take Cummings as source and tell about eustachian tuboplasty for atelectasis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from Cummings. Here is the full, well-structured answer:
Eustachian Tuboplasty for Middle Ear Atelectasis
Source: Cummings Otolaryngology Head and Neck Surgery
Middle Ear Atelectasis - Background
Middle ear atelectasis is thought to result mainly from longstanding eustachian tube (ET) dysfunction. One of the principle functions of the ET is ventilation of the middle ear and mastoid - intermittent opening allows gas exchange and equalization of pressure between the nasopharynx and middle ear space. Middle ear gas composition also exchanges with the mucosa via bilateral diffusion with the blood, and when the ET fails, the middle ear gas composition begins to resemble that of venous blood, driving progressive negative pressure.
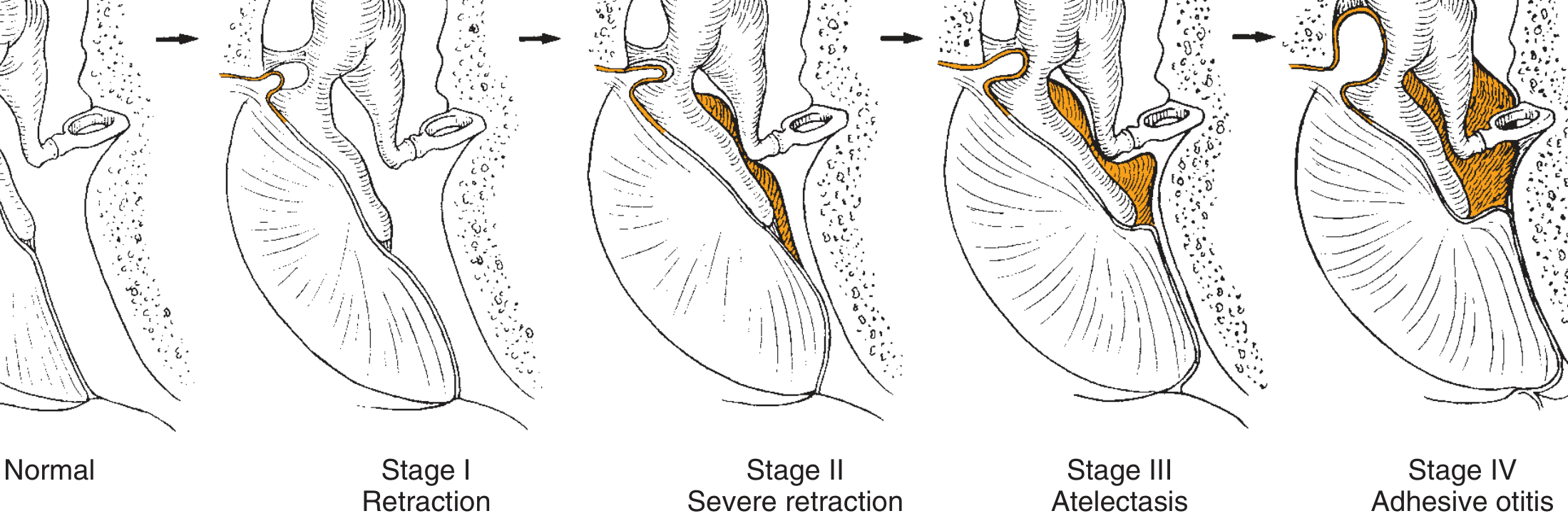
When atelectasis develops, the tympanic membrane becomes retracted onto the promontory and ossicles. The key distinction is:
- Atelectasis: middle ear space partially/completely obliterated but TM is NOT adherent to the medial wall; mucosal lining remains intact
- Adhesive otitis media: space totally obliterated, TM adherent to ossicles and promontory, mucosal surfaces lost
Sade and Berco Classification of TM Retraction (Cummings Fig. 140.3)
| Stage | Description |
|---|---|
| Stage I | Retracted tympanic membrane |
| Stage II | Retraction with contact onto the incus |
| Stage III | Middle ear atelectasis |
| Stage IV | Adhesive otitis media |
Repeated bouts of AOM weaken and thin the TM (Sade and Berco showed collagen destruction of the fibrous lamina propria), predisposing to progressive atelectasis. Not all patients with OME develop atelectasis - most retraction is limited - but deep retraction pockets (pars flaccida or pars tensa) can become cholesteatoma precursors.
Management of Atelectasis - Role of Eustachian Tuboplasty
Cummings addresses the root cause of atelectasis - obstructive ET dysfunction - and outlines tuboplasty as a definitive interventional option after medical and conventional surgical management fails.
Step 1: Address the Underlying Cause
Mucosal inflammatory disease is the most common cause. Initial management of obstructive ET dysfunction:
- Treat allergic disease (nasal antihistamines, nasal steroid sprays/rinses, immunotherapy)
- Manage laryngopharyngeal reflux (dietary measures, PPIs, H2 blockers)
- Rule out anatomic obstruction and nasopharyngeal tumor by nasopharyngoscopy
- Tympanostomy (ventilating) tubes are tried-and-true effective treatment - they bypass the ET entirely, equalizing pressure. Sade showed ventilating tubes improved atelectatic ears; Graham and Knight reported cases where atelectatic TMs were restored to normal position with nitrous oxide + tube insertion
- However, thinning of the lamina propria makes tympanostomy tube retention tenuous with early extrusion and failure - this is a key limitation driving the need for tuboplasty
Step 2: Myringoplasty / Reinforcement
When hearing loss or ossicular erosion occurs, myringoplasty for reinforcement of the atelectatic TM may be indicated (stages III-IV). Laser myringotomy has also been suggested as efficacious.
Balloon Dilation of the Eustachian Tube (Balloon Tuboplasty / BET)
This is the most established tuboplasty technique described in Cummings.
Rationale
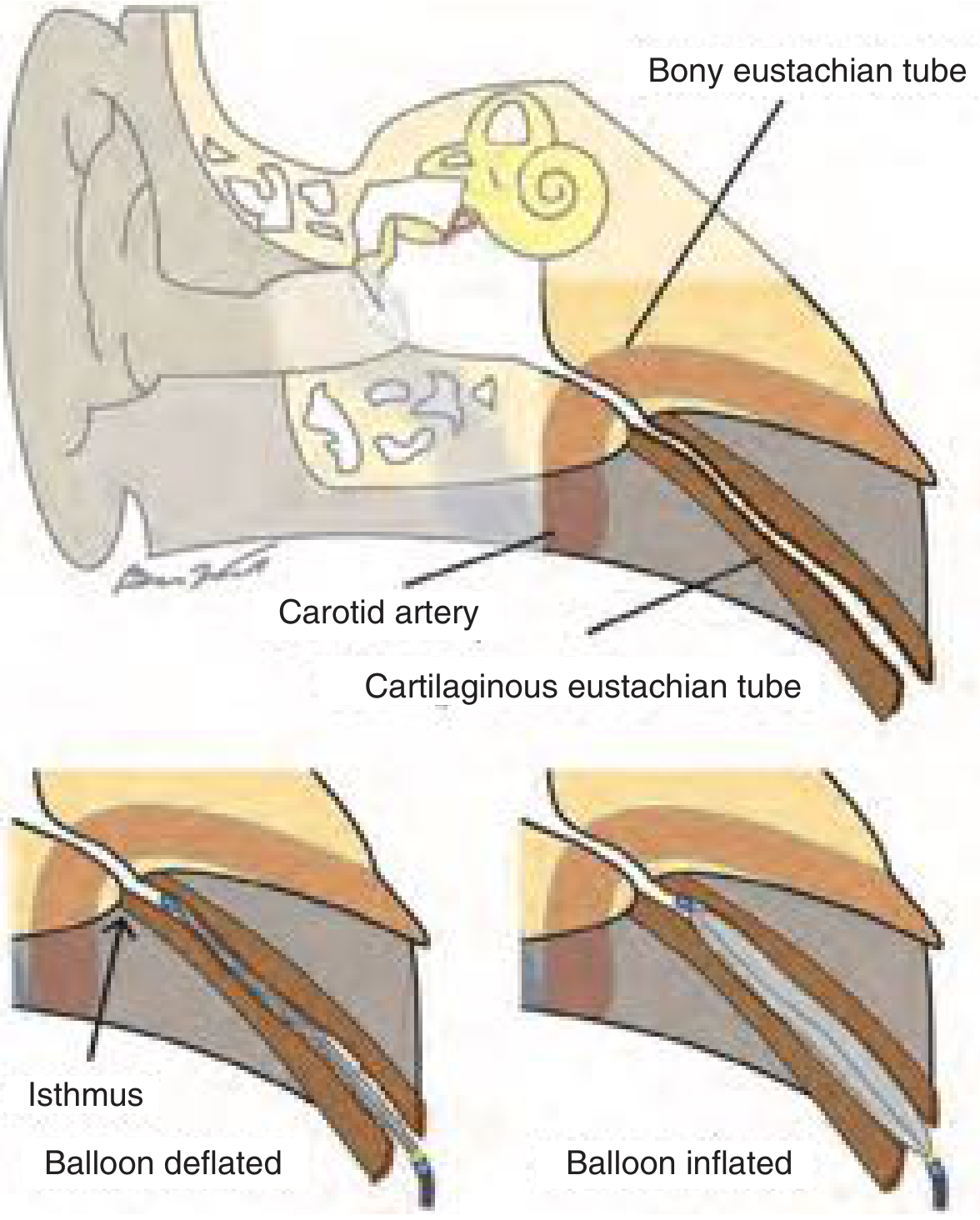
Balloon dilation has been established as a safe and effective method for treating obstructive ET dysfunction using methods analogous to sinus ostial dilation. Cadaver studies have demonstrated the ability to increase luminal diameter. Clinical studies show that the site of pathology for obstructive dysfunction is within the cartilaginous portion of the ET.
Critical Anatomical Boundary
The bony ET must NOT be entered or dilated - it comes into close proximity with the internal carotid artery, with risk of injury especially if the carotid is dehiscent into the lumen. Balloon must not advance beyond the isthmus at the bony-cartilaginous junction.
Indications (Cummings Box 131.1)
Requires both (a) and (b):
(a) All three of the following:
- Chronic symptoms of obstructive ET dysfunction (≥3 months' duration)
- Symptoms persistent despite appropriate directed medical therapy
- Objective pathologic findings on dynamic endoscopic examination (e.g., inflamed mucosa or lymphoid hyperplasia [cobblestoning] within the lumen compromising tubal opening)
(b) At least one of the following:
- Persistent OME or TM with negative pressure on insufflation AND type B or C tympanogram
- Consistent history of baro-challenge
These criteria directly encompass the atelectasis patient population - a retracted TM with negative middle ear pressure and type C tympanogram is a classic indication.
Technique
The balloon is passed transnasally into the cartilaginous ET lumen and inflated within the lumen, dilating the obstructed segment. It is specifically designed to NOT fracture bone (unlike sinus balloon dilation).
Additional Tuboplasty Techniques
Laser / Microdebrider Tuboplasty (KTP Laser): KTP (potassium-titanyl-phosphate) laser and microdebrider can target inflamed tissue at the nasopharyngeal orifice and distal lumen to decrease the bulk of inflammatory tissue. These techniques have reported success but are limited to use around the posteromedial intraluminal surface to avoid cicatricial scar formation and ET stenosis - a key safety limitation.
Summary of Treatment Ladder for Atelectasis
| Step | Treatment |
|---|---|
| 1st | Medical: allergy/reflux control, nasal steroids |
| 2nd | Tympanostomy tubes (bypass ET, restore middle ear aeration) |
| 3rd | Balloon dilation of cartilaginous ET (tuboplasty) when OME/retraction persists after medical therapy with objective ET dysfunction confirmed |
| 4th | KTP laser / microdebrider tuboplasty (ablate intraluminal inflammatory tissue at nasopharyngeal end) |
| 5th | Myringoplasty / TM reinforcement (when TM thinning is severe, hearing loss or ossicular erosion present) |
The fundamental principle is that treating atelectasis definitively requires restoring ET function - tympanostomy tubes treat the effect (negative middle ear pressure) while tuboplasty treats the cause (obstructive ET dysfunction). Balloon tuboplasty has therefore emerged as a logical complement to or replacement for repeated tube insertions in patients who recur with effusion or atelectasis.
- Cummings Otolaryngology Head and Neck Surgery, Chapter 131 (Eustachian Tube Dysfunction) and Chapter 140 (Middle Ear Atelectasis and Adhesive Otitis Media)
This is a shared conversation. Sign in to Orris to start your own chat.