Describe lateral wall of nose with diagram
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the material needed for a thorough answer. Let me compile it.
Lateral Wall of the Nose
The lateral wall of the nasal cavity is the most anatomically complex wall of the nose. It carries the nasal conchae (turbinates), the openings of the paranasal sinuses, and the nasolacrimal duct.
Bony Framework
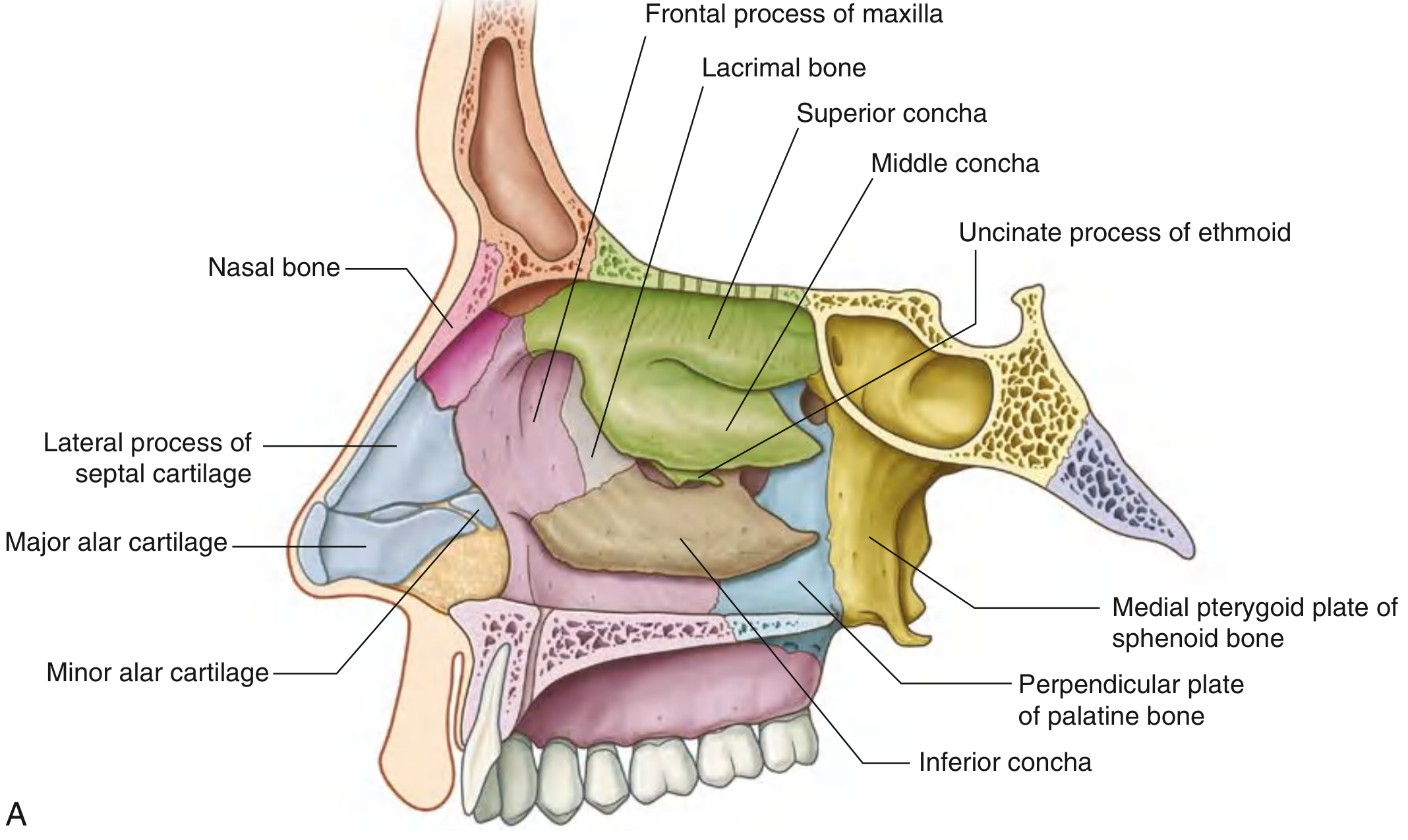
The lateral wall is formed by several bones (Fig. 8.242A):
| Component | Bone |
|---|---|
| Anterior | Nasal bone, frontal process of maxilla |
| Anterosuperior | Lacrimal bone |
| Superoposterior | Ethmoidal labyrinth (superior + middle conchae, uncinate process) |
| Inferoposterior | Perpendicular plate of palatine bone |
| Posterolateral | Medial pterygoid plate of sphenoid |
| Inferior | Inferior concha (independent bone) |
In the external nose (vestibule area), the lateral wall is supported by the lateral process of the septal cartilage and the major and minor alar cartilages, along with soft tissues.
Nasal Conchae (Turbinates)
Three curved bony shelves project medially from the lateral wall:
- Inferior concha - an independent bone (not part of the ethmoid)
- Middle concha - part of the ethmoidal labyrinth
- Superior concha - part of the ethmoidal labyrinth
- (A supreme concha may occasionally be present)
Each concha curves inferiorly at its anterior end to form a lip that overlies the anterior opening of its related meatus. The conchae do not extend into the external nose.
The turbinates are filled with vascular channels and venous sinusoids that serve to warm and humidify inspired air and regulate nasal airflow resistance. They continuously dilate and constrict every 0.5-3 hours in a normal physiological phenomenon known as the nasal cycle.
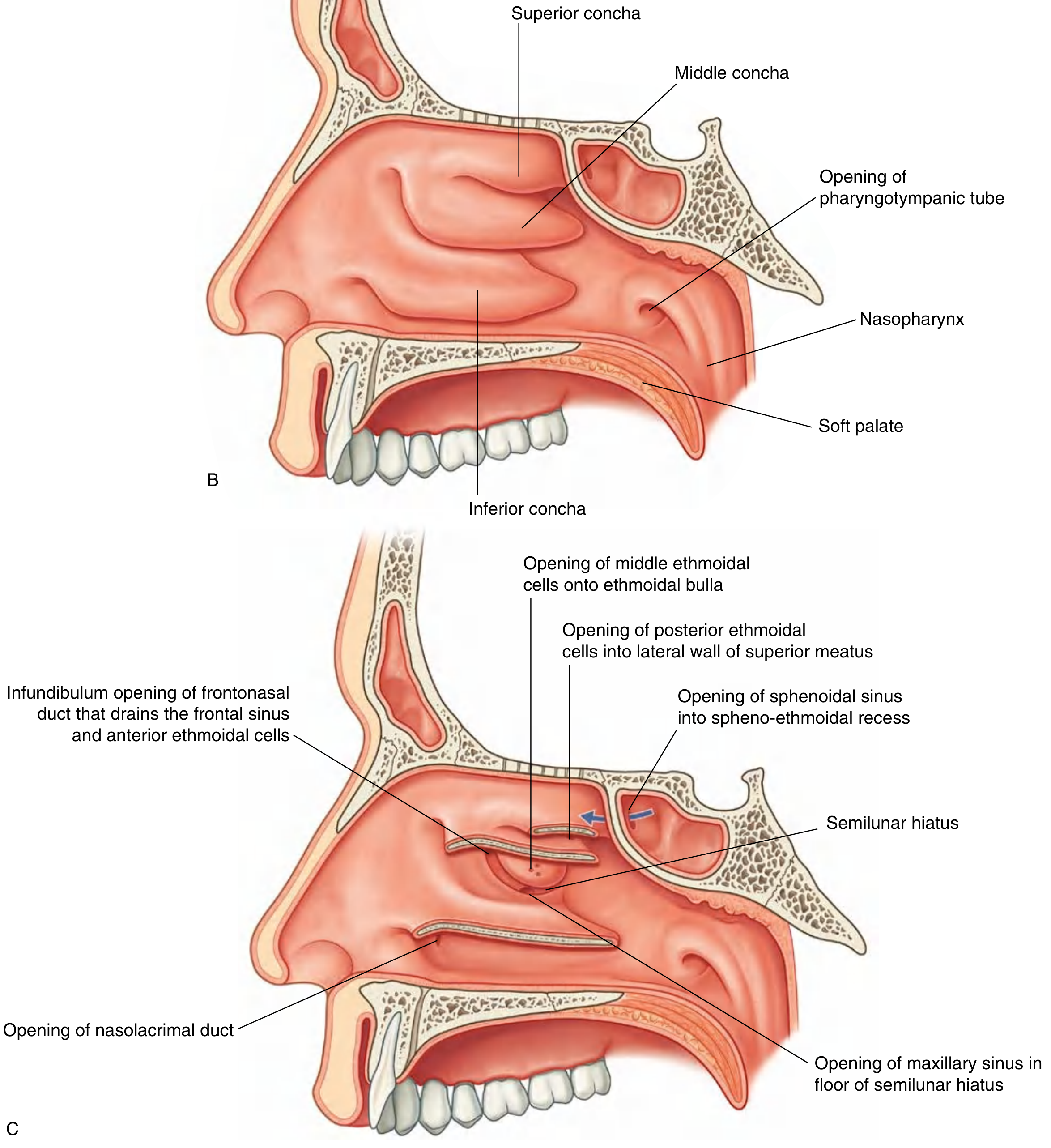
Meatuses (Air Channels)
The three conchae divide the nasal cavity into four air passages:
1. Inferior Meatus
- The largest meatus, lying between the inferior concha and the nasal floor
- Opens into it: The nasolacrimal duct, approximately 1 cm posterior to the head of the inferior turbinate - via a small mucosal fold called Hasner's valve
2. Middle Meatus
- The most clinically important meatus
- Contains the ethmoidal bulla (dome-shaped elevation formed by underlying middle ethmoidal cells) and the semilunar hiatus (a curved gutter inferior to the bulla)
- The ethmoidal infundibulum leads from the anterior end of the semilunar hiatus upward into the frontonasal duct and frontal sinus
- Opens into it: Frontal sinus (via frontonasal duct/ethmoidal infundibulum), maxillary sinus (at the floor of the semilunar hiatus), middle and anterior ethmoidal cells (on/above the ethmoidal bulla)
- The middle meatus is thus the common drainage pathway for the frontal, maxillary, and anterior ethmoid sinuses - collectively called the ostiomeatal complex (OMC)
3. Superior Meatus
- Smaller, between the superior and middle conchae
- Opens into it: Posterior ethmoidal air cells
4. Spheno-ethmoidal Recess
- The space above and posterior to the superior concha
- Opens into it: Sphenoidal sinus (the only paranasal sinus not opening onto the lateral wall proper)
Blood Supply
Both the internal and external carotid arteries contribute:
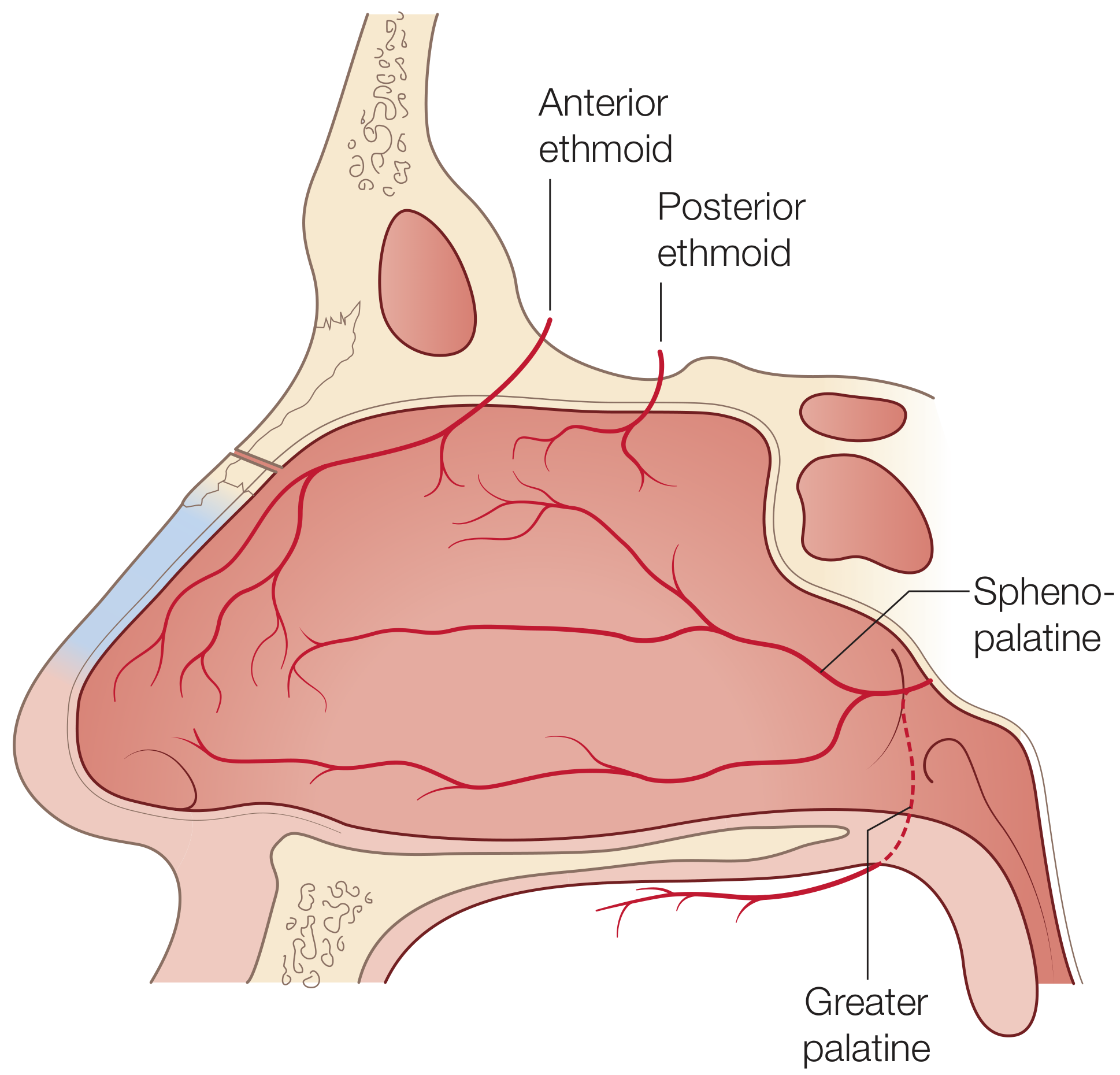
| Vessel | Origin | Area supplied |
|---|---|---|
| Sphenopalatine artery (main supply) | Internal maxillary artery (ECA) | Majority of turbinates and lateral wall; enters via sphenopalatine foramen |
| Anterior ethmoidal artery | Ophthalmic artery (ICA) | Superior lateral wall; enters via anterior ethmoidal foramen |
| Posterior ethmoidal artery | Ophthalmic artery (ICA) | Superior posterior lateral wall |
| Greater palatine artery | Internal maxillary artery (ECA) | Inferior lateral wall adjacent to palate |
| Facial artery branch | External carotid artery | Small anterior strip |
The sphenopalatine foramen (just inferior to the horizontal attachment of the middle turbinate) is the key surgical gateway for the sphenopalatine artery. The crista ethmoidalis of the palatine bone is a reliable surgical landmark for this vessel.
Nerve Supply
| Nerve | Division | Area supplied |
|---|---|---|
| Posterolateral nasal nerves | V2 (maxillary) via sphenopalatine foramen | Lateral wall and turbinates (main supply) |
| Anterior ethmoidal nerve | V1 (ophthalmic) | Superior and anterior lateral wall |
| Olfactory nerve (CN I) | Special sensory | Olfactory area of superior lateral wall |
- Secretomotor (parasympathetic): Presynaptic fibers travel in the vidian nerve (greater superficial petrosal nerve component) and synapse in the sphenopalatine ganglion to innervate nasal mucous glands
- Vasomotor (sympathetic): Postsynaptic fibers from the deep petrosal nerve pass through the sphenopalatine ganglion and regulate vascular tone and turbinate congestion
Gateways to the Lateral Wall
| Gateway | Contents |
|---|---|
| Cribriform plate (perforations) | Olfactory nerve (CN I) fibers; anterior ethmoidal nerve and vessels |
| Sphenopalatine foramen | Sphenopalatine artery; posterolateral nasal nerves from V2 |
| Anterior ethmoidal foramen | Anterior ethmoidal artery and nerve |
| Incisive canal | Nasopalatine nerve; terminal branch of greater palatine artery |
Clinical Relevance
- Ostiomeatal complex (OMC): The middle meatus and its associated drainage pathways are collectively the OMC - obstruction here leads to chronic rhinosinusitis involving the frontal, maxillary, and anterior ethmoid sinuses
- Epistaxis: The sphenopalatine artery is the most common target for endoscopic ligation in posterior epistaxis. The crista ethmoidalis is the key surgical landmark
- Turbinate hypertrophy: A common cause of nasal obstruction due to allergic or non-allergic rhinitis
- Nasolacrimal duct obstruction: Presents with epiphora; the duct opens under the anterior lip of the inferior concha
Sources: Gray's Anatomy for Students, p. 1217-1219; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, p. 1015-1016
Medial. Wall diagram and description
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have excellent material and diagrams. Let me now compile the comprehensive answer.
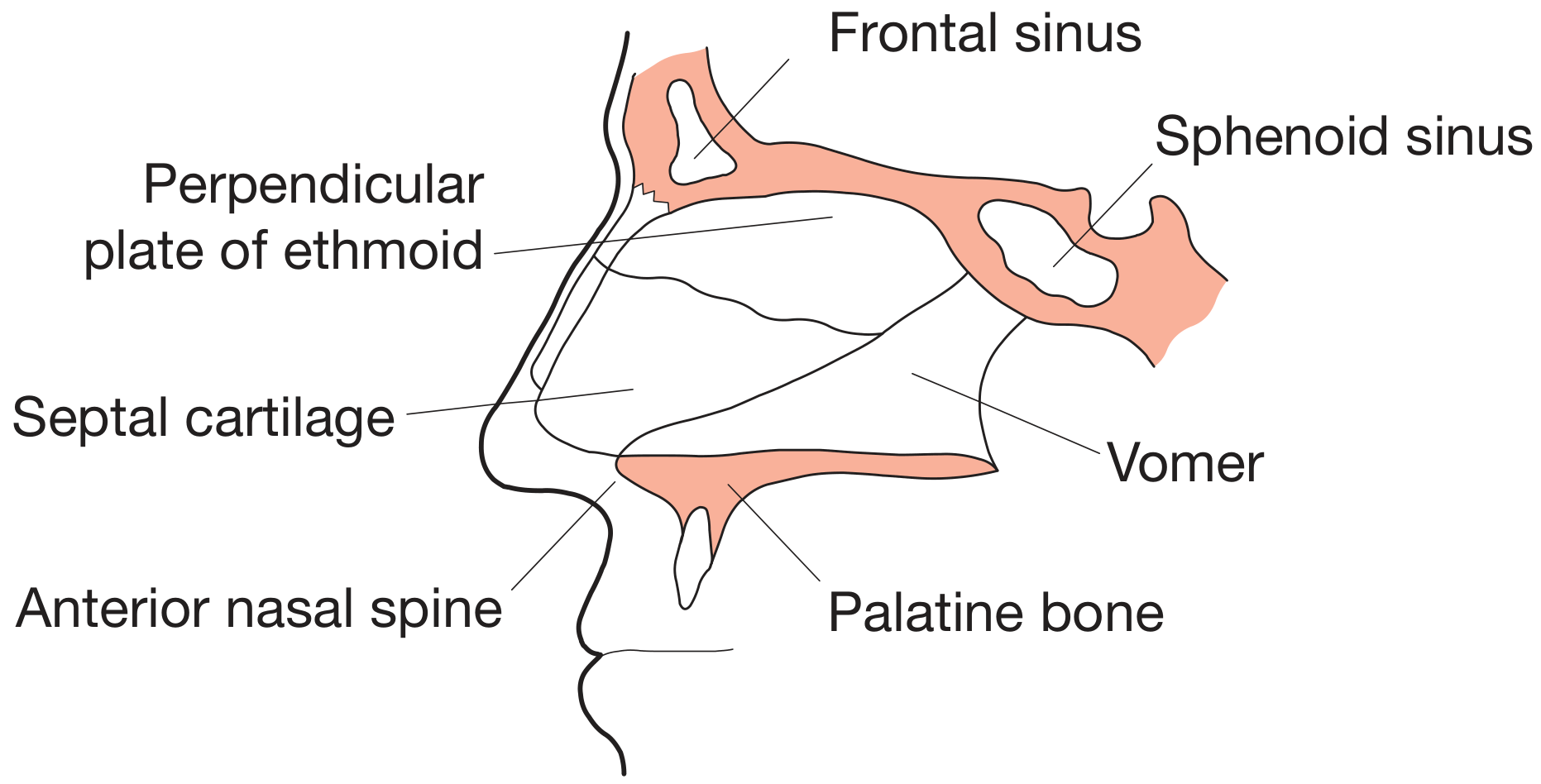
Medial Wall of the Nose (Nasal Septum)
The medial wall of each nasal cavity is formed by the nasal septum - a thin, vertically oriented partition in the median sagittal plane that separates the right and left nasal cavities.
Diagrams
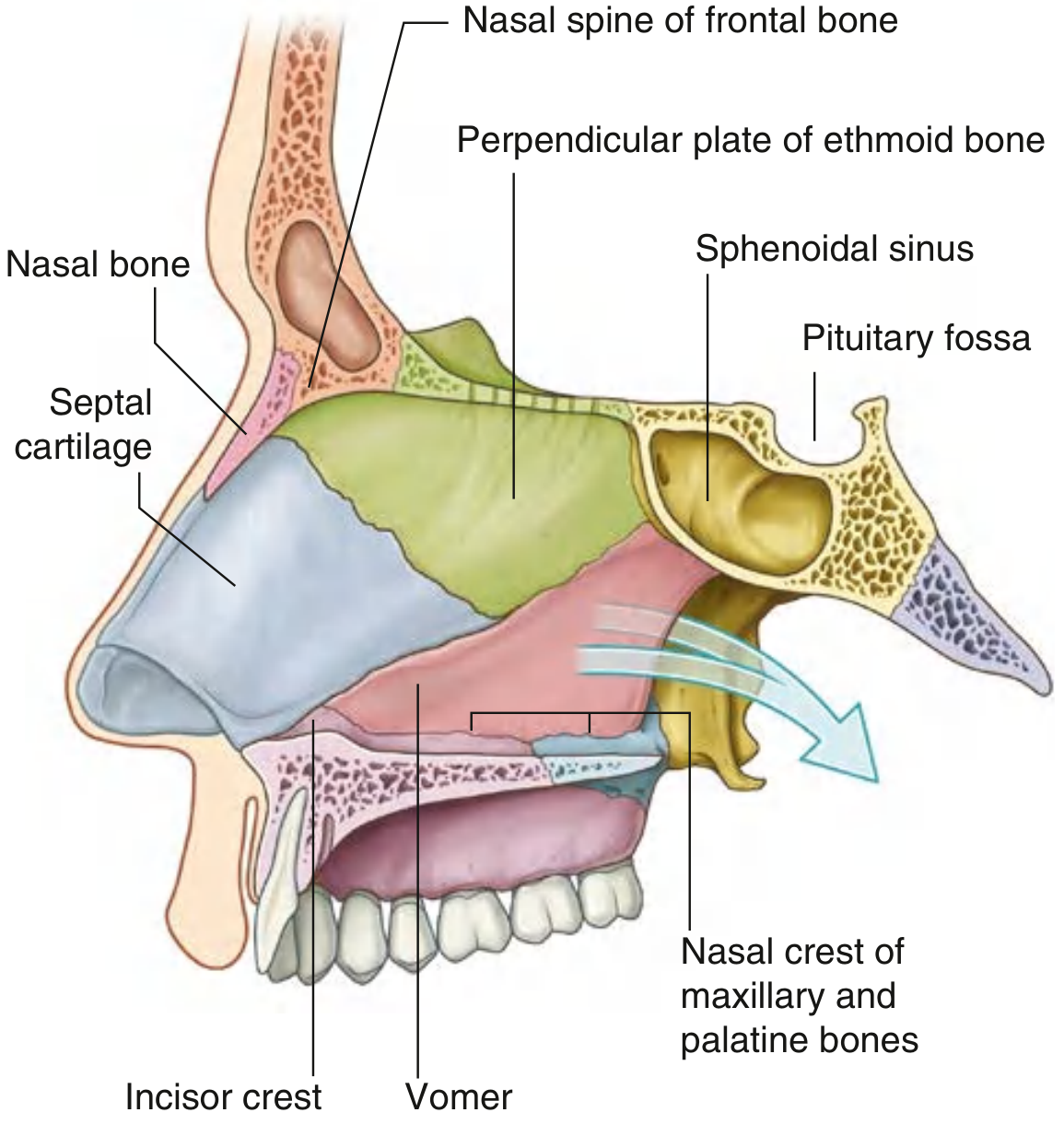
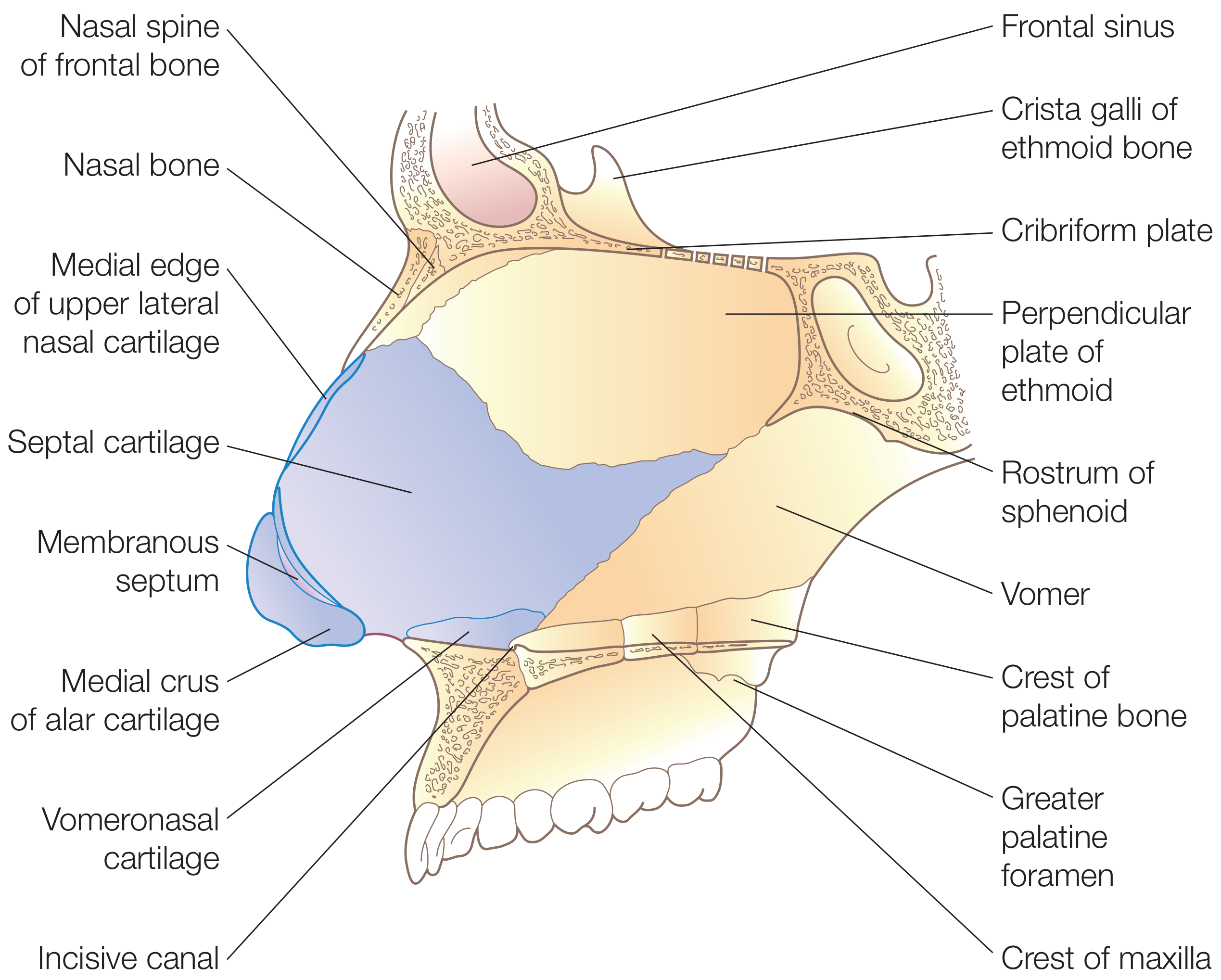
Composition of the Nasal Septum
The septum has three parts: bony, cartilaginous, and membranous.
1. Bony Part
| Component | Position | Notes |
|---|---|---|
| Perpendicular plate of ethmoid | Upper one-third | Continuous superiorly with cribriform plate and crista galli; articulates posteriorly with sphenoid crest, inferiorly with vomer, anteroinferiorly with septal cartilage |
| Vomer | Posterior and inferior | Its two alae articulate with sphenoid rostrum, forming the vomerovaginal canals (carrying pharyngeal branches of maxillary artery); inferior border sits on nasal crest of maxilla and palatine bone; posterior free edge forms the posterior septum |
| Nasal crest of maxilla + palatine bones | Inferior floor attachment | The septal cartilage and vomer rest on this crest |
| Rostrum of sphenoid | Posterior superior | Articulates with vomer alae |
| Nasal bones (midline junction) | Anterosuperior | Small contribution at midline meeting |
| Nasal spine of frontal bone | Superoanterior | Small contribution |
| Incisor crest of maxilla | Anteroinferior |
2. Cartilaginous Part
The septal (quadrilateral) cartilage forms the largest cartilaginous component:
- Bound firmly to nasal bones, perpendicular plate of ethmoid, and vomer by collagenous fibers
- Continuous with the upper lateral cartilages at the bridge of the nose
- Its sphenoidal process (septal tail) extends posteriorly between the vomer and perpendicular plate - a useful graft source during revision rhinoplasty
- Inferior attachment to the nasal crest of the maxilla is via looser connective tissue (a pseudoarthrosis), allowing mobility during trauma to reduce the risk of fracture
- Anteroinferiorly, a small vomeronasal (Jacobson's) cartilage may be present along the nasal floor
3. Membranous Part
- A small segment of connective tissue between the caudal edge of the septal cartilage and the columella
- Forms the mobile, soft lower part of the septum
Summary of Bony Framework
ANTEROSUPERIOR POSTEROSUPERIOR
Nasal spine of Perpendicular plate
frontal bone of ethmoid
↓ ↓
Nasal bone Rostrum of sphenoid
↓ ↓
Septal cartilage ←---→ Vomer (posterior + inferior)
↓
Nasal crest of maxilla + palatine bone (floor)
↓
Incisive canal
Blood Supply
Both internal and external carotid arteries supply the medial wall:
| Artery | Origin | Area supplied |
|---|---|---|
| Sphenopalatine artery (posterior septal branch) | Internal maxillary artery (ECA) | Posterior and superior septum (main supply) |
| Anterior ethmoidal artery | Ophthalmic artery (ICA) | Anterosuperior septum |
| Posterior ethmoidal artery | Ophthalmic artery (ICA) | Posterior superior septum |
| Greater palatine artery | Internal maxillary artery (ECA) | Anteroinferior septum - ascends via incisive canal |
| Superior labial artery (septal branch) | Facial artery (ECA) | Anterior inferior septum / nasal vestibule |
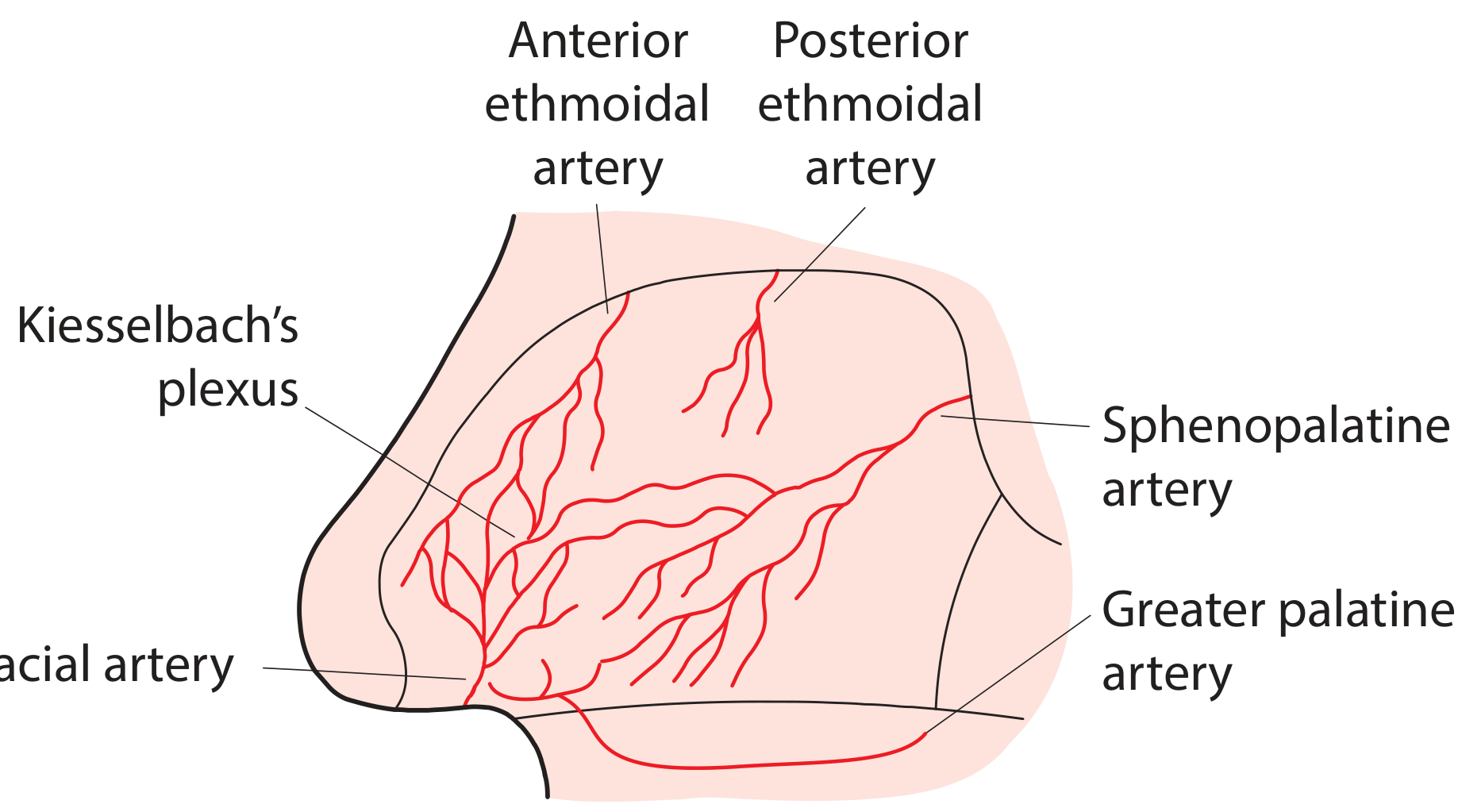
Kiesselbach's Plexus (Little's Area)
All five arteries anastomose in the anteroinferior septum to form Kiesselbach's plexus (Little's area in the UK). It lies just under a thin overlying nasal mucosa and is the most common site of anterior epistaxis. It is formed by:
- Posterior septal branch of sphenopalatine artery
- Anterior ethmoidal artery
- Greater palatine artery
- Alar branch of superior labial artery (facial artery)
Venous Drainage
- Anterior and posterior ethmoidal veins → superior ophthalmic vein → cavernous sinus
- Sphenopalatine vein → pterygoid plexus
- Facial vein
Clinical point: Because nasal veins are valveless, retrograde spread of infection to the cavernous sinus is possible - this is why nasal sepsis (especially "danger triangle" infections) can be life-threatening.
Nerve Supply
Sensory
| Nerve | Division | Area |
|---|---|---|
| Internal nasal branch of anterior ethmoidal nerve | V1 (ophthalmic) | Anterior and superior septum |
| Posterior ethmoidal nerve | V1 | Posterior septum (ethmoid and sphenoid mucosa) |
| Nasopalatine nerve (largest septal nerve) | V2 via sphenopalatine foramen | Passes forward and down the medial wall then through incisive canal to hard palate |
| Olfactory nerve (CN I) | Special sensory | Upper septum (olfactory area) |
Autonomic
| Type | Pathway | Function |
|---|---|---|
| Parasympathetic | Greater superficial petrosal nerve → vidian nerve → sphenopalatine ganglion → postsynaptic fibers | Controls nasal secretions (mucous glands) |
| Sympathetic | Sympathetic chain → superior cervical ganglion → deep petrosal nerve → vidian nerve → through sphenopalatine ganglion | Vasoconstriction; regulates turbinate congestion |
Functions of the Nasal Septum
- Divides the nasal airway into two separate nasal cavities
- Supports the nasal dorsum
- Maintains the nasal tip projection
- Forms part of the internal and external nasal valves (regulation of airflow)
- Source of cartilage graft in rhinoplasty and reconstructive surgery
Clinical Points
| Condition | Note |
|---|---|
| Deviated nasal septum | Often from direct trauma; can cause unilateral nasal obstruction; corrected by septoplasty |
| Anterior epistaxis | Most commonly from Kiesselbach's plexus; first-line: direct pressure, cautery |
| Septal haematoma | Blood collects between mucoperichondrium and cartilage; requires urgent drainage to prevent avascular necrosis of cartilage → saddle-nose deformity |
| Septal perforation | Causes crusting, bleeding, whistling; causes include cocaine use, trauma, granulomatous disease (Wegener's/GPA) |
| Cavernous sinus thrombosis | Can result from septal infection spreading via valveless veins |
Sources: Gray's Anatomy for Students, p. 1216; Scott-Brown's Otorhinolaryngology Vol. 1, p. 1013-1014; Bailey and Love's, p. 1393-1394; K.J. Lee's Essential Otolaryngology, p. 517-518
This is a shared conversation. Sign in to Orris to start your own chat.