitors double its plasma concentration |
| Selegiline | Adjunct for wearing off; generates amphetamine metabolites (anxiety, insomnia); MAO-B selectivity lost at >30-40 mg/day |
| Safinamide | Adjunct to levodopa for "off" periods; reversible MAO-B inhibition + inhibits glutamate release (dual mechanism) |
E. Amantadine
Originally an antiviral, accidentally found to have antiparkinsonian effects. Triple mechanism:
- Increases presynaptic dopamine release
- Blocks muscarinic (cholinergic) receptors
- Inhibits NMDA glutamate receptors (also reduces levodopa-induced dyskinesias)
Less efficacious than levodopa; tolerance develops more quickly. Adverse effects: restlessness, agitation, confusion, hallucinations, orthostatic hypotension, urinary retention, peripheral edema, livedo reticularis.
F. Anticholinergics (Antimuscarinics)
Correct the dopamine/acetylcholine imbalance by reducing cholinergic tone. Adjuncts only; much less effective than levodopa.
| Drug | Notes |
|---|---|
| Benztropine | Adjuvant; may help tremor more than bradykinesia |
| Trihexyphenidyl | Similar profile |
Adverse effects: dry mouth (xerostomia), constipation, urinary retention, visual blurring, confusion. Contraindicated in glaucoma, prostatic hypertrophy, pyloric stenosis.
G. Adenosine A2A Receptor Antagonist
- Istradefylline - Adjuvant to levodopa/carbidopa to reduce "off" episodes. Mechanism: antagonism of adenosine A2A receptors (which are co-localized with D2 receptors in the striatum). Adverse effects: dyskinesias, nausea, constipation, hallucinations, insomnia, impulse control issues.
3. AMYOTROPHIC LATERAL SCLEROSIS (ALS)
The Disease
ALS (Lou Gehrig's disease) involves progressive death of both upper and lower motor neurons, leading to failure of the entire neuromuscular system - limbs, bulbar (speech/swallowing), and respiratory muscles. Average life expectancy from diagnosis is 3-5 years, with death typically from respiratory failure. There is no cure; treatment is largely supportive.
Key pathomechanisms: glutamate excitotoxicity (excess glutamate → NMDA receptor overactivation → calcium influx → neuronal death), oxidative stress, and in familial ALS, SOD1 gene mutations.
ALS Drugs
1. Riluzole (Rilutek) - First-Line
Mechanism: Sodium channel blocker that reduces glutamate release, thereby limiting excitotoxicity in motor neurons.
Effect: Modestly prolongs survival (~2-3 months); does NOT reverse or halt disease.
Adverse effects: Elevated hepatic enzymes (monitor LFTs), asthenia, nausea, dizziness.
2. Edaravone (Radicava)
Mechanism: Free radical scavenger / antioxidant - reduces oxidative stress-induced neuronal damage.
Indication: Approved for early ALS to slow functional decline.
Administration: IV infusion (initial and subsequent cycles); oral suspension also available.
3. Sodium Phenylbutyrate + Taurursodiol (Relyvrio / AMX0035)
A combination drug that protects neurons from endoplasmic reticulum stress and mitochondrial dysfunction. Showed clinical benefit in one phase 2/3 trial.
4. Tofersen (Qalsody) - Gene-Targeted
Mechanism: Antisense oligonucleotide (ASO) that reduces SOD1 protein production. Only for SOD1-mutation ALS (familial ALS subset).
5. Symptomatic/Supportive Treatments
- Spasticity: Baclofen (GABA-B agonist), tizanidine. Dantrolene is contraindicated in ALS - it acts directly on skeletal muscle to impair Ca2+ release from sarcoplasmic reticulum and would worsen muscular weakness (though it is useful in malignant hyperthermia and stroke/SCI spasticity).
- Sialorrhea (drooling): Anticholinergics, botulinum toxin
- Respiratory support: Non-invasive positive pressure ventilation (NIPPV)
- Nutrition: Percutaneous endoscopic gastrostomy (PEG) tube
4. HUNTINGTON'S DISEASE (HD)
The Disease
HD is an autosomal dominant disorder caused by a CAG trinucleotide repeat expansion in the HTT gene (chromosome 4), encoding an abnormal huntingtin protein. The hallmark is progressive loss of medium spiny neurons in the striatum, particularly those forming the indirect pathway (projecting to the globus pallidus externa, GPe). This disinhibits the thalamus, producing the characteristic choreiform (involuntary dance-like) movements.
As the disease progresses, dementia and psychiatric symptoms (depression, irritability, psychosis) dominate. No disease-modifying treatment exists - all therapies are symptomatic.
HD Drugs
1. VMAT2 Inhibitors - For Chorea
These deplete presynaptic catecholamine (dopamine) stores, reducing the excess dopaminergic drive that causes involuntary movements.
| Drug | Notes |
|---|---|
| Tetrabenazine (Xenazine) | Reversible VMAT2 inhibitor; starting dose 12.5 mg/day; metabolized by CYP2D6 (genotyping recommended if >50 mg/day); causes depression with suicidality and parkinsonism as side effects |
| Deutetrabenazine (Austedo) | Deuterated form - stronger C-D bonds increase half-life of active metabolites; similar efficacy and side effects but potentially lower risk of depression |
| Valbenazine (Ingrezza) | Primarily approved for tardive dyskinesia but used in HD chorea |
2. Antipsychotics - For Psychiatric Symptoms and Chorea
Used at lower doses than in primary psychiatric disorders. Haloperidol, risperidone, quetiapine. However, these agents impair cognition and mobility - risks must be weighed carefully.
3. Antidepressants
SSRIs and SNRIs for depression and irritability in HD. Avoid drugs with significant anticholinergic profiles - they can worsen chorea.
4. Benzodiazepines
For anxiety and choreiform movements.
Note on Disease-Modifying Research
Gene-silencing approaches (ASOs targeting HTT mRNA, RNA interference) are under active clinical investigation. The HTT gene's discovery means this is one of the most tractable targets in neurodegeneration for future therapy.
5. MULTIPLE SCLEROSIS (MS)
The Disease
MS is an autoimmune, demyelinating neurodegenerative disease in which T lymphocytes attack the myelin sheath of CNS axons (the BBB breakdown allows lymphocyte infiltration). Lesion plaques in white matter disrupt nerve conduction. The disease can be:
- Relapsing-remitting MS (RRMS): Episodic attacks with recovery between them (most common)
- Secondary progressive MS (SPMS): Steady worsening after initial RRMS
- Primary progressive MS (PPMS): Steady progression from onset (harder to treat)
MS Drugs - Disease-Modifying Therapies (DMTs)
1. Injectable Interferons and Glatiramer
| Drug | Mechanism | Route | Key Adverse Effects |
|---|---|---|---|
| Interferon beta-1a (Avonex, Rebif) | Immunomodulatory; reduces demyelinating inflammation | IM/SC injection | Flu-like symptoms, depression, elevated liver enzymes, injection site reactions |
| Interferon beta-1b (Betaseron) | Same class | SC injection | Same as above |
| Glatiramer acetate (Copaxone) | Synthetic myelin-like polypeptide; acts as decoy to T-cell attack | SC injection | Post-injection reaction: flushing, chest pain, anxiety, itching (self-limiting) |
2. Sphingosine-1-Phosphate (S1P) Receptor Modulators (Oral)
These drugs trap lymphocytes in lymph nodes, preventing them from reaching the CNS.
| Drug | Notes |
|---|---|
| Fingolimod (Gilenya) | First oral MS drug; causes first-dose bradycardia (6-hour cardiac monitoring required); risk of macular edema, PML, opportunistic infections |
| Siponimod (Mayzent) | Requires CYP2C9 genotyping before use; CYP2C9*3/*3 genotype = absolute contraindication; for SPMS |
| Ozanimod (Zeposia) | CYP2C8 substrate; avoid with strong CYP2C8 inducers/inhibitors |
| Ponesimod (Ponvory) | Similar mechanism; once daily oral |
3. Pyrimidine Synthesis Inhibitor
- Teriflunomide (Aubagio) - Inhibits DHODH enzyme in lymphocyte pyrimidine synthesis, reducing active lymphocytes in the CNS. Can elevate liver enzymes. Teratogenic - absolutely contraindicated in pregnancy (very long half-life; cholestyramine washout required if pregnancy is desired).
4. Nrf2 Activators / Fumarates (Oral)
| Drug | Notes |
|---|---|
| Dimethyl fumarate (Tecfidera) | Activates Nrf2 antioxidant pathway; flushing, GI upset common; risk of PML and lymphopenia |
| Diroximel fumarate (Vumerity) | Better GI tolerability than dimethyl fumarate |
| Monomethyl fumarate (Bafiertam) | Similar mechanism |
5. Monoclonal Antibodies (High-Efficacy DMTs)
| Drug | Target | Notes |
|---|---|---|
| Natalizumab (Tysabri) | Anti-VLA-4 (alpha-4 integrin) | Blocks lymphocyte entry into CNS; risk of PML (JC virus reactivation) - test JCV antibody index before use |
| Alemtuzumab (Lemtrada) | Anti-CD52 | Depletes lymphocytes; associated with serious autoimmune disorders (thyroid disease, ITP, nephropathy); reserved for active RRMS |
| Ocrelizumab (Ocrevus) | Anti-CD20 (B cells) | First drug approved for PPMS; also used in RRMS; infusion reactions common |
| Ofatumumab (Kesimpta) | Anti-CD20 | Subcutaneous self-injection option |
| Rituximab | Anti-CD20 | Off-label use; widely used |
| Ublituximab (Briumvi) | Anti-CD20 | Newest; shorter infusion time |
6. Drugs for ALS in the MS Section (as per textbook table)
Lippincott's pharmacology groups riluzole and edaravone together with MS drugs under "neurodegenerative disease" treatments.
7. Acute Relapse Treatment
- High-dose IV methylprednisolone (e.g., 1 g/day x 3-5 days) - shortens relapse duration but does not affect long-term disability. Oral prednisone after IV is optional.
Summary Table: Key Mechanisms at a Glance
| Disease | Core Pathology | Primary Drug Mechanism |
|---|---|---|
| Alzheimer's | Aβ plaques, tau tangles, cholinergic loss | AChE inhibition; NMDA blockade; Anti-Aβ immunotherapy |
| Parkinson's | Dopaminergic SNc neuron loss; Lewy bodies | DA precursor (levodopa); DA agonists; MAO-B inhibition; COMT inhibition |
| ALS | UMN + LMN death; glutamate excitotoxicity | Glutamate release inhibition (riluzole); ROS scavenging (edaravone) |
| Huntington's | Striatal neuron loss; mutant huntingtin | VMAT2 inhibition (tetrabenazine) to reduce chorea |
| MS | Autoimmune demyelination | Immunomodulation (IFN-beta); lymphocyte sequestration (S1P); B-cell depletion (anti-CD20) |
Recent Evidence (2024-2026)
A 2025 network meta-analysis in BMC Medicine (PMID 40189519) found that GLP-1 receptor agonists (like semaglutide) and SGLT2 inhibitors show prophylactic benefits across neurodegenerative diseases - a potentially exciting new frontier beyond current drug classes. A 2024 systematic review (PMID 39666629) confirmed rivastigmine improves gait in PD dementia patients.
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics (Tables 21-23)
- Lippincott Illustrated Reviews: Pharmacology
- Stahl's Essential Psychopharmacology (Chapters 12-13)
- Bradley and Daroff's Neurology in Clinical Practice
- Goldman-Cecil Medicine
Dopaminergic drugs in detail pharmacology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have everything needed for a comprehensive, textbook-grounded answer. Let me compile it.
Dopaminergic Drugs - Deep Pharmacology
Part 1: Dopamine - The Neurotransmitter
Structure and Synthesis
Dopamine (3,4-dihydroxyphenylethylamine) is a catecholamine neurotransmitter and the immediate metabolic precursor of norepinephrine (NE) and epinephrine (EPI). Its synthesis in dopaminergic nerve terminals follows two enzymatic steps:
L-Tyrosine → (Tyrosine Hydroxylase, TH) → L-DOPA → (Aromatic Amino Acid Decarboxylase, AADC) → Dopamine
- Tyrosine Hydroxylase (TH) is the rate-limiting enzyme - the key regulatory point
- After synthesis, dopamine is packaged into storage vesicles by VMAT2 (Vesicular Monoamine Transporter 2)
- Release is by exocytosis
- Reuptake occurs via the DAT (Dopamine Transporter) and, to a lesser extent, the NET (norepinephrine transporter)
- Metabolism: Cytosolic DA → degraded by MAO + ALDH → and by COMT in non-neuronal cells → final metabolite is HVA (homovanillic acid)
Part 2: Dopamine Receptors - Full Classification
There are 5 dopamine receptor subtypes (D1-D5), all G protein-coupled receptors (GPCRs), organized into two families:
D1-Like Family (D1 and D5)
- G protein: Gs → activates adenylyl cyclase → increases cAMP
- Located postsynaptically on dopamine-receptive cells
- D1: Chromosome 5; high density in striatum (caudate-putamen), nucleus accumbens, olfactory tubercle, frontal cortex. Critical for motor control, reward, and cognition.
- D5: Chromosome 4; found in hippocampus and hypothalamus; lower expression
D2-Like Family (D2, D3, D4)
- G protein: Gi → inhibits adenylyl cyclase → decreases cAMP; also inhibits calcium channels and opens potassium channels (hyperpolarization)
- Located both pre- and postsynaptically
- D2: Chromosome 11; high density in striatum, nucleus accumbens, olfactory tubercle. The primary therapeutic target for antipsychotics and dopamine agonists. D2-short (presynaptic autoreceptor) and D2-long (postsynaptic) variants from alternative splicing.
- D3: Chromosome 11; limbic areas, especially nucleus accumbens shell. Also acts as autoreceptor. Target for some PD drugs (pramipexole is D3-preferring).
- D4: Lowest expression in the brain; frontal cortex, amygdala, hippocampus. Present in the retina.
D1 (stimulatory) and D2 (inhibitory) receptor subtypes in the striatum form the basis of the direct and indirect pathway of basal ganglia circuitry (see diagram below).
Part 3: The Major Dopaminergic Pathways in the CNS
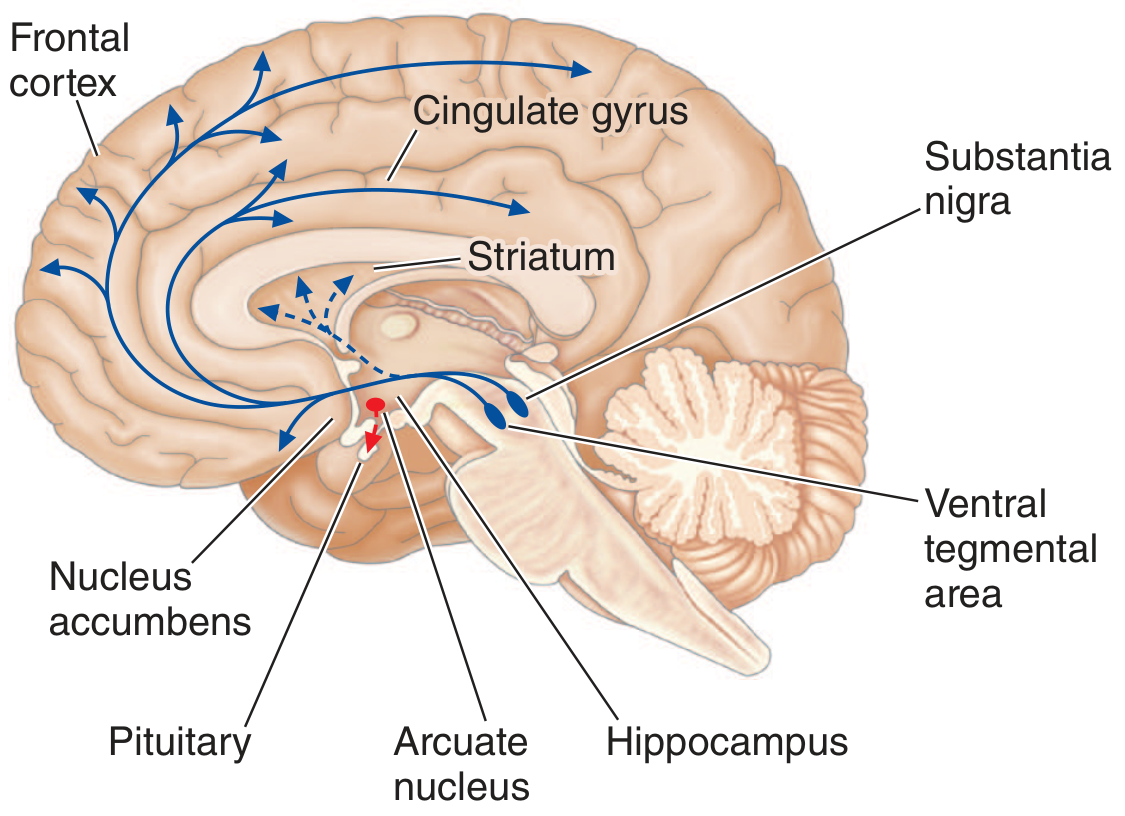
There are 3 major dopaminergic projection systems (plus 2 minor ones):
| Pathway | Origin | Target | Function | Disease When Dysregulated |
|---|---|---|---|---|
| Nigrostriatal | Substantia nigra pars compacta (SNpc) | Dorsal striatum (caudate + putamen) | Voluntary movement coordination | Parkinson's disease; antipsychotic-induced EPS |
| Mesolimbic | Ventral tegmental area (VTA) | Nucleus accumbens, amygdala, hippocampus | Reward, motivation, emotions | Addiction, schizophrenia, bipolar depression |
| Mesocortical | VTA | Prefrontal cortex | Cognition, impulse control, "higher-order" thinking | Schizophrenia (negative/cognitive symptoms), ADHD |
| Tuberoinfundibular | Arcuate nucleus (hypothalamus) | Anterior pituitary (via portal blood) | Inhibits prolactin secretion via D2 receptors | Hyperprolactinemia when blocked |
| Medullary-periventricular | Motor nucleus of vagus | Not fully mapped | Eating behavior | - |
Part 4: Basal Ganglia Circuit - Direct vs. Indirect Pathway
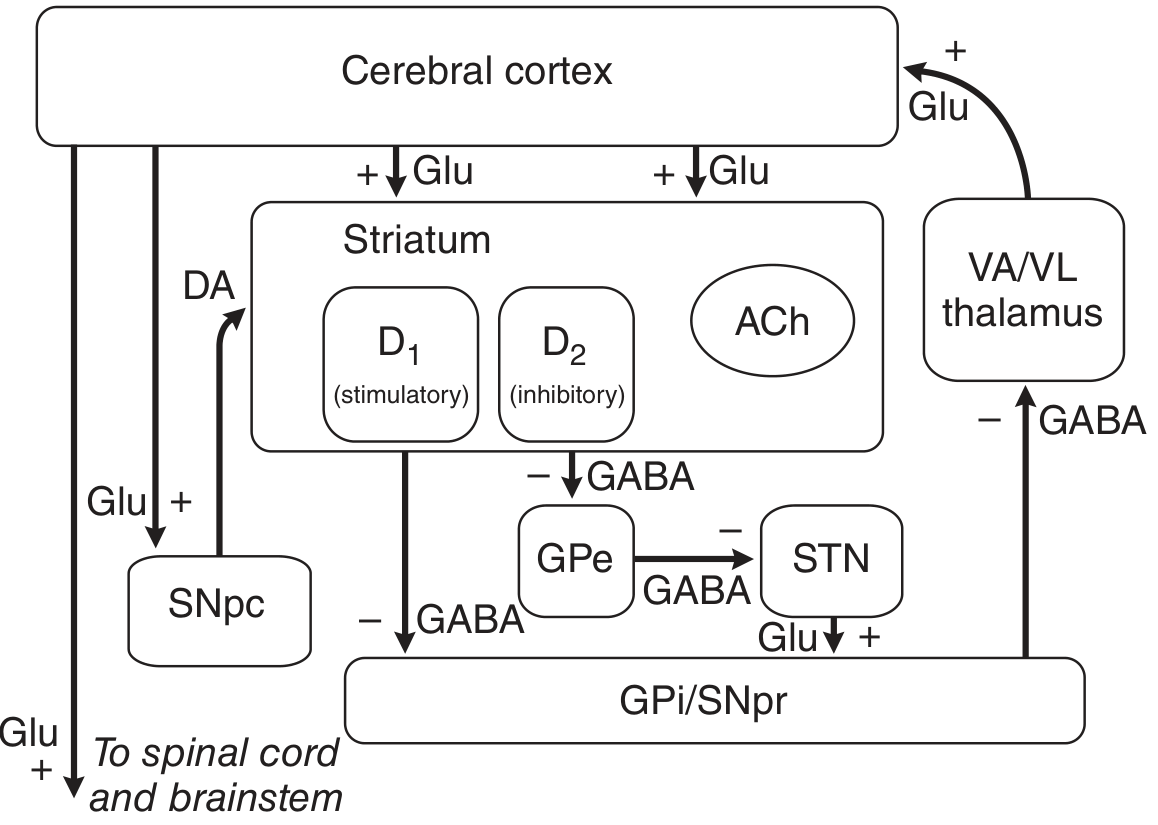
This is fundamental to understanding why dopaminergic drugs work in Parkinson's disease:
Normal State
- Cortex sends glutamate (excitatory) to the striatum
- SNpc sends dopamine to both D1 and D2 receptor-bearing striatal neurons
- Direct pathway (D1): Striatum → SNpr/GPi via GABA (inhibitory). D1 activation stimulates this pathway → net disinhibition of thalamus → motor facilitation
- Indirect pathway (D2): Striatum → GPe → STN → SNpr/GPi. D2 activation inhibits this pathway → also leads to disinhibition of thalamus → motor facilitation
- Net effect of dopamine: facilitates movement through both pathways
In Parkinson's Disease (Loss of SNpc dopamine)
- Direct pathway becomes less active (D1 under-stimulated)
- Indirect pathway becomes overactive (D2 under-stimulated = loss of inhibition)
- Result: GPi/SNpr overactive → excessive inhibition of VA/VL thalamus → reduced cortical excitation → bradykinesia, rigidity, tremor
Part 5: Dopaminergic Drug Classes - Full Pharmacology
CLASS 1: DOPAMINE PRECURSOR - Levodopa + Carbidopa
Levodopa
Why not dopamine directly? Dopamine cannot cross the blood-brain barrier (BBB). Levodopa crosses via a membrane transporter for aromatic amino acids, then is converted to dopamine by AADC primarily within presynaptic terminals of dopaminergic neurons in the striatum.
The problem without carbidopa:
- Without a peripheral AADC inhibitor, >99% of oral levodopa is decarboxylated in gut mucosa and peripheral tissues
- Only ~1% reaches the CNS
- Peripheral DA causes severe nausea, vomiting, orthostatic hypotension
Pharmacokinetics of levodopa:
- Oral absorption: peaks 0.5-2 hours after dose
- Plasma t½: very short - 1-3 hours
- Absorption influenced by: gastric emptying rate, gastric pH, exposure to degradative enzymes in gut mucosa
- High-protein meals delay absorption (aromatic amino acids compete for the same intestinal transporter)
- Enters CNS via aromatic amino acid transporter
- Metabolized by AADC, COMT, and MAO → final products include HVA and 3-O-methyl DOPA
Carbidopa
- Peripheral AADC inhibitor (aromatic amino acid decarboxylase inhibitor)
- Cannot cross the BBB - this is the key pharmacological feature
- Blocks peripheral conversion of levodopa → dopamine
- Result: increased fraction of levodopa available to cross BBB; reduces peripheral dopamine-related side effects (nausea, hypotension)
- A daily dose of 75 mg carbidopa is generally sufficient to prevent nausea
- Most common formulation: carbidopa/levodopa 25/100 (25 mg carbidopa + 100 mg levodopa)
Motor Complications of Long-Term Levodopa Therapy
| Complication | Mechanism | Management |
|---|---|---|
| Wearing-off | Short plasma t½ + progressive loss of surviving nerve terminals that buffer drug | Increased dose frequency; add COMT inhibitor; ER formulations |
| Dyskinesias | Pulsatile (non-physiological) D1/D2 stimulation → abnormal plasticity | Amantadine; reduce levodopa dose; add DA agonist |
| On/off phenomenon | Unpredictable fluctuation; buffering capacity lost | Continuous dopaminergic stimulation (DA agonist, intestinal gel pump) |
CLASS 2: DOPAMINE RECEPTOR AGONISTS (DAs)
These drugs directly activate dopamine receptors - they do not need to be converted. They are more selective and have longer half-lives than levodopa, producing more continuous (less pulsatile) stimulation, which reduces motor complications.
Non-Ergot DAs (Preferred - no fibrotic risk)
| Drug | Receptor Selectivity | t½ | Key Pharmacology |
|---|---|---|---|
| Pramipexole | D3 > D2 (D2-class preferring) | 8-12 h | Renally excreted unchanged; reduce dose in renal impairment; IR (TID) or ER (once daily) |
| Ropinirole | D2-class selective | 6 h | Hepatically metabolized (CYP1A2); IR (TID) or ER (once daily); no titration concerns with renal impairment |
| Rotigotine | D1 + D2 agonist (broadest spectrum) | ~5-7 h (patch delivers continuously) | Transdermal patch; continuous drug delivery avoids peak-trough fluctuations; useful in dysphagia patients |
| Apomorphine | D1/D2 strong agonist | ~40 min | Subcutaneous or sublingual; rescue therapy for acute "off" episodes; highly emetogenic - requires pretreatment with trimethobenzamide (not ondansetron - contraindicated due to hypotension risk with 5HT3 blockade); sublingual form can cause oral mucosal ulcers |
Mechanism in detail (pramipexole/ropinirole):
- Directly activate D2/D3 receptors in the striatum, mimicking dopamine
- D3 receptor activation by pramipexole also provides benefit for restless legs syndrome and may modulate limbic function (also causes impulse control disorders - gambling, hypersexuality)
- As autoreceptor agonists (presynaptic D2/D3), they can also reduce the firing rate and DA synthesis - used clinically at lower doses for RLS
Adverse effects common to all DAs:
- Nausea, vomiting
- Orthostatic hypotension
- Somnolence / sudden sleep attacks (must warn patients not to drive)
- Hallucinations, psychosis (less than levodopa but significant)
- Peripheral edema
- Impulse control disorders (pathological gambling, hypersexuality, compulsive eating/shopping) - more common with DAs than levodopa
- Augmentation of restless legs (with chronic use in RLS)
Ergot-Derived DAs (Generally Avoided Due to Fibrosis Risk)
| Drug | Use | Concern |
|---|---|---|
| Bromocriptine | Hyperprolactinemia, type 2 diabetes (Cycloset), acromegaly | Pleuropulmonary/retroperitoneal fibrosis; valvular heart disease at high doses (via 5HT2B agonism) |
| Cabergoline | Hyperprolactinemia (more effective than bromocriptine) | Same fibrotic risk (5HT2B agonism) - monitor echocardiography; relatively safe at the low doses used for prolactinoma |
Mechanism for hyperprolactinemia: D2 receptors on pituitary lactotrophs tonically inhibit prolactin secretion. Bromocriptine and cabergoline activate these D2 receptors → suppress prolactin → used in prolactinomas and other hyperprolactinemic states.
CLASS 3: COMT INHIBITORS (Catechol-O-Methyltransferase Inhibitors)
Mechanism: COMT is an enzyme that methylates catechols (including levodopa, dopamine, L-DOPA, 3-O-methyl DOPA). Oral levodopa + carbidopa leaves COMT as an important peripheral metabolic pathway. COMT inhibitors block this, increasing levodopa bioavailability (longer plasma t½, more consistent brain levels) and reducing "wearing off."
Key pharmacology of the COMT pathway:
- Peripheral COMT: converts levodopa → 3-O-methyl DOPA (3-OMD), reducing the fraction reaching the CNS
- Central COMT: converts dopamine → 3-methoxytyramine (an inactive metabolite)
| Drug | COMT Selectivity | t½ | Hepatotoxicity | Notes |
|---|---|---|---|---|
| Entacapone | Peripheral COMT only | ~2 h (short) | None | Given with each levodopa dose (multiple times daily); urine discoloration (orange); available in fixed-dose triple combination Stalevo (carbidopa/levodopa/entacapone) |
| Tolcapone | Central + peripheral COMT | Longer | YES - potentially fatal fulminant hepatic failure (3+ deaths reported) | Black-box warning; monitor LFTs every 2 weeks for first year; only use when other therapies fail |
| Opicapone | Peripheral COMT | Short plasma t½ but slow dissociation = once-daily dosing | None reported | Newest; once daily; comparable off-time reduction to entacapone |
CLASS 4: MAO-B INHIBITORS (Monoamine Oxidase B Inhibitors)
Mechanism: Two isoforms of MAO degrade catecholamines:
- MAO-A: preferentially deaminates serotonin, NE, tyramine
- MAO-B: the predominant form in the striatum - responsible for most oxidative metabolism of dopamine in the brain
MAO-B inhibitors reduce DA degradation → preserve dopaminergic tone → improve PD symptoms.
Selective MAO-B inhibitors do not exhibit the "cheese effect" (they do not inhibit peripheral MAO-A, so tyramine from food is still metabolized normally).
| Drug | Selectivity | Reversibility | Key Features |
|---|---|---|---|
| Selegiline | MAO-B selective (at normal doses; selectivity lost at >30-40 mg/day) | Irreversible | Metabolized to L-amphetamine and L-methamphetamine metabolites → anxiety, insomnia; ODT and transdermal patch formulations reduce first-pass metabolism and limit amphetamine generation; adjunct for wearing off |
| Rasagiline | MAO-B selective | Irreversible | No amphetamine metabolites (major advantage over selegiline); metabolized by CYP1A2 - inhibitors of CYP1A2 (e.g., ciprofloxacin, fluvoxamine) can double plasma concentrations; monotherapy in early PD or adjunct in advanced PD; possible disease-modifying effect (TEMPO/ADAGIO trials - early vs. delayed start); multiple drug interactions - avoid meperidine (risk of serotonin syndrome) |
| Safinamide | MAO-B selective | Reversible | Dual mechanism: MAO-B inhibition + inhibits glutamate release (sodium channel blockade); adjunct to levodopa for "off" periods; reversibility means lower risk of drug interactions than irreversible inhibitors |
Drug interactions (critical for all MAO-B inhibitors):
- Meperidine (pethidine): Risk of serotonin syndrome - absolute contraindication
- SSRIs/SNRIs/TCAs: Risk of serotonin syndrome - use with caution
- Sympathomimetics: Risk of hypertensive crisis (less with selective MAO-B inhibitors)
- Tramadol, dextromethorphan: Serotonin syndrome risk
CLASS 5: DOPAMINE PRECURSOR SYNTHESIS ENHANCERS / RELEASER
Amantadine
Originally an antiviral (anti-influenza), with accidental discovery of antiparkinsonian activity.
Triple mechanism of action:
- Increases presynaptic dopamine release from surviving terminals
- Blocks muscarinic (M1) cholinergic receptors - corrects DA/ACh imbalance
- Non-competitive NMDA glutamate receptor antagonist - reduces excitotoxicity AND is the main mechanism for reducing levodopa-induced dyskinesias
Pharmacokinetics:
- Oral bioavailability ~90%
- Renally excreted unchanged (dose-reduce in renal impairment)
- t½: ~10-14 hours
Adverse effects:
- Livedo reticularis (mottled purplish skin - hallmark side effect)
- Peripheral edema (ankle swelling)
- Restlessness, agitation, confusion, hallucinations, acute toxic psychosis (at high doses)
- Orthostatic hypotension, urinary retention, dry mouth
- Tolerance develops with chronic use
Extended-release amantadine (Gocovri): Specifically FDA-approved for levodopa-induced dyskinesias - taken once daily at bedtime (ER formulation).
CLASS 6: ADENOSINE A2A RECEPTOR ANTAGONIST
Istradefylline
Mechanism (indirect dopaminergic):
- A2A receptors are highly co-localized with D2 receptors in the striatum (especially on indirect pathway neurons)
- Activation of A2A receptors inhibits D2 receptor signaling, possibly via A2A-D2 heterodimer formation
- By antagonizing A2A receptors, istradefylline boosts dopamine (D2) signaling in the striatum even without directly activating D2
- Effectively increases "off-time" to "on-time" ratio when used with levodopa
Indication: Adjunct to levodopa/carbidopa for motor fluctuations ("off" episodes)
Dose: Once daily
Adverse effects: Dyskinesias, nausea, constipation, hallucinations, insomnia, impulse control disorders
CLASS 7: ANTICHOLINERGICS (INDIRECT DOPAMINERGIC EFFECT)
These do not act on dopamine receptors but work by correcting the dopamine/acetylcholine imbalance in the striatum. When dopamine is deficient, striatal cholinergic interneurons become relatively overactive. Anticholinergics reduce this.
| Drug | Notes |
|---|---|
| Benztropine (Cogentin) | Antimuscarinic; useful for tremor and drug-induced Parkinsonism |
| Trihexyphenidyl (Artane) | Similar; also useful for acute dystonia |
| Diphenhydramine | Antihistamine with antimuscarinic properties; used in acute drug-induced EPS |
Key adverse effects: Dry mouth, constipation, urinary retention, blurred vision, confusion, memory impairment (avoid in elderly). Contraindicated in angle-closure glaucoma, BPH, pyloric stenosis.
CLASS 8: ERGOT-DERIVED DA AGONISTS (Pituitary-Specific Use)
As detailed above, bromocriptine and cabergoline primarily target D2 receptors on pituitary lactotrophs. Worth noting additional uses:
- Bromocriptine (Cycloset): FDA-approved for type 2 diabetes - activates hypothalamic dopaminergic activity, which modulates circadian regulation of insulin sensitivity. Taken within 2 hours of waking.
- Quinagolide: D2 agonist used in Europe for hyperprolactinemia.
Part 6: Peripheral Dopaminergic Pharmacology
Dopamine as a Vasopressor (IV use in shock/critical care)
DA itself does not cross the BBB when given IV - its effects in critical care are entirely peripheral:
| Dose Range | Predominant Receptor | Effect |
|---|---|---|
| Low (<3 mcg/kg/min) | D1 receptors in renal, mesenteric, coronary beds | Vasodilation; increased GFR, renal blood flow, natriuresis |
| Moderate (3-10 mcg/kg/min) | β1 adrenergic receptors (+ NE release from nerve terminals) | Positive inotropy, increased cardiac output |
| High (>10 mcg/kg/min) | α1 adrenergic receptors | Vasoconstriction, increased SVR |
Critical note: Dopamine is a substrate for both MAO and COMT, making it inactive orally.
Fenoldopam
- Selective D1 receptor agonist (no α or β activity)
- Used IV for hypertensive emergencies - causes renal and mesenteric vasodilation
- Increases GFR and natriuresis (renal protective in some settings)
- Does not cross BBB
Part 7: Drug Interactions Summary
| Drug | Interacting Agent | Mechanism | Consequence |
|---|---|---|---|
| Levodopa | High-protein diet | Aromatic amino acids compete for intestinal and BBB transporter | Reduced absorption and CNS entry |
| Levodopa | Antipsychotics (D2 blockers) | D2 receptor blockade in striatum | Worsens parkinsonism |
| MAO-B inhibitors | Meperidine, SSRIs | Serotonin accumulation | Serotonin syndrome |
| MAO-B inhibitors | Tyramine foods | MAO-B inhibitors alone: minimal risk (MAO-A intact) | "Cheese effect" generally absent at selective doses |
| DA agonists | 5HT3 antagonists (apomorphine) | Profound hypotension | Contraindicated |
| COMT inhibitors | Tolcapone + any hepatotoxin | Additive hepatotoxicity | Monitor LFTs closely |
| Carbidopa | Pyridoxine (Vitamin B6) | B6 is cofactor for AADC - enhances peripheral levodopa metabolism (negates carbidopa) | Loss of therapeutic effect if pyridoxine given without carbidopa |
Quick Reference: Mechanism at the Synaptic Level
[Presynaptic terminal]
Tyrosine → L-DOPA → Dopamine (stored in vesicles via VMAT2)
↓ Exocytosis (depolarization)
[Synaptic cleft]
↓
Postsynaptic D1 (Gs→↑cAMP) or D2 (Gi→↓cAMP) receptors
↓
Presynaptic D2/D3 autoreceptors (feedback inhibition of synthesis/release)
↓
Reuptake via DAT → MAO/ALDH degradation → HVA
COMT in non-neuronal cells → 3-methoxytyramine → HVA
Drugs targeting each step:
- Synthesis enhancement: levodopa (substrate loading)
- VMAT2 inhibition: tetrabenazine (depletes DA)
- Direct receptor agonism: pramipexole, ropinirole, rotigotine
- Reuptake inhibition: cocaine, methylphenidate (not therapeutic in PD)
- MAO-B inhibition: selegiline, rasagiline, safinamide
- COMT inhibition: entacapone, tolcapone, opicapone
- DA release enhancement: amantadine
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Chapters 14, 15, 21
- Katzung's Basic and Clinical Pharmacology 16e, Chapter 29
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- Lippincott Illustrated Reviews: Pharmacology, Chapter 15
This is a shared conversation. Sign in to Orris to start your own chat.