TB
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"tuberculosis"[MeSH Terms] AND "pathogenesis"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material. Let me compose the full answer.
Tuberculosis (TB) - Overview & Pathophysiology
The Organism
Mycobacterium tuberculosis (MTB) is an obligate aerobic, non-spore-forming, non-motile bacillus. Its defining feature is an unusually thick, waxy cell wall rich in mycolic acids, which:
- Makes it acid-fast (retains carbol-fuchsin dye in the Ziehl-Neelsen stain)
- Resists phagolysosomal killing
- Allows intracellular survival inside macrophages
- Enables airborne transmission via tiny droplet nuclei (1-5 µm) that reach the alveoli
The organism is classified into distinct phylogenetic lineages. "Modern" lineages 2-4 drive the global epidemic; lineage 2 strains are particularly associated with rapid drug resistance development and greater transmissibility. - Goldman-Cecil Medicine, p. 3249
Epidemiology
The WHO estimates 1.7 billion people (a quarter of the world's population) carry latent MTB infection. In 2021, approximately 1.3 million people died of TB worldwide, making it historically the leading infectious cause of death from a single pathogen (surpassed only by SARS-CoV-2 during the COVID-19 pandemic). HIV coinfection profoundly amplifies risk: HIV-positive individuals are 25-30 times more likely to develop active TB from latent infection. - Robbins Basic Pathology, p. 474; Goldman-Cecil Medicine, p. 3249
Step 1 - Infection Before Cell-Mediated Immunity (First ~3 Weeks)
When droplet nuclei are inhaled, bacilli deposit in the distal air spaces of the lower upper lobe or upper lower lobe (zones of greatest airflow). They are engulfed by alveolar macrophages via mannose receptors and complement receptor 3 (CR3). MTB then employs a critical virulence strategy:
- Phagosome maturation arrest - blocks fusion with lysosomes
- Inhibits acidification of the phagosome
- Blocks production of reactive nitrogen and oxygen species
The result is unchecked intracellular bacterial replication, leading to bacteremia with seeding of multiple sites (lungs, lymph nodes, kidneys, meninges, bone) before immunity develops. - Robbins Basic Pathology, p. 475
Step 2 - Cell-Mediated Immunity (After ~3 Weeks)
Once MTB antigens reach draining lymph nodes, dendritic cells and macrophages present them to CD4+ T cells. Under the influence of macrophage-secreted IL-12, naive T cells differentiate into Th1 cells, which then secrete IFN-γ. This is the pivotal cytokine in TB immunity.
IFN-γ activates macrophages to:
- Produce TNF-α - recruits monocytes that form the granuloma
- Upregulate iNOS (inducible nitric oxide synthase) - generates nitric oxide (NO) and reactive nitrogen intermediates that kill mycobacteria
- Produce defensins (antimicrobial peptides) toxic to MTB
- Achieve phagolysosome maturation to actually digest the bacillus
The IFN-γ / TNF / CD4 T-cell axis is so essential that defects in IL-12 signaling, IFN-γ, TNF, or NO production all result in poorly formed granulomas and disease progression. This explains why anti-TNF-α therapies (e.g. infliximab for RA/IBD) carry a black-box warning for TB reactivation. - Robbins Basic Pathology, p. 475-476
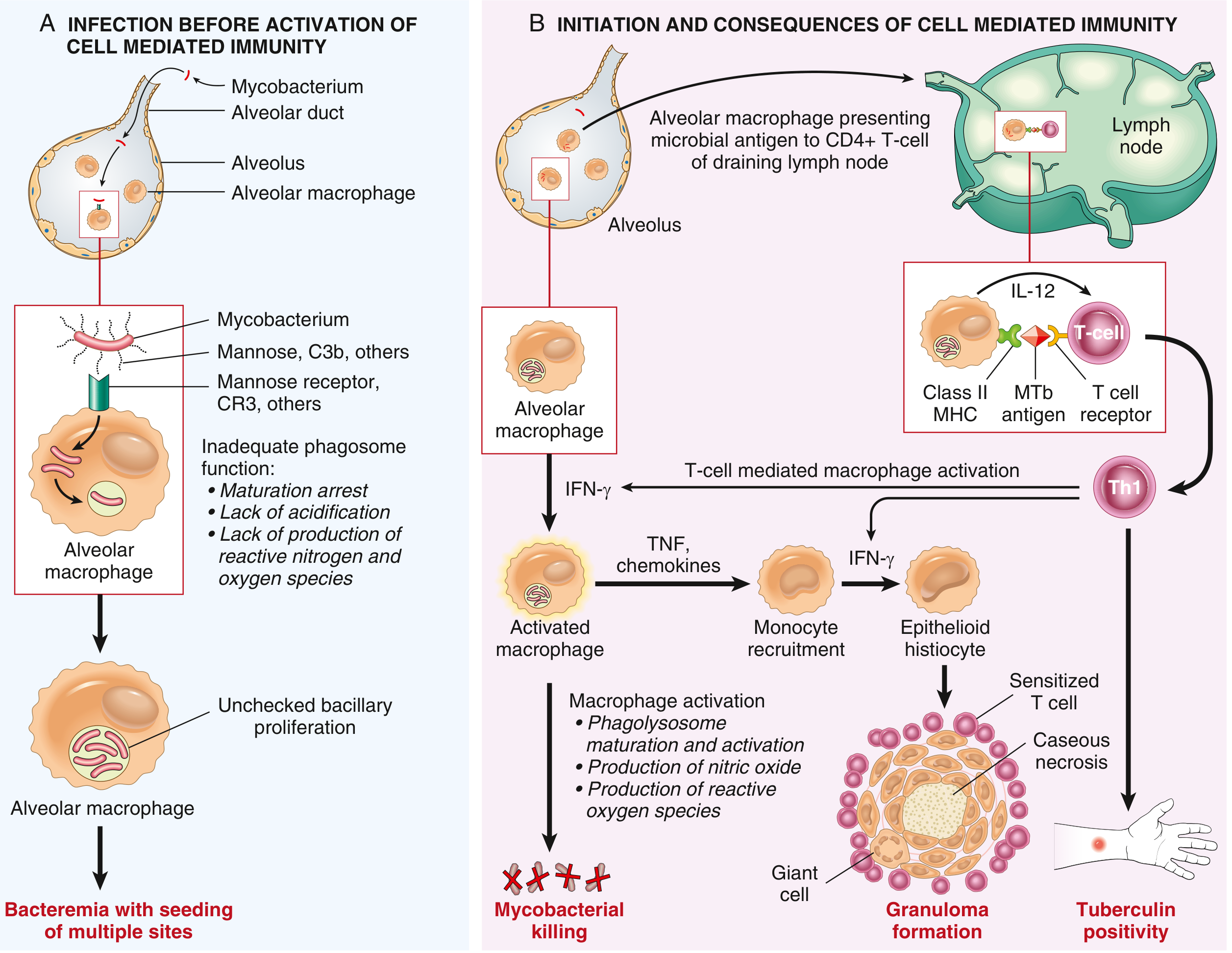
The Granuloma - Hallmark Lesion
The tuberculous granuloma (tubercle) forms when IFN-γ drives macrophages to differentiate into epithelioid histiocytes, which aggregate around the bacilli. Some fuse into Langhans-type multinucleate giant cells (nuclei arranged at periphery). Surrounding this core are sensitized T lymphocytes.
Centrally, a process unique to TB occurs: caseous necrosis - an amorphous, cheese-like coagulative necrosis with complete effacement of tissue architecture. This results from:
- Intense delayed-type hypersensitivity
- Local ischemia
- Toxic bacterial products
The caseum is largely devoid of living cells but can contain viable organisms. In immunocompetent hosts, the granuloma walls off and controls the infection. In immunocompromised hosts (HIV, malnutrition, anti-TNF therapy), granuloma formation fails and instead sheets of macrophages with unchecked bacillary growth are seen. - Robbins Basic Pathology, p. 475-476
Primary TB
Primary TB occurs in a previously unexposed, unsensitized individual. About 5% of newly infected individuals develop significant disease.
Ghon focus: A 1.0-1.5 cm gray-white area of consolidation, usually subpleural in the lower upper lobe or upper lower lobe, often with central caseous necrosis.
Ghon complex: Ghon focus + lymphangitis + regional hilar/mediastinal lymph node caseation. This triad is the hallmark of primary infection.
In ~95% of immunocompetent people, cell-mediated immunity controls infection and the Ghon complex undergoes progressive fibrosis and calcification (visible on X-ray as the Ranke complex). Despite early hematogenous seeding, no further lesions develop. - Robbins Basic Pathology, p. 474-476
Latent TB Infection (LTBI)
In the remaining ~90% who never develop active disease, MTB enters a state of dormancy. The bacteria survive within the granuloma, metabolically suppressed. Organisms may persist in:
- Macrophages
- Lymph node lymphatic endothelial cells (LECs) - recently identified reservoir
Lifetime risk of reactivation from LTBI: 5-10%. - Tietz Laboratory Medicine; Murray & Nadel's
Secondary (Reactivation) TB
Secondary TB arises in a previously sensitized host, either from:
- Reactivation of dormant primary lesions (typically decades later)
- Reinfection with a large inoculum
Characteristic location: apex of one or both upper lobes (highest oxygen tension favors aerobic MTB growth). Because hypersensitivity pre-exists, the immune response is rapid and tends to wall off the focus, so regional lymph node involvement is far less prominent than in primary TB.
Without adequate control, the caseous center liquefies (due to proteolytic enzymes), ruptures into a bronchus, is expectorated, and leaves behind a cavity. This is the basis of:
- Cavitary TB on CXR
- Infectious aerosol transmission (open TB)
- Hemoptysis (erosion into pulmonary vessels - Rasmussen aneurysm)
Secondary TB can also disseminate hematogenously to produce miliary TB (millet seed-sized granulomas throughout the body) when immune control completely fails. - Robbins Basic Pathology, p. 476-478
Summary Flowchart
Inhalation of droplet nuclei (1-5 µm)
↓
Alveolar macrophage engulfs MTB
↓
MTB blocks phagolysosome fusion → intracellular replication
↓
Hematogenous/lymphatic seeding (bacteremic phase)
↓ [~3 weeks]
IL-12 → CD4+ Th1 cells → IFN-γ
↓
Macrophage activation (iNOS, TNF, defensins)
↓
Granuloma formation with caseous necrosis
↓
┌──────────────────────────────┐
│ │
~95% Immunocompetent ~5% Immunocompromised
Ghon complex → fibrosis/ Progressive primary TB
calcification (Ranke complex) (no granulomas, sheets of
Latent TB infection bacilli-laden macrophages)
│
Reactivation risk 5-10% lifetime
↓
Secondary TB: apical cavitary disease
Key Risk Factors for Progression to Active TB
| Risk Factor | Mechanism |
|---|---|
| HIV (CD4 <200) | Depletes Th1 response |
| Anti-TNF therapy | Blocks granuloma maintenance |
| Diabetes mellitus | Impaired macrophage function |
| Malnutrition | Deficient cell-mediated immunity |
| Silicosis | Damages alveolar macrophages |
| End-stage renal disease | T-cell dysfunction |
| Age extremes | Immature/waning immunity |
- Goldman-Cecil Medicine, Table 299-1, p. 3250
This is a shared conversation. Sign in to Orris to start your own chat.