Mitral regurgitation
Reading File
Finding Sources
Searching PubMed
"mitral regurgitation"[MeSH Terms] AND management
Reading File
Searching PubMed
"mitral regurgitation"[MeSH Terms] AND ("valve repair" OR "transcatheter")
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive review of mitral regurgitation (MR) based on authoritative cardiology and surgical textbooks.
Mitral Regurgitation (MR)
Definition and Overview
Mitral regurgitation is the backward flow of blood from the left ventricle (LV) into the left atrium (LA) during systole due to incompetent closure of the mitral valve. Unlike mitral stenosis (which is primarily rheumatic), MR results from dysfunction of any component of the complex mitral apparatus: the leaflets, chordae tendineae, papillary muscles, annulus, or left ventricle itself.
- Braunwald's Heart Disease, 10th Ed.
Classification
MR is divided into two major categories:
1. Primary (Organic/Degenerative) MR
Intrinsic disease of the mitral valve leaflets:
- Mitral valve prolapse (MVP) - most common cause for mitral valve replacement in the developed world
- Rheumatic heart disease
- Infective endocarditis
- Fibromuscular dysplasia
- Connective tissue disorders (Marfan syndrome, Ehlers-Danlos)
2. Secondary (Functional/Ischemic) MR
The valve leaflets are structurally normal, but regurgitation occurs due to:
- LV dilatation (dilated cardiomyopathy) causing mitral annular dilatation
- Ischemic MR - apical displacement of papillary muscles in infarcted or ischemic myocardium, causing leaflet tethering and poor coaptation
- Atrial fibrillation causing annular dilatation
About 75% of patients with heart failure and reduced ejection fraction have some degree of secondary MR; it is severe in ~20%.
- Goldman-Cecil Medicine, 26th Ed.
- Symptom to Diagnosis, 4th Ed.
Pathophysiology
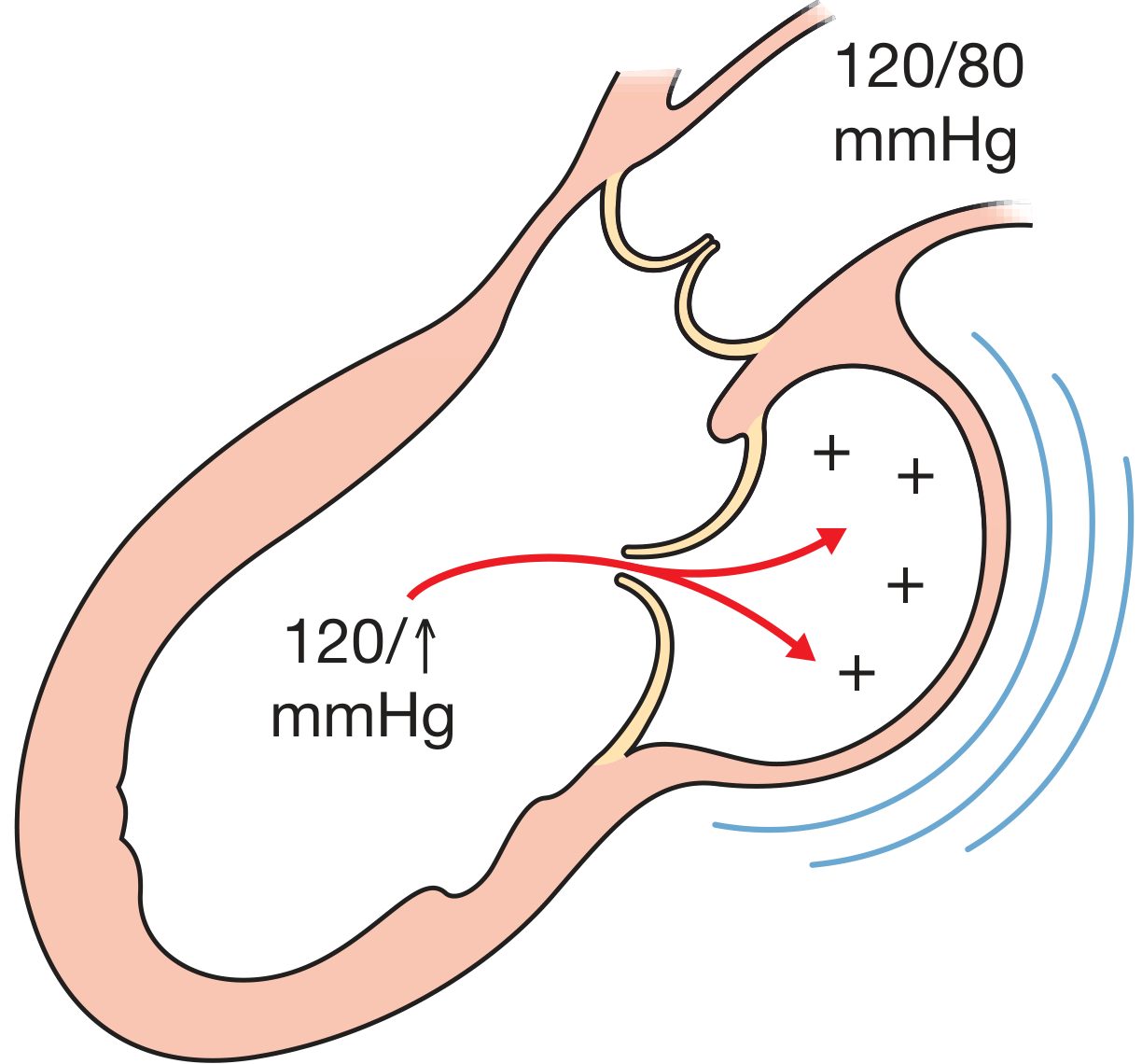
Figure: Features and pathophysiology of mitral regurgitation. The LV ejects blood both forward (into the aorta at 120/80 mmHg) and backward into the LA, raising LA pressure.
Compensated (Chronic) MR
- Regurgitation reduces LV afterload, so ejection fraction is initially normal to high
- LA and LV gradually dilate to accommodate the volume overload
- LV end-systolic volume remains low
- Patient may remain asymptomatic for years (average 16 years from diagnosis to symptoms)
Decompensated MR
- Systolic function eventually fails
- LV end-systolic volume increases, stroke volume falls, and EF declines
- Important caveat: An EF of 55% in severe MR may represent substantial systolic dysfunction (the regurgitant volume artificially inflates EF)
- LV dysfunction at this stage may be irreversible
Acute MR (e.g., papillary muscle rupture post-MI, acute endocarditis)
-
No time for compensatory chamber changes
-
Sudden severe LA pressure elevation
-
Presents with flash pulmonary edema and cardiogenic shock
-
Poorly tolerated and a surgical emergency
-
Symptom to Diagnosis, 4th Ed.; Goldman-Cecil Medicine
Clinical Features
Symptoms
- Chronic MR: Often asymptomatic for many years; progresses to fatigue, exertional dyspnea, orthopnea, palpitations
- Acute MR: Severe dyspnea, tachycardia, pulmonary edema; cardiogenic shock may develop rapidly
- Annual mortality in severe MR is approximately 5%
Physical Examination
| Finding | Details |
|---|---|
| Murmur | Holosystolic (pansystolic), blowing, best heard at the apex, radiates to the axilla |
| Murmur grading | Grade 3+ correlates with moderate-severe MR (Sensitivity 85%, Specificity 81%; LR+ 4.5, LR- 0.2) |
| S1 | Soft or inaudible |
| S2 | Physiologically split; followed by S3 in severe MR (reflects rapid LV filling, not necessarily heart failure) |
| Apex beat | Heaving, displaced downward and to the left (LV dilatation) |
| Acute MR | Murmur may be short or absent (rapid LA-LV pressure equalization) |
- Goldman-Cecil Medicine; Symptom to Diagnosis 4th Ed.
ECG
- Left atrial enlargement (bifid P waves - "P mitrale")
- Left ventricular hypertrophy
- Atrial fibrillation (common with LA dilatation)
Chest X-ray
- Cardiomegaly (LA and LV enlargement)
- Prominent pulmonary vasculature
- Absence of cardiomegaly suggests mild or non-chronic MR
Echocardiographic Features
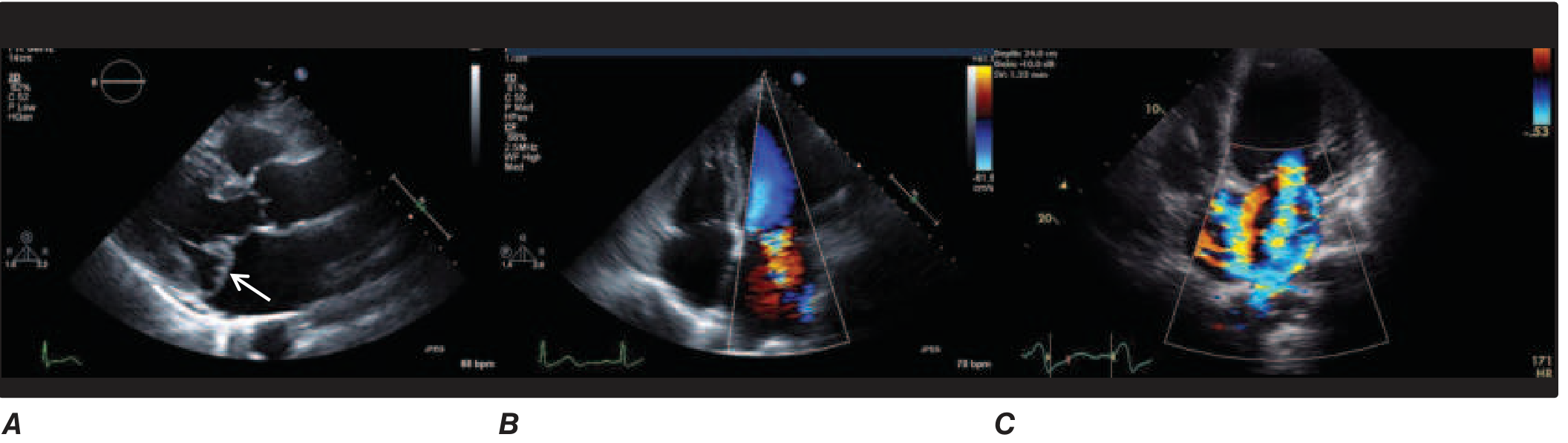
A. Mitral valve prolapse with posterior leaflet prolapsing behind the anterior leaflet. B. Color-flow Doppler showing the MR jet (MVP). C. Severe functional/secondary MR with a large central jet in a dilated LV.
- TTE (Transthoracic echocardiography): Test of choice for diagnosis and quantification of MR
- Color-flow Doppler: Visualizes the regurgitant jet; distinguishes mild from severe MR
- 3D echocardiography: Provides additional pathoanatomic detail for surgical planning
- TEE (Transesophageal echocardiography): More precise valve anatomy; determines feasibility of repair vs replacement
- CMR (Cardiac MRI): Directly quantifies regurgitant volume when echo is inadequate
Monitoring intervals:
-
Mild MR: Echo every 3-5 years
-
Moderate-severe MR: Echo every 6-12 months or sooner with new symptoms
-
Harrison's Principles, 22nd Ed.; Symptom to Diagnosis 4th Ed.
Management
Medical Management
- No proven medical therapy slows progression of primary MR or delays surgery
- Secondary MR with HF: Treat the underlying heart failure aggressively - ACEi/ARB, beta-blockers, sacubitril/valsartan (superior to valsartan alone for reducing secondary MR)
- Cardiac resynchronization therapy (CRT): For HFrEF with LBBB - can improve systolic function and sometimes eliminate secondary MR
- Rate/rhythm control for atrial fibrillation
Surgical Indications (Primary MR)
Surgery is reserved for severe primary MR in the following settings:
| Category | Indication |
|---|---|
| Symptomatic patients | Dyspnea, orthopnea, fatigue |
| Asymptomatic with LV dysfunction | EF <60% OR LV end-systolic diameter >40 mm |
| Asymptomatic, normal LV function | High likelihood of successful repair (repair risk <1%) |
| Any severity | Concurrent cardiac surgery planned for another reason |
Early surgery (before thresholds are reached) is appropriate when repair is highly likely, since survival is normal after successful repair performed before LV dysfunction develops.
- Goldman-Cecil Medicine; Bailey and Love's Surgery 28th Ed.
Surgical Options
1. Mitral Valve Repair (Preferred)
- Preferred over replacement whenever feasible
- Restores valve competence and preserves the subvalvular apparatus
- No prosthesis-related risks (no lifelong anticoagulation needed)
- Substantially lower operative mortality vs replacement (2% vs 6%)
- Better postoperative EF and lower endocarditis risk
- Currently ~70% of US mitral surgeries are valve repairs
- Most applicable for posterior chordal rupture (MVP); anterior and rheumatic lesions are more challenging
2. Mitral Valve Replacement with Apparatus Preservation
- Prosthetic valve inserted while maintaining chordae-papillary muscle continuity
- Preserves LV geometry and function
- Operative mortality ~2x that of repair
3. Mitral Valve Replacement without Apparatus Preservation
- Required when repair is not feasible (severe rheumatic deformity)
- Destruction of the apparatus causes a permanent fall in LV function and EF
- Carries all prosthesis-related risks (thromboembolism, endocarditis, structural failure)
Transcatheter Approaches
-
MitraClip (edge-to-edge repair): Replicates the Alfieri stitch, creating a double-orifice mitral valve via transseptal approach; FDA-approved for:
- High surgical risk patients with primary (degenerative) MR
- Heart failure with secondary MR despite optimal medical therapy
-
Less invasive than surgery but less effective - typically leaves mild-moderate residual MR
-
Based on EVEREST II (vs surgery in primary MR) and COAPT trial (survival benefit in secondary MR)
-
Transcatheter MVR: Still experimental; used primarily in severe mitral annular calcification
-
Braunwald's Heart Disease; Goldman-Cecil Medicine
Secondary (Ischemic) MR - Special Considerations
| Severity | Recommended Approach |
|---|---|
| Severe ischemic MR | Valve repair or chordal-sparing replacement (equivalent outcomes at 1-2 years; replacement results in less residual MR and fewer HF events) |
| Moderate ischemic MR + concurrent CABG | Repair with CABG; repair alone does not clearly add benefit over CABG alone |
| Secondary MR + HF | Medical therapy (sacubitril/valsartan, CRT) first; percutaneous repair if persistent; 5-year survival ~50% |
Complications of MR
- Pulmonary edema (acute or decompensated)
- Atrial fibrillation (LA dilatation)
- Pulmonary hypertension
- Right heart failure (RV dysfunction from chronic pulmonary hypertension)
- Irreversible LV systolic dysfunction
- Sudden cardiac death
Key Takeaway Points
- MR is a disease of the entire mitral apparatus, not just the leaflets
- Primary MR (leaflet disease, e.g., MVP) vs secondary MR (LV/atrial dysfunction) have different mechanisms and management
- EF is an unreliable marker in severe MR because regurgitation artificially elevates it; an EF of 55-60% may already represent significant dysfunction
- Echocardiography is the cornerstone of evaluation and surveillance
- Valve repair is strongly preferred over replacement whenever technically feasible
- In secondary MR, treat heart failure first (sacubitril/valsartan, CRT) before considering intervention
This is a shared conversation. Sign in to Orris to start your own chat.