Give me everything you got about prostatic carcinoma from Robbins
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have everything from both Robbins books. Here is the complete synthesis:
Carcinoma of the Prostate - Robbins
Sources: Robbins & Kumar Basic Pathology (9780323790185) and Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
1. Epidemiology
Adenocarcinoma of the prostate is the most common cancer in men in the United States, estimated to account for ~21% of male cancers. It is the second leading cause of cancer-related death in men, behind only lung cancer. It is largely a disease of aging - autopsy incidence rises from ~20% in men in their 50s to ~70% in men ages 70-80. There is a wide spectrum of natural history, from aggressive and rapidly fatal to more commonly indolent disease of little clinical significance.
Racial disparity: African American men die from prostate cancer at a rate more than double that of European American men. The causes are not fully understood, though unequal access to screening and treatment are major contributors.
2. Anatomy and Zones
The prostate is divided into biologically distinct regions:
- Peripheral zone: 70-80% of carcinomas arise here (posterior location, palpable on rectal exam)
- Transition zone: Most benign hyperplasia arises here (causes urinary obstruction)
- Central zone and periurethral zone: Less commonly affected
The normal prostate gland contains glands with two cell layers: a flat basal cell layer and an overlying columnar secretory cell layer. This two-layer architecture is lost in carcinoma - a key histologic clue.
3. Pathogenesis
Clinical and experimental observations implicate four major factors:
Androgens
Androgens are central. Growth and survival of prostate cancer cells depend on androgens, which bind to the androgen receptor (AR) and induce expression of pro-growth and pro-survival genes. This explains why surgical or chemical castration causes tumor regression. Most tumors eventually become androgen-resistant through:
- AR gene amplification (hypersensitivity to low androgen levels)
- AR splice variants lacking the ligand-binding domain (ligand-independent activation)
- AR mutations allowing activation by non-androgen ligands
- Alternative signaling pathway activation bypassing AR entirely
Heredity
- Men with first-degree relatives with prostate cancer have a 2-fold increased risk
- BRCA2 mutations (homologous recombination repair) and DNA mismatch repair gene mutations (Lynch syndrome) increase risk of early-onset, aggressive disease
- MYC regulatory region variants increase risk
- HOXB13 transcription factor variant (role in prostatic development) confers several-fold increased risk
Environmental Factors
- Western diet (charred red meats, animal fats) associated with increased risk
- Carcinogens, estrogens, and oxidants are hypothesized to damage prostatic epithelium, driving genetic/epigenetic changes
- GSTP1 polymorphisms (glutathione-S-transferase) linked to risk - impaired detoxification of polycyclic aromatic hydrocarbons
Acquired Genetic and Epigenetic Alterations
The most common genetic alteration is a chromosomal rearrangement juxtaposing an ETS family transcription factor gene (most commonly ERG or ETV1) next to the androgen-regulated TMPRSS2 promoter - occurs in ~50% of prostate cancers, producing androgen-dependent overexpression of ETS oncogenes.
Other driver alterations:
- MYC amplification and PTEN deletion - accelerate cell growth, contribute to antiandrogen resistance
- TP53 loss (deletion/mutation) and RB deletions - common in late-stage disease
- AR gene amplifications - late-stage
- p27 silencing (CDK inhibitor) - common early event
Epigenetic silencing (DNA methylation) is also prevalent:
- GSTP1 (glutathione-S-transferase Pi 1) - one of the most frequent early events; impairs xenobiotic detoxification, enhancing genotoxicity
- RB, CDKN2A (cell cycle regulation)
- MLH1, MSH2 (genomic stability)
- APC (Wnt signaling)
4. Precursor Lesion: High-Grade Prostatic Intraepithelial Neoplasia (HGPIN)
About 80% of prostates removed for carcinoma also harbor HGPIN. HGPIN consists of architecturally benign large branching acini lined by atypical cells with prominent nucleoli that may be cytologically identical to carcinoma. Unlike carcinoma, HGPIN:
- Retains (at least partially) a basal cell layer
- Has an intact basement membrane
Many molecular changes seen in invasive cancer are already present in HGPIN, strongly supporting its precursor role.
5. Morphology
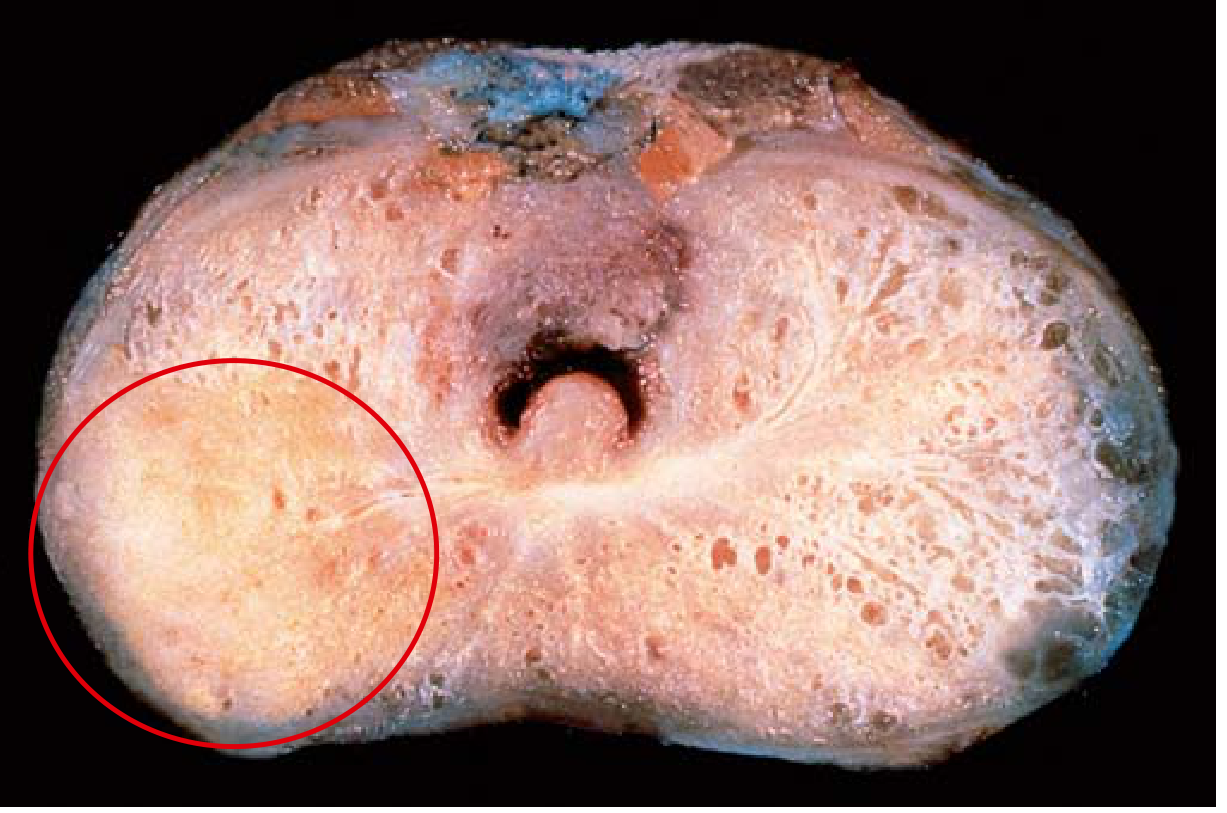
Gross appearance: In ~70% of cases, carcinoma arises in the peripheral zone (classically posterior). On cross-section, neoplastic tissue is gritty and firm, often difficult to visualize by eye. Advanced lesions appear as firm, gray-white lesions with ill-defined margins infiltrating the adjacent gland.
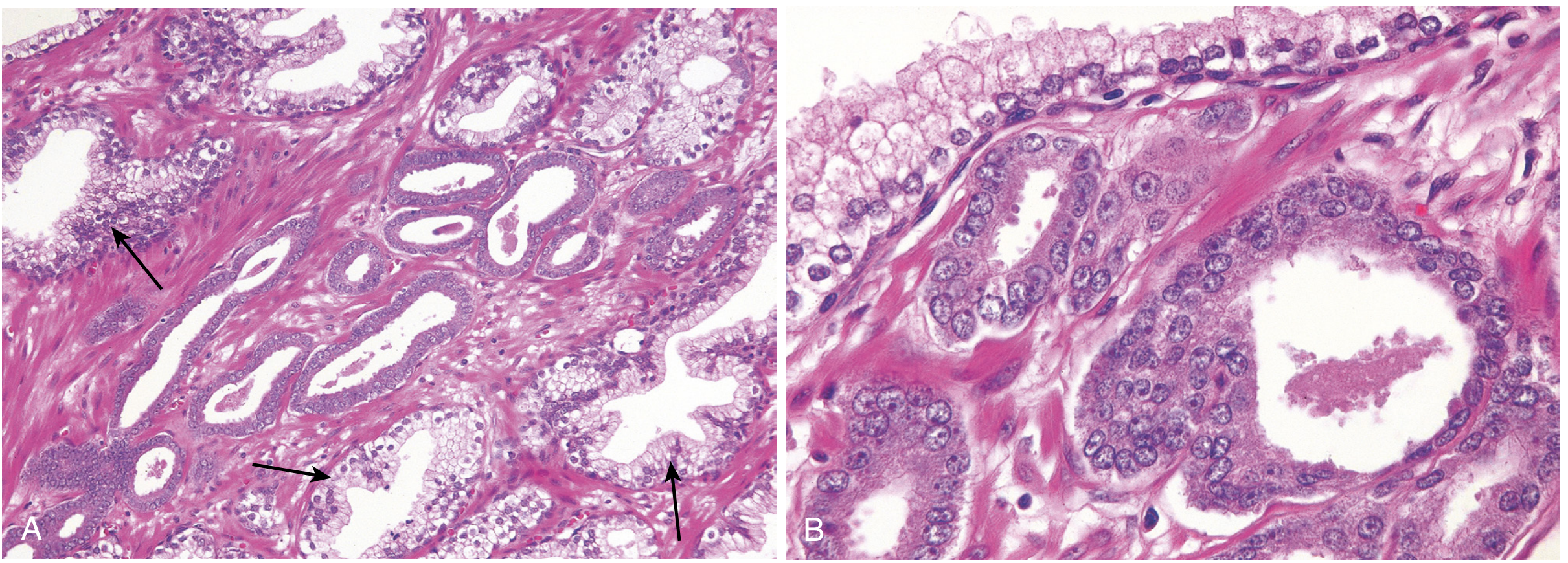
Microscopic appearance: Most are moderately differentiated acinar adenocarcinomas. Key histologic features compared to benign glands:
| Feature | Benign Glands | Malignant Glands |
|---|---|---|
| Size | Larger | Smaller, crowded |
| Basal cell layer | Present | Absent |
| Branching/papillary infoldings | Present | Absent |
| Cell layer | Two-layered | Single uniform layer |
| Nuclei | Normal | Enlarged, prominent nucleoli |
| Mitoses | Rare | Rare |
| Cytoplasm | Normal | Pale-clear to amphophilic |
Perineural invasion: A specific, diagnostically useful finding on biopsy - malignant glands wrapping around nerves.
With increasing grade: irregular/ragged glandular structures, cribriform glands, sheets of cells, or infiltrating individual cells.
Immunohistochemistry: Basal cells in benign glands can be highlighted by markers (high-molecular-weight cytokeratin, p63), which are absent in cancer. AMACR (alpha-methylacyl-CoA racemase) is positive in cancer, helpful in equivocal cases.
6. Gleason Grading System
Grading is based on glandular patterns of growth across 5 grades:
| Grade | Pattern |
|---|---|
| 1 | Most well-differentiated; uniform round glands packed into well-circumscribed nodules |
| 2 | Slightly less regular glands |
| 3 | Individual discrete glands, more variable size and spacing |
| 4 | Poorly formed, fused, or cribriform glands |
| 5 | No gland formation; tumor infiltrates in cords, sheets, solid nests |
Most tumors contain more than one pattern. A primary grade (dominant pattern) + secondary grade (second-most frequent) are added to give the Gleason score (range 2-10).
Grade Groups (contemporary system)
| Grade Group | Gleason Score | Pattern |
|---|---|---|
| 1 | ≤6 (3+3) | Only individual discrete well-formed glands |
| 2 | 3+4=7 | Predominantly well-formed glands + lesser poorly formed/fused/cribriform |
| 3 | 4+3=7 | Predominantly poorly formed/fused/cribriform + lesser well-formed |
| 4 | 4+4=8 / 3+5 / 5+3 | Only poorly formed/fused/cribriform OR mix of well-formed + lack of glands |
| 5 | 9-10 | Lack of gland formation (or necrosis) ± poorly formed/fused/cribriform |
- Most screen-detected treatable cancers: Gleason scores 6-7 (Grade Groups 1-3)
- Advanced cancers less likely to be cured: Gleason scores 8-10 (Grade Groups 4-5)
7. Staging (pTNM, AJCC 8th Edition)
| pTNM | Finding |
|---|---|
| pT2 | Organ confined |
| pT3 | Extraprostatic extension |
| pT3a | Extraprostatic extension (unilateral or bilateral) or microscopic bladder neck invasion |
| pT3b | Tumor invades seminal vesicles |
| pT4 | Fixed or invades external sphincter, rectum, bladder, levator muscles, or pelvic wall |
| Nx | Regional nodes not assessed |
| N0 | No regional nodal metastasis |
| N1 | Regional nodal metastasis |
| M0 | No distant metastases |
| M1a | Distant lymph node metastases |
| M1b | Bone metastases |
| M1c | Other distant sites |
Grade (Grade Groups) is now integrated with pTNM to derive combined prognostic groups ("upstaging").
8. Spread and Metastases
- Local invasion: Most commonly involves periprostatic tissue, seminal vesicles, and base of the urinary bladder (producing ureteral obstruction in advanced disease); may invade adjacent soft tissues, wall of urinary bladder, or (less commonly) rectum
- Lymphatic spread: Obturator nodes first, then paraaortic nodes
- Hematogenous spread: Chiefly to bones, particularly the axial skeleton
- Lumbar spine > proximal femur > pelvis > thoracic spine > ribs (order of frequency)
- Metastases are classically osteoblastic (bone-forming) - this is a distinctive feature that strongly points to prostatic origin (most other cancers cause lytic lesions)
- Detectable on radionuclide bone scan
- Extensive visceral dissemination is the exception
9. Clinical Features
Localized disease: Nearly always asymptomatic. Discovered by:
- Elevated serum PSA (most common in US)
- Palpable irregular hard nodule on digital rectal examination (due to peripheral zone location)
Advanced/locally invasive disease: Symptoms of urinary obstruction (less likely early than BPH because of peripheral location).
Metastatic disease: Bone pain, pathologic fractures, spinal cord compression.
10. PSA (Prostate-Specific Antigen)
PSA is a product of prostatic epithelium, normally secreted in semen. It is an androgen-regulated serine protease that cleaves the seminal coagulum. Only minute amounts circulate normally.
As a screening test - controversial:
- Organ-specific, NOT cancer-specific
- PSA is elevated in BPH, prostatitis, prostate infarction, instrumentation, ejaculation
- 20-40% of patients with organ-confined prostate cancer have PSA below cutoffs
- Many prostate cancers are so indolent that detection may lead to overtreatment with associated morbidity
- Large studies show PSA screening has little or no impact on reducing prostate cancer mortality
As a monitoring tool - unambiguous value:
- Serial PSA measurements after treatment (surgery or radiation) are highly valuable for detecting recurrence or disseminated disease
- Elevated PSA after radical prostatectomy = recurrent/disseminated disease
MRI in the setting of elevated PSA can help identify nonpalpable cancers.
11. Treatment
Localized, high-risk disease:
- Radical prostatectomy: Most common treatment; prognosis based on pathologic stage, margin status, and Gleason grade
- Radiotherapy: External-beam radiation or brachytherapy (radioactive seeds implanted in prostate) - excellent local control, used when patient is not a surgical candidate
- Both with or without hormonal manipulation
- >90% of patients who receive definitive therapy for localized disease can expect to live ≥15 years
Low-risk, low-volume disease (Grade Group 1):
- Genomic gene panel tests can help stratify which cancers can be followed with active surveillance alone (avoiding overtreatment)
Metastatic disease - androgen deprivation:
- Orchiectomy (surgical castration)
- Synthetic LHRH agonists (e.g., leuprolide, goserelin): Chronic administration desensitizes pituitary LHRH receptors → suppresses LH release → reduces testosterone production by Leydig cells
- Androgen deprivation induces remissions, but most tumors eventually develop androgen-independent clones → disease progression → death
12. Miscellaneous / Other Prostatic Tumors
(From Robbins & Cotran, Pathologic Basis of Disease)
- Ductal adenocarcinoma (peripheral ducts): Presents like ordinary prostate cancer; (periurethral ducts): hematuria and obstructive symptoms similar to urothelial cancer; poor prognosis
- Adenosquamous / pure squamous carcinoma: Following hormone therapy or de novo
- Colloid (mucinous) carcinoma: Abundant mucinous secretions >25% of tumor
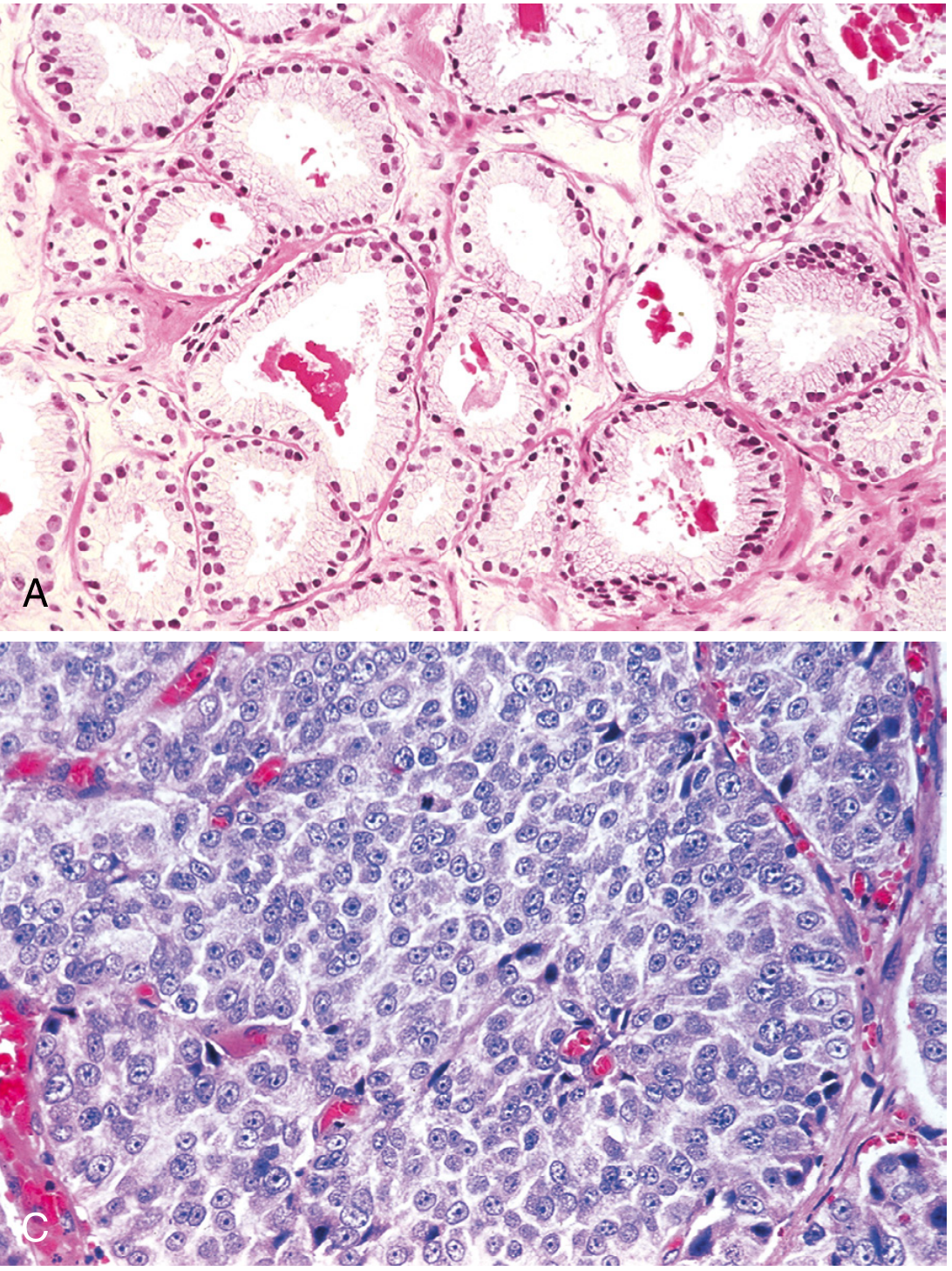
- Small-cell carcinoma (neuroendocrine carcinoma): Most aggressive variant; almost all rapidly fatal; increasingly seen as recurrent disease in patients treated with antiandrogen therapy (therapy controls conventional adenocarcinoma but provokes emergence of androgen-independent neuroendocrine subclone)
- Secondary involvement: Most common secondary tumor is urothelial carcinoma (bladder CIS extending into prostatic ducts/acini, or direct invasion)
- Stromal tumors: Unique mesenchymal tumors derived from prostatic stroma
Key Concepts Summary (Robbins & Cotran)
- Most common malignancy in US males; ranges from indolent (managed by active surveillance) to lethal
- Arises in peripheral zone, palpable on rectal exam
- Most common driver mutations: TMPRSS2-ETS rearrangements (androgen-dependent ETS overexpression, especially ERG or ETV1)
- Gleason grading strongly correlates with stage and is a strong prognosticator; compressed into Grade Groups that influence combined prognostic staging
- Most localized cancers are clinically silent, detected by PSA monitoring
- Bone metastases are classically osteoblastic
- PSA: imperfect screener (false-negatives and false-positives), but excellent for monitoring after treatment
- Treatment: surgery/radiation ± hormonal manipulation; androgen deprivation (orchiectomy or LHRH agonists) for metastatic disease
- Robbins & Kumar Basic Pathology (Robbins Pathology), pp. 660-664
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 907-910
This is a shared conversation. Sign in to Orris to start your own chat.